


Adipotide / FTPP
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Adipotide / FTPP: A Vascular-Targeting Peptidomimetic With an Unusual Concept and a Vivid Preclinical Signal
Adipotide / FTPP is not just another "weight-loss peptide," but a rare research peptidomimetic built on a far more unusual idea: in preclinical models, it was studied as a targeted agent aimed at the vasculature of white adipose tissue. That is exactly what makes it compelling. Instead of the usual discussion about appetite control or "boosting metabolism," the concept here was to intervene directly in the vascular support system of fat tissue — and in published animal studies, that approach was indeed associated with a marked reduction in white fat mass and body weight.
It sounds almost like science fiction, except with a laboratory badge and a very serious expression. At the same time, the value of Adipotide today does not lie in grand promises, but in its status as a strong research concept — one that produced a vivid preclinical signal, yet never made it into clinical practice.
For a careful client, that makes the molecule not a "magic solution," but a genuinely meaningful object of interest: complex, unusual, and clearly far from mass-market. If the goal is to look at the peptide space more deeply than standard marketing language allows, Adipotide is exactly the kind of case that is worth a closer look.
Adipotide (FTPP): A Scientific Review of the Fat-Targeting Proapoptotic Peptidomimetic
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Adipotide — also known as FTPP (Fat-Targeted Proapoptotic Peptide) or Prohibitin-Targeting Peptide 1 (TP01) — is one of the most mechanistically unusual compounds in obesity research. It doesn’t suppress appetite. It doesn’t rev up metabolism. It does something far more direct: it seeks out the blood vessels feeding white fat tissue and causes them to self-destruct, starving fat cells of their nutrient supply.
In obese mice, this produced roughly 30% body weight reduction over four weeks.[1] In obese rhesus monkeys, it produced rapid fat loss and improved insulin resistance.[2] Then a Phase I human trial was initiated — and eventually discontinued, primarily due to kidney toxicity concerns.[8] The compound has not been approved anywhere and is no longer in active clinical development. That arc — remarkable animal data, real safety problems, discontinued human development — is the story of Adipotide.
| At a glance | |
|---|---|
| Other names | FTPP, Prohibitin-TP01, TP01, Prohibitin-targeting peptide 1 |
| Full sequence | CKGGRAKDC-GG-D(KLAKLAK)₂ |
| Molecular formula | C₁₁₁H₂₀₄N₃₆O₂₈S₂ |
| Class | Synthetic bipartite peptidomimetic |
| Primary targets | Prohibitin (PHB) and Annexin A2 (ANXA2) on white adipose vasculature |
| Developed by | Wadih Arap and Renata Pasqualini, MD Anderson Cancer Center / Baylor College of Medicine |
| Highest trial phase | Phase I (registered; discontinued ~2019) |
| Regulatory status | Not approved; not an authorised drug anywhere |
| Development status | Discontinued |
Where It Came From
The origins of Adipotide lie not in obesity research, but in cancer biology. In the late 1990s and early 2000s, researchers Wadih Arap and Renata Pasqualini at MD Anderson Cancer Center were exploring a concept called vascular zip codes — the idea that blood vessels in different tissues carry unique molecular addresses on their surface. They used a technique called combinatorial phage display — essentially a massive molecular library screen conducted inside living animals — to identify peptide sequences that selectively home to specific vascular beds.[5]
The discovery that changed direction: a cyclic peptide sequence, CKGGRAKDC, was found to selectively target endothelial cells within the vasculature of white adipose tissue. The molecular address it recognised was prohibitin — a protein expressed on the inner wall of blood vessels feeding white fat, but not prominently expressed on vessels supplying other tissues. The prohibitin-binding motif was chemically fused to the D-enantiomer D(KLAKLAK)₂ sequence, an amphipathic peptidomimetic that disrupts mitochondrial membranes upon receptor-mediated cell internalisation and causes targeted apoptosis. The result was Adipotide — which targeted the vasculature of white adipose tissue and resulted in approximately 30% weight reduction in obese mice over a period of four weeks.[1]
Structure: Two Functional Halves
Adipotide is a bipartite peptidomimetic — two distinct functional units joined by a short glycine linker (GG). Each half has a specific job.
| Domain | Sequence | Function |
|---|---|---|
| Homing peptide | CKGGRAKDC (cyclic) | Binds to prohibitin and annexin A2 on white adipose vasculature |
| Glycine linker | GG | Connects the two domains; provides flexibility |
| Proapoptotic domain | D(KLAKLAK)₂ | Disrupts mitochondrial membranes; triggers apoptosis once internalised |
The D-enantiomer designation in the proapoptotic domain is significant: using D-amino acids (mirror images of the natural L-forms) makes the sequence highly resistant to proteolytic degradation by the body’s enzymes, extending its biological activity. The cyclic structure of the homing domain improves receptor binding affinity and stability compared to linear peptide sequences.
