





DSIP
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
DSIP (Emideltide): An Enigmatic Neuropeptide With Real Scientific Intrigue and an Honestly Unresolved Story
DSIP, also known as emideltide, is one of the more enigmatic peptides in sleep research. In earlier studies, it was examined as a possible factor linked to delta sleep, and small human observations described effects on sleep, daytime functioning, and several related parameters. It sounds almost like a relic from vintage neurophysiology, and that is precisely part of its appeal.
Yet the central intrigue is that the elegance of the story still outweighs the strength of the modern evidence base: a 2006 review described DSIP as a "still unresolved riddle." In the published literature, it appears less as a clinically established and fully resolved therapeutic story, and more as an investigational neuropeptide with intriguing historical signals in sleep, pain, and stress-response research.
For readers who evaluate peptides not by hype but by genuine scientific depth, DSIP is compelling precisely because of its ambiguity: there seems to be a signal, but final clarity remains elusive. If your interest extends beyond the usual "headline molecules" to peptides with real scientific intrigue, DSIP very much belongs in that category.
DSIP (Delta Sleep-Inducing Peptide): A Scientific Review
Based on peer-reviewed literature and regulatory documents — see References. Last updated: April 2026.
The Short Version
Delta Sleep-Inducing Peptide (DSIP) is one of the oldest and strangest research peptides in the field. It was first isolated in 1974 from the cerebral venous blood of sleeping rabbits by Swiss researchers Monnier and colleagues — predating the molecular biology era, PCR, and gene sequencing. Fifty years later, it remains scientifically puzzling in ways that few other neuropeptides can match: no confirmed receptor has been identified, no precursor protein or gene has been found, and its mechanisms remain only partially characterised.
Yet DSIP is not a trivially marginal compound. It has been studied in humans, it has published clinical data (however old and limited), it has plausible neuropharmacological activities supported by multiple mechanistic lines of evidence, it is present in human tissue and breast milk, and it crosses the blood-brain barrier — a feature that is genuinely pharmacologically significant.
| At a glance | |
|---|---|
| Full name | Delta Sleep-Inducing Peptide |
| Abbreviation | DSIP |
| Sequence | Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu (9 amino acids) |
| Molecular weight | ~850 Da |
| Origin | First isolated from rabbit cerebral venous blood during sleep (1974–1977) |
| Also found in | Human brain, pituitary, limbic system, breast milk, peripheral organs, plasma |
| Known receptor | ❌ None confirmed |
| Precursor gene | ❌ Not identified |
| Half-life (in vitro) | ~15 minutes (carrier protein complex suspected in vivo) |
| Blood-brain barrier crossing | Yes — unusual among peptides |
| FDA status | ⚠️ Category 2 — cannot be legally compounded; immunogenicity concern cited |
| WADA status | Not specifically listed (as of April 2026); check current list |
| Human evidence | Small IV infusion studies (1980s); ~100-patient withdrawal series (1984); no modern RCTs |
Discovery: A Pre-Molecular-Biology Mystery
In 1974, Marcel Monnier and colleagues at the University of Basel collected blood from the cerebral veins of rabbits in which sleep had been induced by electrical stimulation of the thalamus, then infused this blood into the third ventricle of awake recipient rabbits. The recipients showed characteristic EEG changes — increased delta-wave (slow-wave) activity consistent with deep sleep. Through systematic fractionation of the blood, the active sleep-inducing component was isolated and sequenced: a nonapeptide with the sequence Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu (WAGGDASGE).[1][2]
What makes DSIP scientifically anomalous
Fifty years of subsequent research has produced a picture unlike almost any other peptide in neuroscience. The gene responsible for producing DSIP has not been found in any organism studied. No G-protein-coupled receptor, ion channel, or other binding site has been confirmed as the primary DSIP receptor.[8] This is genuinely unusual: for virtually every other neuropeptide characterised since the 1970s, the molecular biology era identified the gene encoding the precursor peptide and at least a candidate receptor. For DSIP, neither has been established. Database searches have also found that the DSIP sequence aligns with a protein from the bacterium Amycolatopsis coloradensis — suggesting a possible bacterial origin, or a remarkable case of convergent molecular evolution. This is not a reason to dismiss DSIP — but mechanistic understanding is built on indirect evidence rather than the usual molecular framework.
