
ACE 031
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
ACE-031: An ActRIIB-Fc Research Biologic With a Strong Scientific Concept and an Honest Development History
ACE-031 is not one of those molecules that comes with a loud name and nothing behind it. It is a notable ActRIIB-Fc research biologic that attracted attention because of its broad ligand-trap logic and genuine scientific interest. In experimental and early research settings, it showed a measurable signal in lean mass and muscle volume, so interest in it did not arise from elegant theory alone.
What makes its history especially valuable is its honesty: ACE-031 turned out not to be a simple "peptide trend," but a complex biologic that demonstrated both the potential of the mechanism and its limitations. For a careful client, that makes it particularly interesting — there is a strong scientific concept here, a serious development background, and a clear reason why it is still discussed today without excessive hype or fairy-tale marketing.
If what interests you is not generic solutions, but molecules with a meaningful research history and substantial biology behind them, ACE-031 is certainly worth a closer look.
ACE-031 (Ramatercept): What the Science Actually Shows
The Short Version
Imagine your muscles have a built-in speed limiter. No matter how hard you train, a protein called myostatin keeps pulling you back toward a biological ceiling your body has quietly decided on. ACE-031 — also known as ramatercept — was the most clinically advanced attempt to disable that limiter entirely. The results in early trials were genuinely impressive. The complications were, too. And understanding both sides of that story is exactly what this article is for.
| At a glance | |
|---|---|
| Other name | Ramatercept |
| What it is | Recombinant ACVR2B-Fc fusion protein |
| Molecular weight | ~100–130 kDa |
| Developed by | Acceleron Pharma + Shire Pharmaceuticals |
| What it targets | Myostatin, activin A/B, GDF-11, BMP-9, BMP-10 |
| Highest trial phase | Phase 2 (terminated) |
| Current status | Development permanently discontinued (2013) |
| WADA status | Prohibited — Section S4.3 [7] |
First Things First: ACE-031 Is Not a Typical Peptide
This is worth saying upfront, because a lot of the online conversation around ACE-031 treats it like just another research peptide. It isn’t. ACE-031 is a recombinant fusion protein — a large, engineered biological molecule weighing roughly 100 to 130 kDa. For context, common research peptides like BPC-157 weigh around 0.3 kDa. ACE-031 is hundreds of times larger, produced in mammalian cell cultures rather than by chemical synthesis, and far closer in complexity to a therapeutic antibody than to a conventional peptide. That distinction matters for almost everything: how it’s made, how it behaves in the body, what its half-life looks like, and how to think about the clinical data.
Where It Came From
The story of ACE-031 really starts in 1997, when researcher Se-Jin Lee at Johns Hopkins discovered myostatin — a protein that acts as a natural brake on muscle growth. His team found that mice without the myostatin gene grew muscles roughly twice the normal size. Soon after, similarly dramatic cases appeared in cattle and, in rare instances, in children with natural myostatin mutations. All of them had extraordinary muscle development with no apparent neurological effects. The implication was hard to ignore: if you could safely block myostatin in humans, you might be able to treat the devastating muscle wasting seen in diseases like Duchenne muscular dystrophy. That was the bet Acceleron Pharma made. Founded in Cambridge, Massachusetts in 2003, the company designed ACE-031 as a “decoy receptor.” In 2008, in collaboration with Shire Pharmaceuticals, ACE-031 entered clinical trials.
How It Works
Your skeletal muscle cells have receptors on their surface — one of them is called ACVR2B. When myostatin binds to this receptor, it triggers a chain reaction inside the cell that says: stop growing. ACE-031 is essentially a free-floating copy of that receptor, released into the bloodstream. Because it binds myostatin with greater affinity than the receptor on the cell surface, it acts as a molecular sponge — soaking up myostatin before it can deliver its “stop growing” message. The problem is that ACVR2B doesn’t just bind myostatin. ACE-031 captures a whole family of related molecules:
| Ligand captured | What it normally does |
|---|---|
| Myostatin (GDF-8) | Limits muscle growth |
| Activin A | Regulates reproduction, bone, inflammation |
| Activin B | Broad tissue regulation |
| GDF-11 | Development and metabolism |
| BMP-9 | Maintains healthy blood vessel walls |
| BMP-10 | Maintains healthy blood vessel walls |
Those last two — BMP-9 and BMP-10 — turned out to be the problem. They are essential for keeping blood vessel endothelium intact. Mutations in the BMP-9 pathway are the known cause of hereditary haemorrhagic telangiectasia, a genetic condition whose defining symptom is spontaneous nosebleeds and dilated skin vessels.