How It Works: The Mechanism
Think of Adipotide as a two-stage guided weapon. Stage one is navigation; stage two is detonation.
Stage 1 — Navigation: After systemic administration, the CKGGRAKDC homing domain circulates and binds selectively to prohibitin and annexin A2 (ANXA2) expressed on the surface of endothelial cells lining blood vessels that supply white adipose tissue. An annexin A2-prohibitin receptor system targeted by adipotide has been reported in the white adipose tissue vasculature of human patients[5] — suggesting the molecular target exists in humans, not just animal models.
Stage 2 — Apoptosis: Once bound, the peptide is internalised into the endothelial cell. The D(KLAKLAK)₂ domain then disrupts mitochondrial membrane integrity, triggering programmed cell death (apoptosis) in those specific endothelial cells.
The downstream consequence: Without blood vessel supply, the surrounding white adipocytes are deprived of oxygen and nutrients. They undergo ischaemic stress and subsequently die — a process called ischaemic apoptosis. The dead tissue is then cleared by the immune system.
Why it doesn’t affect brown fat or other tissues: Brown adipose tissue has a different vascular molecular profile. The prohibitin-ANXA2 receptor system targeted by Adipotide appears enriched specifically in white adipose vasculature, giving the compound its tissue selectivity. This is not absolute — the degree of selectivity and the potential for off-target vascular effects were among the unresolved questions in the clinical programme.
An additional mechanism — fatty acid transport: Beyond vascular targeting, research indicates that the PHB-ANXA2 complex also participates in fatty acid transport into adipocytes, interacting with the fatty acid transporter CD36. Adipotide may therefore also modulate lipid uptake directly — though this is a secondary and less well-characterised mechanism compared to the vascular apoptosis pathway.[6]
Preclinical Data: What the Animal Studies Showed
The preclinical story for Adipotide is genuinely striking — and also represents the best evidence available, given that no human efficacy data was published.
Mouse studies
Proapoptotic peptide completely reversed high-fat diet-induced obesity in mice and reduced body weight in mice and rats on a high-fat diet but not in those on a low-fat diet.[4] Fat loss occurred with no change in energy expenditure but with reduced food intake — occurring without signs of illness and despite reduced circulating leptin and reduced hypothalamic POMC gene expression, indicating that the decrease in food intake was independent of the action of leptin. The observation that Adipotide only worked in animals on a high-fat diet — not lean animals — suggests some selectivity for pathologically expanded fat depots. The appetite suppression effect, occurring independently of leptin, was unexpected and its mechanism remains incompletely understood.
A separate study found that metabolic improvements in glucose tolerance appeared within days of treatment, before significant fat mass reduction had occurred — suggesting direct metabolic effects beyond simply reducing adipose mass.[3]
Primate studies — the landmark 2011 paper
Treatment with adipotide induced targeted apoptosis within blood vessels of white adipose tissue and resulted in rapid weight loss and improved insulin resistance in obese monkeys. Magnetic resonance imaging and dual-energy x-ray absorptiometry confirmed a marked reduction in white adipose tissue.[2] After 28 days of treatment followed by 28 days of observation, obese rhesus monkeys showed approximately 11% body weight reduction and 39% reduction in white adipose tissue volume. Insulin resistance improved significantly. The primary side effect was relatively mild, predictable, and reversible renal injury and altered tubular function.
| Study | Model | Key finding | Source |
|---|---|---|---|
| Kolonin et al. 2004 [1] | Obese mice | ~30% body weight reduction over 4 weeks via targeted vascular apoptosis | Nature Medicine |
| Kim et al. 2010 [3] | Obese mice and rats | Complete reversal of diet-induced obesity; reduced food intake; glucose tolerance improved before weight loss | Diabetes |
| Barnhart et al. 2011 [2] | Obese rhesus monkeys | ~11% body weight loss; ~39% white fat reduction; improved insulin resistance; reversible renal effects | Science Translational Medicine |
The Human Clinical Trial
In May 2012, a Phase I clinical trial was initiated at MD Anderson Cancer Center (NCT01262664),[8] sponsored by Arrowhead Research Corporation. This was a first-in-man study.
Study design: Single cycle of Adipotide (subcutaneous daily injection for 28 days) in a narrow patient population — obese men (BMI >30) with metastatic castrate-resistant prostate cancer for whom standard treatments were not an option. Five dose levels were planned, with three patients per level. Starting dose: 0.03 mg/kg daily. The population was deliberately chosen for both scientific and ethical reasons: prostate cancer outcomes are worsened by obesity (and prohibitin is expressed in prostate cancer vasculature), so the trial could simultaneously assess weight-related effects and oncological safety.