Chemistry and Structural Properties
DSIP is a linear nonapeptide with no disulphide bridges or unusual modifications: H&sub2;N-Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu-COOH.
| Property | Detail |
|---|---|
| Length | 9 amino acids |
| Molecular weight | ~850 Da |
| Character | Amphiphilic (both hydrophilic and hydrophobic regions) |
| Blood-brain barrier permeability | Yes — can cross BBB in both directions |
| Oral stability | Reported to resist gut enzymatic degradation — unusual for a peptide |
| In vitro half-life | ~15 minutes (aminopeptidase cleavage) |
| In vivo persistence | Likely longer — carrier protein complexation hypothesised |
Two features are pharmacologically notable. DSIP is amphiphilic, which may facilitate membrane crossing and explain its blood-brain barrier permeability. When compared with most other peptides, DSIP is unusual in that it can freely cross the blood-brain barrier and is reportedly absorbed from the gut without being denatured by enzymes — rare properties that would be significant for therapeutic development. The very short in vitro half-life of ~15 minutes raises a question about how DSIP exerts sustained physiological effects. The most likely answer is that in the body, DSIP complexes with carrier proteins (possibly albumin) that protect it from rapid degradation — a hypothesis that fits available pharmacokinetic evidence but has not been directly confirmed.[9]
Distribution in the Human Body
DSIP has been found in both free and bound forms in the hypothalamus, limbic system, and pituitary, as well as various peripheral organs, tissues, and body fluids. In the pituitary it co-localises with many peptide and non-peptide mediators such as ACTH, MSH, TSH, and melanin concentrating hormone. It is abundant in the gut secretory cells and in the pancreas where it co-localises with glucagon.[8]
DSIP is also present in human breast milk at concentrations of 10–30 ng/mL.[3] Brain and plasma DSIP concentrations exhibit a marked diurnal variation, with levels low in the mornings and higher in the afternoons — consistent with a biological role in sleep preparation, though whether this is causal or correlational is unclear.
Proposed Mechanisms of Action
Without a confirmed receptor, DSIP’s mechanism of action is necessarily described in terms of observed effects on neurotransmitter systems and physiological outputs. Several partially overlapping mechanisms have been proposed.
1. NMDA receptor modulation
DSIP has been reported to block NMDA receptor activity in some systems — a mechanism that would support both its sedative/sleep-promoting effects and proposed neuroprotective properties, since excessive NMDA activation causes excitotoxicity in stroke and neurodegeneration.[10]
2. Opioid system interaction
DSIP does not appear to bind directly to opioid receptors but stimulates the release of endogenous opioid peptides (particularly Met-enkephalin), producing indirect opioid effects. The sleep-inducing effect in the thalamus is suppressed by naloxone (an opioid receptor antagonist) — suggesting that at least part of DSIP’s sleep-promoting mechanism runs through the opioid system. This mechanism may underlie its analgesic properties and its reported utility in withdrawal syndromes.[8]
3. GABAergic potentiation
DSIP has been reported to potentiate the effects of GABA, the brain’s primary inhibitory neurotransmitter. GABA-A receptor activation is the mechanism through which benzodiazepines and barbiturates produce their sedative effects. If DSIP enhances GABAergic tone, this provides a plausible second mechanism for its sleep-promoting effects and also for its reported antiepileptic properties.