What the Clinical Trials Actually Showed
Phase 1 — Healthy postmenopausal women
The first human study enrolled 48 healthy postmenopausal women in a placebo-controlled single-dose study, with doses ranging from 0.02 to 3 mg/kg injected subcutaneously.[2] The results at the highest dose (3 mg/kg) were striking:
| What was measured | What happened |
|---|---|
| Lean body mass | +3.3% within 29 days — after a single dose |
| Thigh muscle volume | +5.1% within 29 days |
| Bone metabolism markers | Improved (an unexpected bonus finding) |
| Fat metabolism markers | Improved (another unexpected finding) |
| FSH hormone levels | Dropped by ~43% — a sign of how broadly activin signalling was suppressed |
| Tolerability | Generally fine; some injection site reactions |
One dose. Four weeks. Measurable changes in body composition. The 43% FSH drop was a quieter warning signal — it showed that the molecule was affecting hormonal systems well beyond its intended target.
Phase 2 — Boys with Duchenne muscular dystrophy
In 2010, a randomised double-blind placebo-controlled study began at multiple Canadian paediatric centres.[1] Boys with DMD on concurrent steroid therapy were enrolled across two dosing cohorts: Cohort 1 (0.5 mg/kg every 4 weeks) and Cohort 2 (1 mg/kg every 2 weeks).
| What was measured | What happened |
|---|---|
| Lean body mass | Significant dose-dependent increase; ~4–5% at 1 mg/kg |
| 6-minute walk test | Trend toward maintenance (not statistically significant) |
| Bone mineral density | Trend toward improvement |
| Fat mass | Trend toward reduced gain |
| Serious adverse events | None |
| Reason for stopping | Nosebleeds and telangiectasias (dilated skin vessels) |
In May 2013, Acceleron and Shire officially announced they would not restart the programme.[10] Development concluded permanently.
What We Know for Certain, and What We Don’t
| Confirmed by published data | Still unknown or unproven |
|---|---|
| ACE-031 increases lean mass in humans [1][2] | Long-term safety in any population |
| Increases muscle and bone in mouse models [4] | Whether functional outcomes would have improved with longer treatment |
| Broad ACVR2B ligand binding causes vascular effects [1] | Optimal dose for a hypothetical safe version of this approach |
| FSH suppression occurs with activin blockade [2] | Reproductive consequences of prolonged use |
| Black market products do not contain authentic ACE-031 [3] | Safety profile of what black market products actually contain |
The Safety Picture — Honest and Complete
The adverse events in ACE-031 trials were not random bad luck. They were a direct, mechanistically predictable consequence of what the molecule does.[1][2] The vascular side effects — nosebleeds, gum bleeding, telangiectasias, and skin redness — were attributed to cross-inhibition of BMP-9 and BMP-10, ligands essential for endothelial cell function.