What happened: The trial was registered through 2019, at which point it was listed as terminated. No peer-reviewed results from this trial have been published as of April 2026. Clinical development was not continued. The primary reason cited for discontinuation was nephrotoxicity — kidney toxicity — which had already been flagged as the key safety concern in primate models.
Safety: The Kidney Problem
This is the most critical section of the article for understanding why Adipotide did not progress to approval. The mechanism of Adipotide’s renal toxicity is not fully characterised, but the leading hypothesis relates to the proapoptotic D(KLAKLAK)₂ domain. After adipose vascular apoptosis occurs, peptide fragments may reach the kidney during clearance. The kidney’s filtration system — particularly the proximal tubular cells — may be vulnerable to mitochondrial disruption from these fragments, causing tubular injury.
In primate models, the kidney effects were described as reversible and manageable within the doses studied.[2] The challenge for human development was the therapeutic window: the margin between a dose that achieves meaningful fat loss and a dose that causes unacceptable kidney damage. The emergence of highly effective, well-tolerated GLP-1 receptor agonists (semaglutide, tirzepatide) substantially raised the bar for any competing obesity compound to clear.
| Safety concern | Evidence source | Severity assessment |
|---|---|---|
| Renal tubular injury / nephrotoxicity | Primate models (Barnhart 2011) [2] | Reversible in animals; unresolved in humans |
| Off-target vascular apoptosis | Theoretical; receptor specificity not absolute | Unknown magnitude in humans |
| Long-term tissue remodelling effects | Not characterised | Unknown |
| Effects on lymphatic vasculature | Not systematically studied | Unknown |
| Human safety profile overall | No published Phase I results | Essentially unknown |
What Is Confirmed and What Remains Unknown
| Confirmed by published data | Not established or unknown |
|---|---|
| Prohibitin and ANXA2 receptor system exists in human white adipose vasculature [5] | Whether Adipotide achieves meaningful fat loss in humans |
| ~30% body weight reduction in obese rodent models [1] | Human safety profile at any dose |
| ~11% body weight loss and ~39% fat reduction in obese primates [2] | Therapeutic window in humans |
| Improved insulin resistance in primate models [2] | Long-term effects on vascular architecture and tissue |
| Reversible renal injury in primates at studied doses [2] | Whether renal effects are acceptable at effective doses in humans |
| Glucose tolerance improved before fat loss in mice [3] | Mechanism of appetite suppression independent of leptin |
Potential Research Applications Beyond Obesity
Oncology: Prohibitin is expressed in vasculature of several tumour types, including prostate, breast, and ovarian cancers.[5] The ligand-directed vascular targeting concept could theoretically be adapted to deliver cytotoxic or imaging agents to tumour vasculature — using the same homing principle but different payloads. This remains a research concept, not an established therapy.
Vascular biology research tool: Adipotide has value as a research tool for studying white adipose tissue vasculature, angiogenesis in obesity, and the role of the prohibitin-ANXA2 receptor system in metabolic disease — independent of any therapeutic application.[6]
Metabolic disease research: The observation that glucose tolerance improved before significant fat mass reduction occurred — and via mechanisms apparently independent of leptin — points toward direct metabolic signalling effects that are not fully understood and merit investigation.[3]
Comparison with Other Fat-Loss Approaches
| Compound / Approach | Mechanism | Clinical status | Key difference from Adipotide |
|---|---|---|---|
| Adipotide (FTPP) | Vascular apoptosis in white fat | Discontinued | Direct physical destruction of fat vasculature |
| Semaglutide (Ozempic/Wegovy) | GLP-1 receptor agonist; appetite and metabolism | FDA-approved | Central and metabolic; no vascular apoptosis |
|
Tirzepatide (Mounjaro) |
GLP-1 + GIP dual agonist | FDA-approved | Hormonal mechanism; extensive human data |
| Tesamorelin | GHRH analogue; stimulates GH | FDA-approved (HIV lipodystrophy) | Hormonal; validated; narrower indication |
| TNP-470 / angiostatin | Non-selective angiogenesis inhibitors | Research only | Not fat-specific; broader vascular effects |
| Follistatin / myostatin inhibitors | Muscle/fat ratio modulation | Research / limited approval | Different target; affects muscle-fat balance |
Common Misconceptions
“Adipotide was proven safe in monkeys, so it’s probably safe in humans.”
Primate models are more predictive than rodent models, but they are not a guarantee of human safety. The renal effects observed in primates were described as reversible at studied doses[2] — but whether that holds across the range of doses needed for meaningful human weight loss, and in people with varying baseline kidney function, was never established in published trials.
“The Phase I trial produced results.”