4. MAPK / glucocorticoid signalling
DSIP is proposed to interact with components of the MAPK cascade and shows homology to glucocorticoid-induced leucine zipper (GILZ), which can prevent Raf-1 activation and inhibit phosphorylation of ERK. This links DSIP to glucocorticoid biology — consistent with observations that low DSIP levels have been found in Cushing’s syndrome.
5. Adrenergic transmission modulation
Several early reviews propose that DSIP’s physiological actions are primarily mediated through modulation of adrenergic transmission, particularly alpha-1 adrenoceptors. Adrenergic modulation would connect DSIP to both cardiovascular effects (antihypertensive observations in animal studies) and sleep/arousal, since adrenergic tone is a key driver of wakefulness.
| Proposed mechanism | Evidence quality | Established? |
|---|---|---|
| NMDA receptor antagonism | In vitro and animal models | ❌ Not confirmed in humans |
| Indirect opioid agonism (Met-enkephalin release) | Animal models; naloxone blocking consistent | Plausible; not directly confirmed |
| GABAergic potentiation | Animal models | Plausible; not directly confirmed |
| MAPK / glucocorticoid signalling | In silico and in vitro | Speculative |
| Adrenergic transmission modulation | Animal models | Plausible; not directly confirmed |
| Primary receptor target | — | ❌ No receptor identified |
Human Clinical Evidence
Evidence for sleep effects
Schoenenberger et al. 1981 (positive): A double-blind, crossover study in six normal volunteers. DSIP was applied as a slow intravenous infusion at 25 nmol/kg in the morning. Subjects immediately reported a feeling of sleep pressure, and sleep increased by 59% (median total sleep time) within a 130-minute interval after treatment compared with placebo. Delayed effects on subsequent night sleep included shorter sleep onset, reduced stage 1, and better sleep efficiency.[4] Two additional 1984 studies in insomnia patients (approximately 10 patients each) found statistically significant improvements in sleep efficiency, fewer arousals, and increased slow-wave sleep.[5]
Contradictory evidence: Several subsequent studies failed to replicate sleep-promoting effects. One study found that DSIP when administered as an adjunct to isoflurane anaesthesia actually increased heart rate and reduced anaesthetic depth — the opposite of what was expected. In rats, intracerebroventricular DSIP did not increase sleep (attributed to rapid metabolism), though more stable analogues did — with one also producing arousal.[8]
Evidence for withdrawal syndrome treatment
A 1984 series of approximately 100 inpatients with opioid and alcohol withdrawal received intravenous DSIP. In 97% of opiate-dependent and 87% of alcohol-dependent patients, clinical symptoms and signs were reported to disappear after injection of DSIP, although some patients reported occasional headaches.[7]
Evidence for chronic pain
DSIP lowered pain levels significantly in 6 out of 7 patients with migraine, chronic tinnitus, and psychogenic pain attacks after intravenous administration over 5 consecutive days. A simultaneous significant reduction of concomitantly occurring depressive states was also observed.[6] The concurrent improvement in depression raises the question of whether pain relief was mediated through mood improvement rather than direct analgesic action.
Human evidence summary
| Indication | Design | N | Finding | Confidence |
|---|---|---|---|---|
| Acute sleep promotion [4] | DB crossover RCT | 6 | 59% ↑ sleep time; improved efficiency | Very low (tiny N) |
| Insomnia [5] | Small clinical studies | ~10 | ↑ sleep efficiency; fewer arousals | Very low |
| Opioid withdrawal [7] | Uncontrolled inpatient series | ~100 | 97% success | ❌ Very low (no control) |
| Alcohol withdrawal [7] | Uncontrolled inpatient series | ~100 | 87% success | ❌ Very low (no control) |
| Chronic pain [6] | Uncontrolled pilot | 7 | Significant pain reduction in 6/7 | Very low |
| As anaesthetic adjunct | Controlled observation | Small | Increased HR; reduced anaesthetic depth | Contradicts expected effect |
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) | ⚠️ Category 2 bulk drug substance — cannot be legally compounded; immunogenicity concerns cited [12] |
| EMA (Europe) | ❌ Not approved |
| WADA | Not specifically listed as of April 2026 — verify current list |
| Research chemical market | Available from multiple vendors; unregulated |
The FDA notes that compounded drugs containing DSIP may pose a risk for immunogenicity, and that no safety-related information regarding DSIP has been identified, so it is unknown whether it could be harmful to humans.[12] Since DSIP’s precursor gene has not been found, the immune system may treat injected DSIP as a foreign peptide — a mechanism of risk that is real even if unquantified. The Category 2 designation does not mean DSIP is known to be dangerous; it means there is insufficient information to conclude it is safe.