| Adverse event | Why it happened | How severe |
|---|---|---|
| Nosebleeds (epistaxis) | BMP-9/10 blockade → blood vessel wall fragility | Mild to moderate |
| Telangiectasias (dilated skin vessels) | BMP-9/10 blockade → vascular remodelling | Reversible |
| Gum bleeding | Likely same vascular mechanism | Mild |
| FSH suppression | Activin A/B neutralisation affecting hormonal axis | Dose-dependent |
| Injection site reactions | Local inflammation | Mild |
How ACE-031 Compares to Similar Compounds
| Compound | Type | Status | Key difference |
|---|---|---|---|
| ACE-031 (ramatercept) | ACVR2B-Fc trap | Discontinued | Broad; binds BMP-9/10 |
| ACE-083 | FST-Fc trap | Discontinued | Local action; no BMP-9/10 binding; muscle grew but function didn’t improve |
| Bimagrumab | Anti-ACVR2B antibody | Active (obesity, metabolic disease) | Blocks receptor rather than trapping ligands |
| Apitegromab | Anti-latent myostatin antibody | Active (SMA, sarcopenia) | Much higher selectivity; targets myostatin before it’s even activated |
| Luspatercept | Modified ACVR2B-Fc | FDA-approved (β-thalassaemia, MDS) | Different ligand profile; different indication; a distinct drug |
A Bigger Lesson the Field Had to Learn
When ACE-031’s successor — ACE-083 — was designed, Acceleron made a smart fix. They engineered the new molecule to act locally at the injection site rather than systemically, and specifically avoided BMP-9/10 binding. The vascular problem was solved on paper. In a Phase 2 trial for facioscapulohumeral muscular dystrophy, MRI confirmed increased thigh muscle volume — but the trial was terminated early because there was no improvement in muscle function.[5]
The muscle grew. The patient’s ability to walk, lift, or move did not improve meaningfully. Adding muscle mass in a diseased tissue does not automatically restore the tissue’s function. Growing a larger but damaged muscle is a bit like inflating a punctured tyre — it looks better on the outside, but it doesn’t fix the underlying problem. This doesn’t mean the myostatin pathway is a dead end. It means the next generation of approaches needs to be more precise.
The Black Market Problem
A 2025 study in Drug Testing and Analysis examined 14 products sold commercially as “ACE-031.”[3] Of those 14, only 12 contained any ACVR2B-reactive protein. But none of the 12 contained the actual ACVR2B-Fc fusion protein — the molecule that was studied in clinical trials. Instead, they contained full-length activin receptor IIB: a related but fundamentally different protein.
Common Misconceptions, Addressed Directly
“ACE-031 is just another research peptide.”
It isn’t. It’s a large recombinant biological molecule closer in complexity to a monoclonal antibody than to conventional peptides. The comparison is structurally and pharmacologically misleading.
“They stopped the trials over minor nosebleeds.”
The nosebleeds and telangiectasias were symptomatic of a mechanistically serious problem — disruption of the vascular endothelium via BMP-9/10 neutralisation.[1] The concern was not the symptom itself but what it indicated about the molecule’s broader effects on blood vessel biology.
“ACE-031 proved myostatin inhibition works for DMD.”
It showed changes in body composition.[1] It did not demonstrate a statistically significant improvement in the functional outcome that matters most for DMD patients — the ability to walk and move. That distinction is critical.
“Products sold as ACE-031 contain ACE-031.”
According to independent laboratory analysis (Reichel, 2025), they do not.[3]
Frequently Asked Questions
Is ACE-031 approved anywhere in the world?
No. It has never received regulatory approval from any health authority for any indication.
Can it be used legally?
It is not an approved drug. It is explicitly prohibited under WADA Section S4.3 as a “decoy activin receptor.”[7] It is sold in some markets as a research chemical marked “not for human consumption” — a label that reflects its actual status accurately.
Are there successor drugs that work better?
Research continues. Apitegromab (Scholar Rock) and bimagrumab (Novartis) represent more selective approaches to the same biological pathway and are in active clinical development for different indications. Whether they succeed where ACE-031 did not remains to be seen.[5]
What should someone take away from this?
That the science here is genuinely interesting — and genuinely complicated. ACE-031 was not a failed experiment in the sense of producing no results. It was an experiment that produced important results, including some that the field didn’t expect and had to reckon with carefully. That’s how science is supposed to work.