No peer-reviewed results from NCT01262664 have been published.[8] The trial’s termination was recorded but detailed findings have not been released in the scientific literature as of April 2026.
“Adipotide only targets fat — it’s perfectly selective.”
The selectivity is real but not absolute. The prohibitin-ANXA2 receptor system is enriched in white adipose vasculature, but prohibitin is expressed in other contexts too. Whether the compound’s effects are genuinely confined to fat tissue vasculature in humans — and whether renal clearance of breakdown products causes off-target damage — were open questions that were not resolved.
“It’s been discontinued because Big Pharma suppressed it.”
The documented explanation is more straightforward: nephrotoxicity concerns, an uncharacterised therapeutic window, and a pharmaceutical landscape that shifted dramatically when GLP-1 agonists demonstrated excellent efficacy and acceptable safety in large human trials.
“The 30% weight loss in mice means 30% in humans.”
Rodent-to-human translation in obesity research is notoriously unreliable. The primate data (~11% body weight reduction)[2] is more relevant — and even that cannot be directly extrapolated to humans without clinical trials.
Frequently Asked Questions
Is Adipotide approved anywhere?
No. It has never received regulatory approval from any health authority for any indication.
Was it ever tested in humans?
A Phase I trial was registered (NCT01262664)[8] and reportedly initiated in 2012 in obese prostate cancer patients. No results have been published. The trial was terminated and clinical development discontinued around 2019.
What stopped clinical development?
Kidney toxicity (nephrotoxicity) identified in primate models was the primary concern.[2] The therapeutic window — the margin between effective and toxic doses — was not established to a degree that would support continued human development, particularly given the competitive landscape with GLP-1 agonists.
Is there ongoing research?
Academic research interest in the prohibitin-ANXA2 vascular targeting concept continues — particularly in oncology and vascular biology[6][7] — but Adipotide as a clinical anti-obesity drug is not in active development as of April 2026.
Is it sold as a research chemical?
Yes, by various vendors. As with many discontinued research compounds, it circulates in the research chemical market marked “not for human consumption.” Published human safety data does not exist, meaning there is no evidence base for assessing risk in human use.
How does it compare to semaglutide?
Mechanistically, they are entirely different. Semaglutide suppresses appetite and modulates metabolism through GLP-1 receptor signalling — a hormonal mechanism with extensive human trial data and FDA approval. Adipotide physically destroys fat-feeding blood vessels — a vascular mechanism with impressive animal data[1][2] and no published human evidence. In practical terms, semaglutide is a validated drug; Adipotide is a discontinued research compound.
Key Takeaways
- The mechanism is genuinely novel. No approved obesity therapy works by destroying adipose vasculature. The prohibitin-ANXA2 receptor targeting concept represents a distinct biological approach with real scientific credibility.
- The animal data was impressive — particularly in primates.[2] Rapid, significant fat loss with measurable metabolic improvements in non-human primates is a meaningful finding.
- The safety problem was real and unresolved. Kidney toxicity in primate models was not a minor footnote — it was the central barrier to human development, and it was never overcome.
- No human efficacy or safety data has been published. Everything about Adipotide’s potential in humans remains extrapolation from animal models.
- Clinical development is permanently discontinued. The compound is not in active pharmaceutical development. The competitive landscape with approved GLP-1 agonists makes a revival unlikely without fundamental redesign to address the renal safety issue.
- Academic research interest continues — not for Adipotide as an anti-obesity drug, but as a platform for understanding vascular targeting in adipose tissue and oncology.[6][7]
References
Key Scientific Articles
- Kolonin MG, Saha PK, Chan L, Pasqualini R, Arap W. Reversal of obesity by targeted ablation of adipose tissue. Nature Medicine. 2004;10(6):625–632. doi: 10.1038/nm1048. PMID: 15152612
- Barnhart KF, Christianson DR, Hanley PW, et al. A peptidomimetic targeting white fat causes weight loss and improved insulin resistance in obese monkeys. Science Translational Medicine. 2011;3(108):108ra112. doi: 10.1126/scitranslmed.3002621. PMC3666164
- Kim DH, Sartor MA, Bain JR, et al. Rapid and weight-independent improvement of glucose tolerance induced by a peptide designed to elicit apoptosis in adipose tissue endothelium. Diabetes. 2012;61(9):2299–2310.
- White JD, Gase G, Arap W, Pasqualini R, Bhatt DL. Peptide designed to elicit apoptosis in adipose tissue endothelium reduces food intake and body weight. International Journal of Obesity. 2013;37(12):1572–1579. PMC2844838
- Staquicini FI, Cardó-Vila M, Kolonin MG, et al. Vascular ligand-receptor mapping by direct combinatorial selection in cancer patients. Proceedings of the National Academy of Sciences. 2011;108(46):18637–18642. doi: 10.1073/pnas.1114503108. PMID: 22049339
Reviews
- Fang Y, Kaszuba T, Imoukhuede PI. Systems biology will direct vascular-targeted therapy for obesity. Frontiers in Physiology. 2020;11:831. doi: 10.3389/fphys.2020.00831. PMID: 32760294
- Smith TL, Sidman RL, Arap W, Pasqualini R. Targeting vascular zip codes: from combinatorial selection to drug prototypes. In: The Vasculome. Academic Press; 2022:393–401.