Safety: What Is Known and Unknown
Short-term human safety (published data)
The early human studies reported minimal adverse effects. Transient headache, dizziness, nausea, and vertigo are the most commonly described side effects following IV infusion. No serious adverse events or deaths have been reported in any published study. A 2001 editorial described DSIP as “incredibly safe” based on the absence of any lethal dose in animal studies — a description that reflects the limited information available rather than a rigorous safety characterisation.[9]
Unknown and uncharacterised risks
| Safety concern | Status |
|---|---|
| Long-term effects of repeated subcutaneous dosing | ❌ Not studied |
| Immunogenicity with chronic use | ⚠️ Explicitly flagged by FDA; not formally assessed |
| Drug interactions | ❌ Not characterised |
| Effects in pregnant or breastfeeding individuals | ❌ Not studied (DSIP is present in breast milk, but exogenous dosing is unstudied) |
| Cancer-related risk | ❌ Not assessed; MAPK/ERK pathway interaction could theoretically be relevant |
| Safety in renal or hepatic impairment | ❌ Not studied |
DSIP vs. Other Sleep-Related Compounds
| Compound | Mechanism | Human evidence | Regulatory status |
|---|---|---|---|
| DSIP | Unknown; NMDA modulation, indirect opioid, GABA potentiation | Small 1980s IV studies; contradictory | ❌ Not approved; FDA Category 2 |
| Melatonin | MT1/MT2 receptor agonist; circadian regulation | Extensive | ✅ OTC (US); approved EU (specific indications) |
| Ramelteon (Rozerem) | MT1/MT2 agonist | Phase 3 trials | ✅ FDA-approved |
| Suvorexant (Belsomra) | Orexin receptor antagonist | Phase 3 trials | ✅ FDA-approved |
| Benzodiazepines | GABA-A positive allosteric modulator | Extensive | ✅ FDA-approved; controlled substances |
| Z-drugs (zolpidem) | GABA-A positive allosteric modulator | Extensive | ✅ FDA-approved; controlled substances |
What Is Confirmed and What Remains Unknown
| ✅ Confirmed (with caveats) | ❌ Not established |
|---|---|
| DSIP is present endogenously in human brain, pituitary, and plasma | Its receptor |
| Plasma levels correlate with circadian rhythm and sleep initiation | Its precursor gene |
| It crosses the blood-brain barrier — rare for a peptide | Its precise mechanism of action |
| IV infusion increased sleep time in 6 healthy volunteers (1981) [4] | Whether subcutaneous dosing produces similar effects to IV |
| Reported effects on withdrawal symptoms in ~100 inpatients [7] | Whether withdrawal effects are real (no control group) |
| No lethal dose established in animals | Long-term safety with repeated use |
| Short-term IV use produced minor adverse effects only | Immunogenicity risk with chronic dosing |
Common Misconceptions
“It’s been studied for 50 years, so we know how it works.”
Fifty years of study have not identified its receptor, precursor gene, or primary mechanism of action. Extensive study has produced extensive contradictions. Longevity of research does not substitute for mechanistic clarity.
“It’s naturally found in the body, so it must be safe.”