References
Scientific Articles
- Campbell C, McMillan HJ, Mah JK et al. Myostatin inhibitor ACE-031 treatment of ambulatory boys with Duchenne muscular dystrophy: Results of a randomized, placebo-controlled clinical trial. Muscle & Nerve. 2017;55(4):458–464. PMID: 27462804
- Attie KM, Borgstein NG, Yang Y et al. A single ascending-dose study of muscle regulator ACE-031 in healthy volunteers. Muscle & Nerve. 2013;47(3):416–423. PMID: 23169607
- Reichel M. Gel Electrophoretic Detection of Black Market ACE-031. Drug Testing and Analysis. 2025. doi: 10.1002/dta.3898
- Suh J, Lee YS. Myostatin Inhibitors: Panacea or Predicament for Musculoskeletal Disorders? Journal of Bone Metabolism. 2020;27(3):151–165. PMC7571243
Reviews
- Nyakundi BB, Yang J. Therapeutic applications and challenges in myostatin inhibition for enhanced skeletal muscle mass and functions. Biomolecules. 2025. PMC11842502
- Rodgers BD, Garikipati DK. Clinical, agricultural, and evolutionary biology of myostatin: a comparative review. Endocrine Reviews. 2008;29(5):513–534. PMID: 18591852
Official Sources
- World Anti-Doping Agency. WADA Prohibited List 2024/2025 — Section S4.3. wada-ama.org
- ClinicalTrials.gov. NCT01099761: Phase 2 Study of ACE-031 in Boys with DMD. clinicaltrials.gov
- Muscular Dystrophy Association. Update: ACE-031 Clinical Trials in Duchenne MD. mda.org
- Acceleron Pharma / Shire PLC. Press release: Conclusion of ACE-031 collaboration. May 2, 2013.
Researcher and Institutional Profiles
- Se-Jin Lee, PhD — Johns Hopkins University. Discoverer of myostatin (1997).
- Acceleron Pharma, Inc., Cambridge, MA — original developer of ACE-031. Acquired by Merck & Co., 2021.
- Craig Campbell, MD — Western University, Ontario. Principal investigator, Phase 2 DMD trial.
- Diana Escolar, MD — Kennedy Krieger Institute, Johns Hopkins. Phase 2 co-investigator.
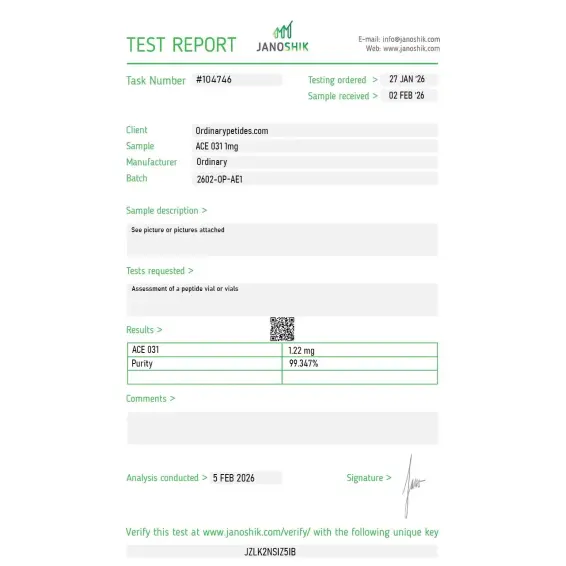
Certificate of Analysis
An independent test report is available for ACE-031. This report provides batch-level documentation and analytical verification information for research reference.

Based on 2 reviews
5.0
We use it as the broad-spectrum trap arm against more selective myostatin tools — comparing ActRIIB-Fc's multi-ligand sequestration against selective anti-myostatin approaches to map which downstream effects depend on which trapped ligand. The lack of selectivity is the experimental feature, not a flaw, since it lets us ask what the combined ligand blockade does versus single-ligand inhibition. The material held its trapping activity across our SMAD-signaling conditions.
The ligand-trap architecture is what we actually study — ACE-031 is the ActRIIB extracellular domain fused to an Fc, so it sequesters myostatin, activin, and GDF-11 by acting as a decoy receptor rather than binding a receptor itself. For probing TGF-β-superfamily ligand sequestration as a mechanism, it's a defined fusion-protein tool, and the multi-ligand trapping is the point — it's not a selective myostatin binder. The material reproduced the expected ligand-binding behavior in our SMAD-reporter assays.
It is an experimental biologic "trap" designed to bind myostatin and related molecules that normally limit muscle growth.
Yes, but not exclusively. More accurately, it is a broad ActRIIB ligand trap, rather than a strictly selective blocker of myostatin alone.
Yes. In phase I studies in healthy women, it was associated with increases in lean body mass and thigh muscle volume.
No. Only trends were observed across several measures, but no convincing clinical evidence base was established.