Official Sources and Regulatory Records
- ClinicalTrials.gov. NCT01262664: A First-in-Man, Phase I Evaluation of a Single Cycle of Prohibitin Targeting Peptide 1 in Patients With Metastatic Prostate Cancer and Obesity. Registered December 2010; terminated 2019. clinicaltrials.gov
- Wikipedia. Prohibitin-targeting peptide 1. en.wikipedia.org
Researcher and Institutional Profiles
- Wadih Arap, MD, PhD — David H. Koch Center, MD Anderson Cancer Center, University of Texas; Rutgers Cancer Institute of New Jersey. Co-discoverer of Adipotide.
- Renata Pasqualini, PhD — Co-developer of the vascular zip code / phage display approach; MD Anderson Cancer Center / Rutgers Cancer Institute of New Jersey.
- Mikhail G. Kolonin, PhD — University of Texas Health Science Center, Houston. Key contributor to early Adipotide obesity research.
- Arrowhead Research Corporation — Sponsor of Phase I clinical trial NCT01262664 (2012).
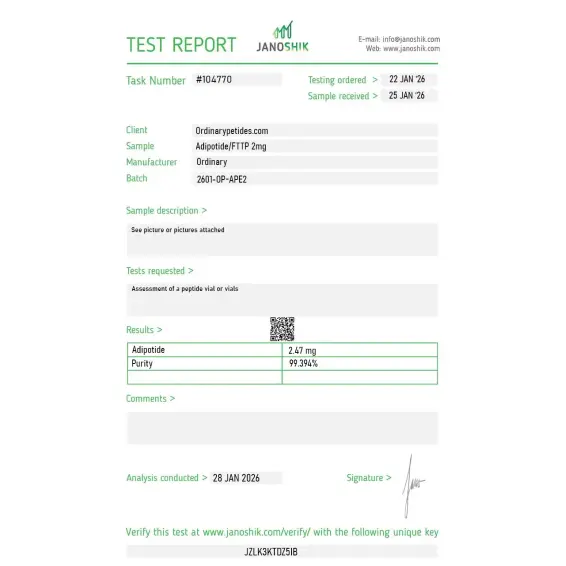
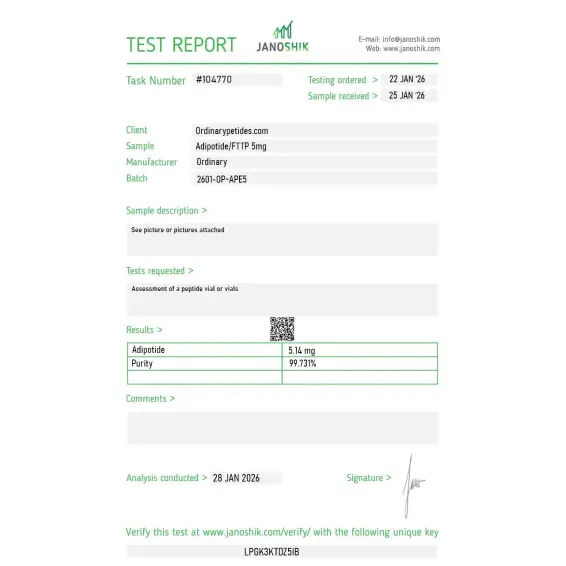
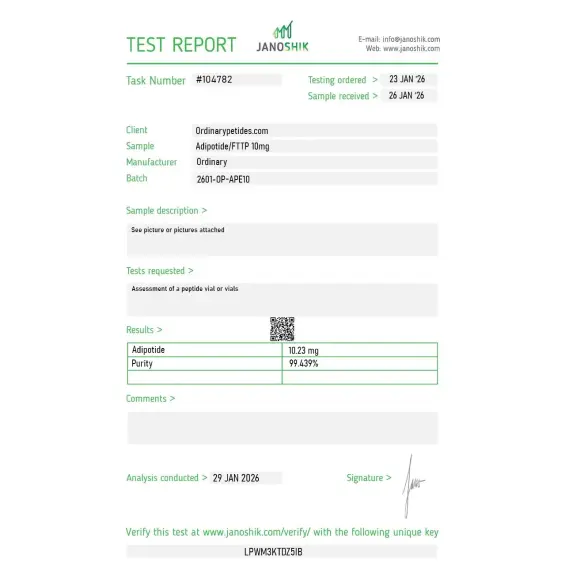
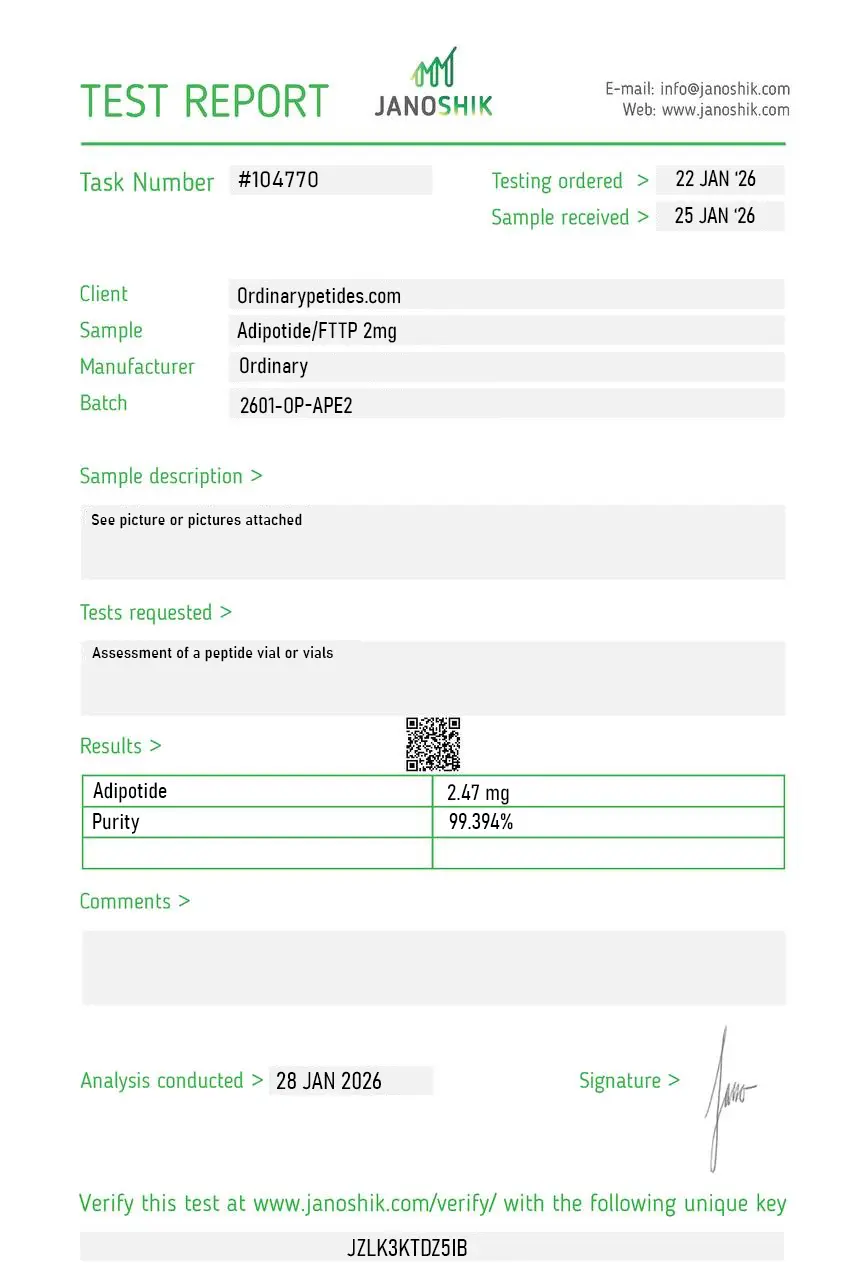
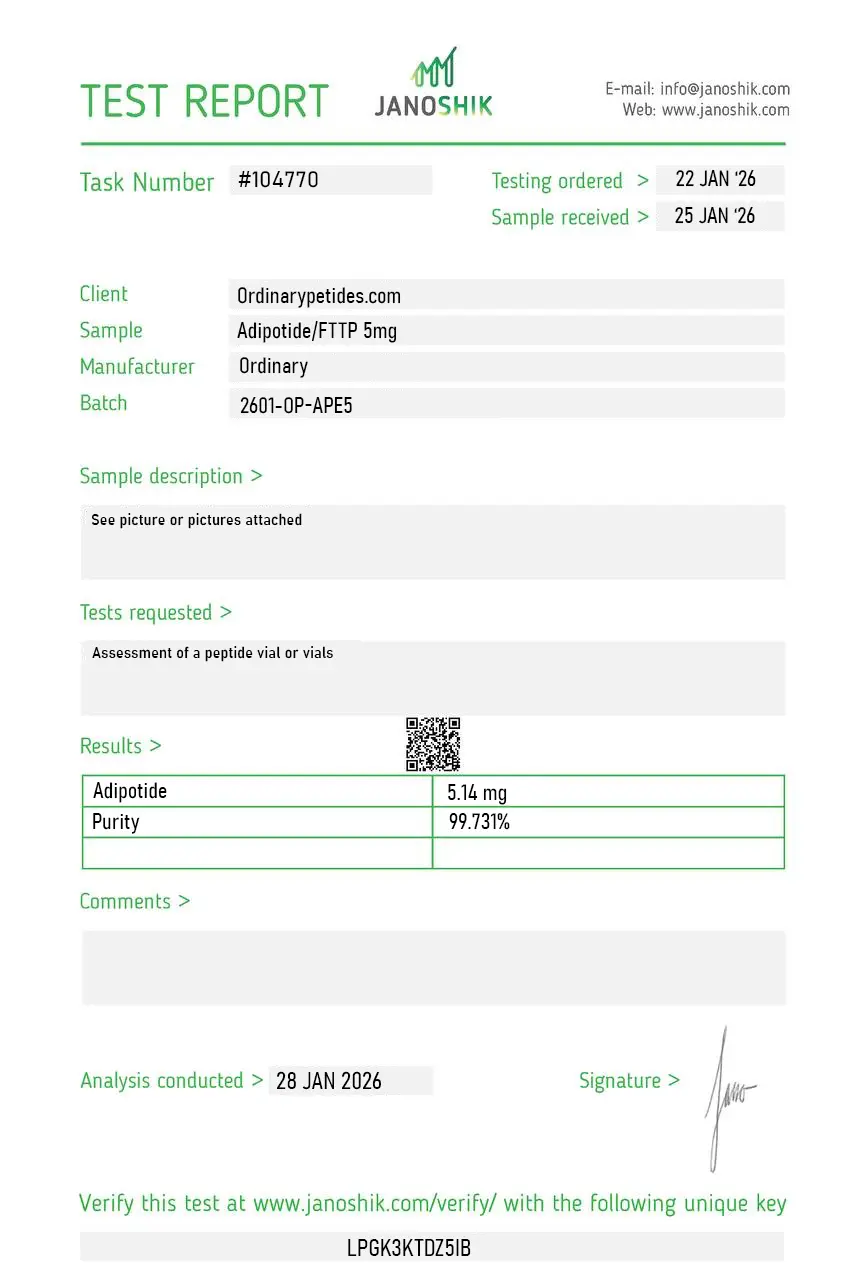
Certificate of Analysis