DSIP is present endogenously, but endogenous presence does not validate exogenous injection at potentially supraphysiological concentrations. The FDA’s immunogenicity concern is specifically about injecting what may be treated as a foreign peptide — not about DSIP’s presence in normal physiology.[12]
“The 97% withdrawal success rate means it treats addiction.”
The 97% figure comes from a single uncontrolled inpatient study published in 1984. Without a placebo group, it is impossible to separate DSIP’s effect from the benefits of hospitalisation, supportive care, clinical attention, and natural withdrawal progression. The finding is interesting and warrants proper investigation — but it cannot be cited as evidence that DSIP treats addiction.[7]
“Unlike sedatives, DSIP doesn’t cause sedation — it’s a natural sleep promoter.”
The 1981 human study found increased sleep time without classic pharmacological sedation. But the anaesthesia study found increased heart rate and reduced anaesthetic depth — suggesting that DSIP’s effects on the CNS are complex, dose-dependent, and not fully predictable. “Not sedating” does not mean “without CNS effects.”
Frequently Asked Questions
Is DSIP the same as melatonin?
No. They operate through completely different mechanisms. Melatonin regulates circadian timing by activating MT1/MT2 receptors in the suprachiasmatic nucleus. DSIP is proposed to modulate sleep architecture — particularly slow-wave sleep depth — through NMDA, opioid, and GABAergic pathways. They address different aspects of sleep biology.
Can it be legally compounded in the US?
No. DSIP is on the FDA’s Category 2 list — it cannot be legally compounded under the 503A framework, reflecting both immunogenicity concerns and the absence of adequate safety information.[12]
Why hasn’t a receptor been found after 50 years?
This is genuinely unanswered. The most likely explanations are that DSIP acts through multiple receptors rather than one primary target; the receptor is an atypical binding site that standard screening methods do not easily identify; or DSIP’s primary mode of action is through modulation of other peptide systems (indirect opioid, GABAergic) rather than direct receptor binding. The absence of a known gene and precursor also suggests that the biological origin of endogenous DSIP is still not understood.[8]
Is DSIP on the WADA prohibited list?
DSIP is not explicitly listed as a prohibited substance on the WADA list as of April 2026, but athletes should check the current year’s list directly, as the list is updated annually and the S2 category (peptide hormones and growth factors) could potentially encompass it.
Key Takeaways
- DSIP is one of the most biologically interesting and least understood peptides in neuroscience. After 50 years of research, it has no confirmed receptor, no known precursor gene, and no consensus mechanism — yet produces real, measurable physiological effects in animals and (inconsistently) in humans.[8]
- Human evidence is limited, dated, and partially contradictory. The best sleep data comes from a 6-person IV infusion study from 1981. The most striking clinical claim (97% withdrawal success) has no control group. No modern, adequately powered RCT exists for any indication.
- ⚠️ The FDA’s immunogenicity concern is scientifically credible. Without a confirmed endogenous gene or precursor, injecting DSIP may present it to the immune system as a foreign peptide — a mechanism of risk that is real even if unquantified.[12]
- DSIP occupies a genuinely distinct mechanistic niche. No approved sleep medication works through NMDA modulation combined with indirect opioid enhancement. If its mechanism is eventually clarified, DSIP or a stable analogue might offer something genuinely different from existing pharmacology.
- The compound’s unusual pharmacokinetic properties — BBB permeability, apparent oral absorption — are genuinely notable and distinguish it from most research peptides. Whether these properties translate to practical therapeutic advantage is not yet established.
- ⚠️ Research-grade DSIP from unregulated vendors carries quality and purity risks entirely separate from the scientific question of whether DSIP has biological effects. The Category 2 designation and the FDA’s safety concerns apply regardless of vendor claims.
References
Discovery and Foundational Studies
- Monnier M, Hösli L. Dialysis of sleep and waking factors in blood of the rabbit. Science. 1964;146:796–798.
- Schoenenberger GA, Maier PF, Tobler HJ, et al. A naturally occurring delta-EEG-enhancing nonapeptide in urine of sleep-deprived rats. Pflügers Archiv. 1977;369(2):99–109.