Because of safety signals, including epistaxis and telangiectasia; later mechanistic work linked this to non-selective effects on the BMP9/BMP10 pathway.
No. There are no reliable data indicating approval by either the FDA or the EMA.
Yes. WADA explicitly lists ACE-031 as an example of a decoy activin receptor on the prohibited substances list.
ACE-031 (also known as Ramatercept) is a recombinant fusion protein — not a traditional short-chain peptide — created by combining the extracellular domain of activin receptor type IIB (ActRIIB) with the Fc portion of human IgG1. It was developed jointly by Acceleron Pharma and Shire Pharmaceuticals with the goal of treating severe muscle-wasting conditions. It functions as a decoy receptor — circulating in the bloodstream and binding to myostatin and related muscle-suppressing proteins before they can reach actual muscle cell receptors. It received FDA orphan drug status in 2010 for Duchenne Muscular Dystrophy but its clinical development program was permanently discontinued in 2013.
ACE-031 acts as a soluble decoy for ActRIIB receptors. Myostatin (GDF-8) and other TGF-β superfamily members — including activin A, GDF-11, and related growth differentiation factors — normally bind to ActRIIB receptors on muscle cells and signal them to suppress growth. ACE-031 intercepts these ligands in circulation before they reach the cells, effectively neutralizing multiple muscle-suppressing signals simultaneously. This broader blockade — covering not just myostatin but the entire ActRIIB ligand family — was what made ACE-031 more potent than single-target myostatin antibodies, but also what contributed to its off-target safety issues.
In Phase 1 trials in healthy postmenopausal women, a single dose of ACE-031 at 3 mg/kg produced statistically significant increases in total lean body mass of 3.3% and thigh muscle volume of 5.1% at 29 days, alongside improvements in bone and fat metabolism biomarkers. In Phase 2 trials in boys with Duchenne Muscular Dystrophy, early results showed increases in lean muscle mass and promising improvements in mobility. These were genuinely impressive results — but the trials were halted in early 2011 due to safety concerns, and in May 2013 Acceleron and Shire permanently ended the entire ACE-031 development program.
Participants in the DMD trials developed several unexpected adverse events — nosebleeds, gum bleeding, and telangiectasia (small dilated blood vessels visible in the skin). These suggested that ACE-031 was interfering not only with myostatin but with activin A and other TGF-β ligands that play important roles in vascular integrity and endothelial function. Additional concerns included significant drops in follicle-stimulating hormone (FSH) levels in females, and theoretical risks of cardiac muscle hypertrophy — the heart being a muscle that could also be affected by unrestrained ActRIIB blockade. The adverse events were not individually life-threatening but their biological implications — that the compound was disrupting vascular biology in unpredictable ways — were serious enough to end the program permanently.
ACE-031 has no approved therapeutic use anywhere in the world and its pharmaceutical development is permanently discontinued. It is banned by WADA and most major sporting organizations. A 2025 study in Drug Testing and Analysis examining black market ACE-031 products found that of 14 products tested, none actually contained the genuine ACVR2B-Fc fusion protein — instead containing the full-length activin receptor 2B without the Fc fragment, meaning black market products are not only dangerous but also likely chemically inauthentic.
Clinically documented side effects include nosebleeds, gum bleeding, telangiectasia, injection site reactions including redness and swelling, decreased FSH levels in women, and headache. Theoretical longer-term risks include cardiac hypertrophy from unregulated cardiac muscle growth, disruption of bone metabolism, reproductive hormone interference, and potential effects on any tissue where ActRIIB ligands play regulatory roles. The fact that its mechanism is non-selective for myostatin — hitting the entire ActRIIB ligand family — makes its systemic effects both broader and more unpredictable than more targeted compounds.
Everyone. ACE-031 has no approved human therapeutic indication, its clinical development was permanently terminated due to safety concerns, its black market versions are likely counterfeit and uncharacterized, and it is banned in competitive sport. It should not be used by anyone outside of a strictly controlled, institutionally approved research setting. People with cardiovascular conditions, hormonal disorders, vascular abnormalities, or bleeding tendencies face particular risk given the documented adverse event profile.