Independent test reports are available for Adipotide / FTTP 2mg, 5mg, and 10mg batches. These reports provide batch-level documentation and analytical verification information for research reference.

Based on 2 reviews
5.0
We work the conditional-cytotoxicity design itself — KLAKLAK is the interesting half, a cationic amphipathic D-peptide that's inert in serum but disrupts mitochondrial membranes once internalized, so lethality is gated entirely by the homing domain's delivery. Adipotide is a textbook instance of that gate-and-payload logic. The material performed predictably in our internalization-dependent apoptosis readouts, which is precisely the behavior the architecture is supposed to produce.
The reason this sits in our freezer is the targeting motif, not the warhead — CKGGRAKDC was a phage-display hit for prohibitin on the adipose vascular endothelium, and we study homing-sequence specificity across tissue-vascular addresses. Adipotide is a clean worked example of how a display-derived peptide gets weaponized into a construct. We use it to benchmark our own homing candidates' binding, and the material gave reproducible endothelial-binding signal.
Adipotide (also known as FTPP — Fat-Targeted Proapoptotic Peptide — or Prohibitin-targeting peptide 1) is a synthetic peptidomimetic compound with the sequence CKGGRAKDC-GG-D(KLAKLAK)₂. It was developed by researchers Dr. Renata Pasqualini and Dr. Wadih Arap at the MD Anderson Cancer Center, originally in the context of cancer research. Unlike every other fat-loss compound covered in this series — which works through appetite suppression, metabolic stimulation, hormone modulation, or lipolysis — Adipotide operates through an entirely unique vascular destruction mechanism that directly eliminates the blood supply to white fat tissue.
Animal studies have reported potential kidney stress markers and systemic toxicity at certain dosages. It requires strict laboratory supervision and careful dose control.
It is a prohibitin-targeting research compound composed of a vascular-binding motif linked to a mitochondrial-disrupting sequence, studied primarily in adipose tissue models.
Adipotide does not act like GLP-1 receptor agonists or appetite suppressants. Instead, it targets adipose tissue vasculature in experimental models and is not an approved clinical weight-loss medication.
Peptides vary widely in safety profiles. Experimental peptides may lack long-term human safety data, can cause off-target effects, and may carry regulatory and quality-control risks if not sourced appropriately.
It is an experimental peptidomimetic that attempts to reduce white adipose tissue by damaging the blood vessels that feed it through a predesigned molecular "address."
Yes. FTPP is one of its working labels (fat-targeted proapoptotic peptide). The names prohibitin-TP01 and TP01 are also used.
More accurately, it should be called a research-stage targeted peptide / peptidomimetic directed against white adipose tissue. The label "weight-loss peptide" oversimplifies the story and hides its cytotoxic mechanism.
Yes. According to published data, it did so in mice, rats, and obese rhesus macaques.
No. There is no convincing published clinical evidence base for human efficacy.
In preclinical work, the main limitation was renal toxicity, especially tubular injury.
No. It remains an investigational agent.
Because its preclinical story was exceptionally striking and offered an unusual route to obesity treatment through the vasculature of white fat. It is a good example of how a strong idea can fail to reach practice because of translational and safety problems.
Adipotide / FTPP is one of the most interesting and at the same time one of the most instructive peptide anti-obesity developments of the past decades. It showed that white adipose tissue can indeed be attacked through its vascular infrastructure, and in preclinical work this produced impressive weight loss and metabolic improvement. But that very "strength of mechanism" also made the project difficult to translate clinically: renal toxicity, lack of a convincing human efficacy base, and halted development prevent Adipotide from being regarded as a proven treatment for obesity. The most honest formulation is this: it is a strong research concept, but not a successful clinical solution.
Adipotide is a two-domain molecule. The first domain — CKGGRAKDC — is a homing peptide that selectively binds to prohibitin and annexin A2, proteins found specifically on the surface of endothelial cells lining blood vessels that supply white adipose tissue. The second domain — D(KLAKLAK)₂ — is a proapoptotic sequence that disrupts mitochondrial membranes upon cellular internalization, triggering programmed cell death. Once the homing peptide guides the compound to fat tissue vasculature, the proapoptotic domain kills those endothelial cells, collapsing the blood vessels feeding the fat. Deprived of oxygen and nutrients, the white adipocytes undergo ischemic injury and die — an irreversible process — and are then cleared by the immune system. Crucially, prohibitin expression appears selective to white fat vasculature and tumor vasculature, meaning brown fat and healthy non-adipose tissue are theoretically spared.
Results in animal models were striking. In obese mice, Adipotide produced approximately 30% reduction in body weight over 4 weeks. In a landmark 2012 study published in Science Translational Medicine — a highly credible journal — obese rhesus monkeys treated daily for 4 weeks showed an average 11% reduction in body weight and 39% reduction in fat deposits. Insulin resistance improved significantly. An unexpected secondary finding was that treated animals also spontaneously reduced food intake, suggesting an indirect appetite-regulating effect possibly mediated through adipokine changes. Importantly the researchers noted that the primary documented side effect was mild, predictable, and reversible renal injury — a finding they considered manageable in the context of the drug's efficacy.
Adipotide has never entered human clinical trials. It is not FDA-approved and is not approved by any regulatory authority worldwide. It is banned by WADA. Research interest from the original team has continued at a preclinical level, and the compound remains a research-only agent. The annexin A2-prohibitin receptor system targeted by Adipotide has since been confirmed in white adipose tissue vasculature of human patients, which maintains its theoretical translational relevance — but the gap between primate results and human trials has never been bridged.
It is administered by subcutaneous injection in animal studies, with research protocols typically running up to 4 weeks. No standardized human dosing protocol exists. It is available as a lyophilized research peptide reconstituted with bacteriostatic water, sold exclusively for laboratory research use.
The most significant documented side effect in animal studies is renal toxicity — kidney tubular injury and altered tubular function observed at higher doses. The researchers described this as mild, predictable, and reversible in primate studies, but the degree of renal risk in humans is entirely unknown. Other reported effects in animal studies include fatigue, mild dehydration, nausea, headache, and vomiting. The irreversible nature of its mechanism — permanently destroying fat tissue vasculature — is itself a profound concern, as any off-target effects on non-adipose vasculature could not be undone. The fact that prohibitin is also expressed on tumor vasculature raises theoretical oncological interaction concerns that have not been characterized.
Given the complete absence of human safety data, anyone with kidney disease or reduced renal function should consider this compound particularly dangerous. People with active cancer, cardiovascular disease, or vascular abnormalities face unknown and potentially serious risks. Pregnant or breastfeeding women should not use it. The irreversible cellular destruction mechanism means that any adverse event from Adipotide cannot be reversed — unlike most compounds where stopping the drug stops the effect. This makes it categorically more dangerous than most experimental peptides from a risk management perspective.