- Graf MV, Hunter CA, Kastin AJ. Presence of delta sleep-inducing peptide-like material in human milk. Journal of Clinical Endocrinology & Metabolism. 1984;59(1):127–132.
Human Sleep Studies
- Schoenenberger GA, et al. Acute and delayed effects of DSIP (delta sleep-inducing peptide) on human sleep behavior. International Journal of Clinical Pharmacology, Therapy, and Toxicology. 1981. PMID: 6895513
- Schneider-Helmert D, et al. Effects of DSIP on chronic insomnia patients. Neuropsychobiology. 1984 series.
Withdrawal and Clinical Applications
- Larbig W, Gerber WD, Kluck M, Schoenenberger GA. Therapeutic effects of DSIP in patients with chronic, pronounced pain episodes: a clinical pilot study. European Neurology. 1984;23:372–385. PMID: 6548970
- Wikipedia. Delta-sleep-inducing peptide — section on addiction and withdrawal. en.wikipedia.org/wiki/Delta-sleep-inducing_peptide
Reviews
- Graf MV, Kastin AJ. Delta-sleep-inducing peptide (DSIP): a review. Neuroscience & Biobehavioral Reviews. 1984;8(1):83–93. PMID: 6145137
- Pollard BJ, Pomfrett CJD. Delta sleep-inducing peptide. European Journal of Anaesthesiology. 2001;18(7):419–422.
- ScienceDirect Topics. Delta Sleep-Inducing Peptide. sciencedirect.com
Animal Studies (Selected)
- Delta Sleep-Inducing Peptide recovers motor function in SD rats after focal stroke. Molecules. 2021;26(17):5173. MDPI
Regulatory Sources
- FDA. Certain Bulk Drug Substances for Use in Compounding that May Present Significant Safety Risks — Category 2 (includes DSIP). fda.gov
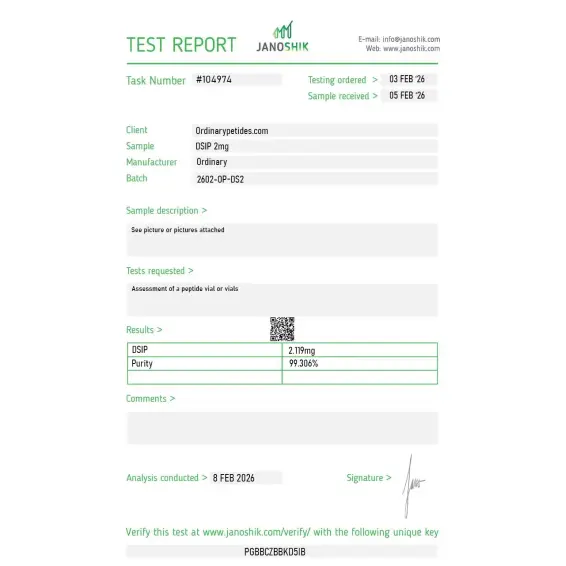
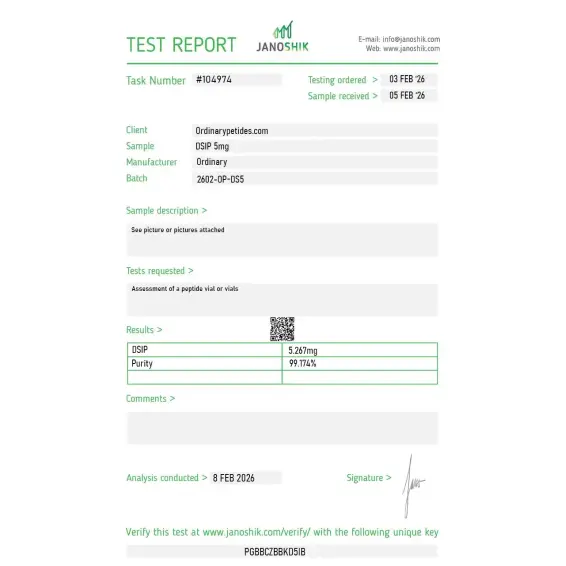
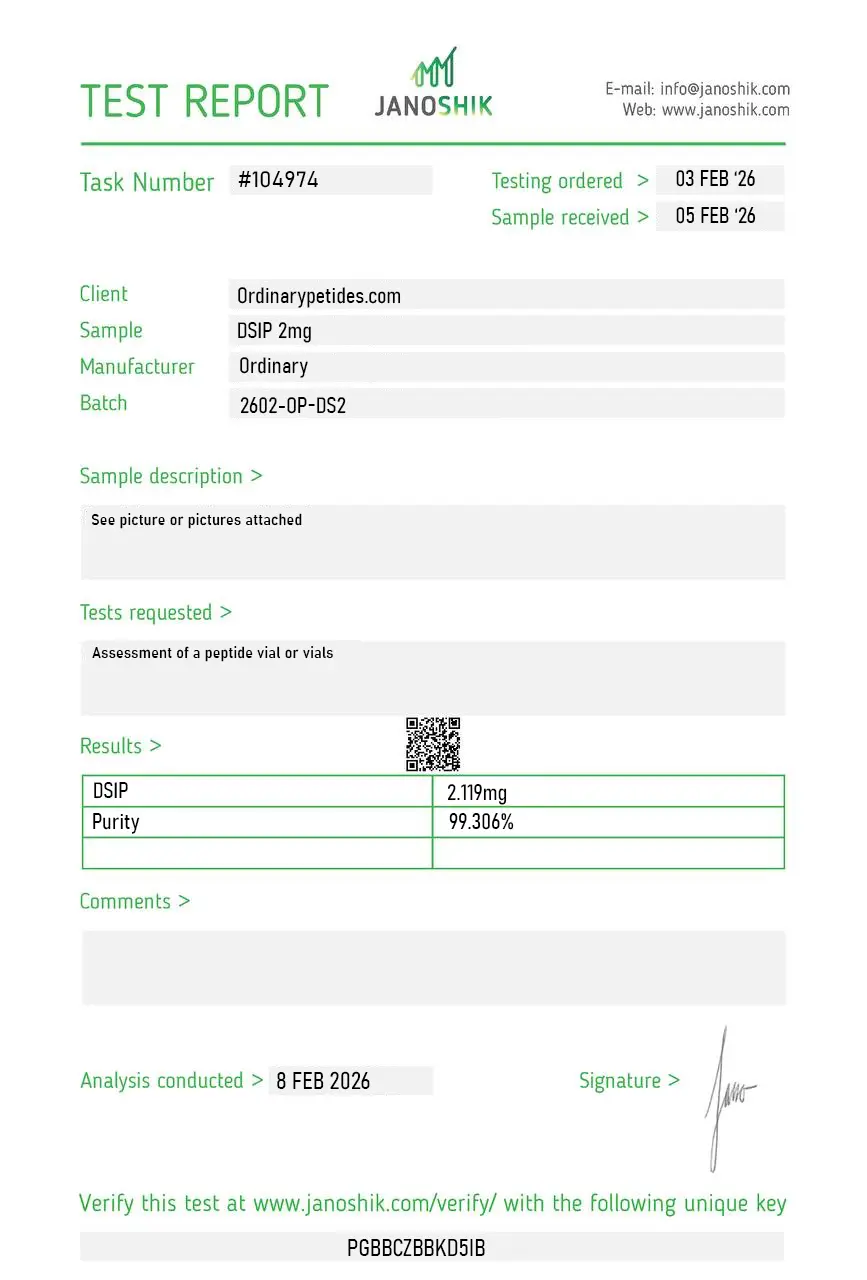
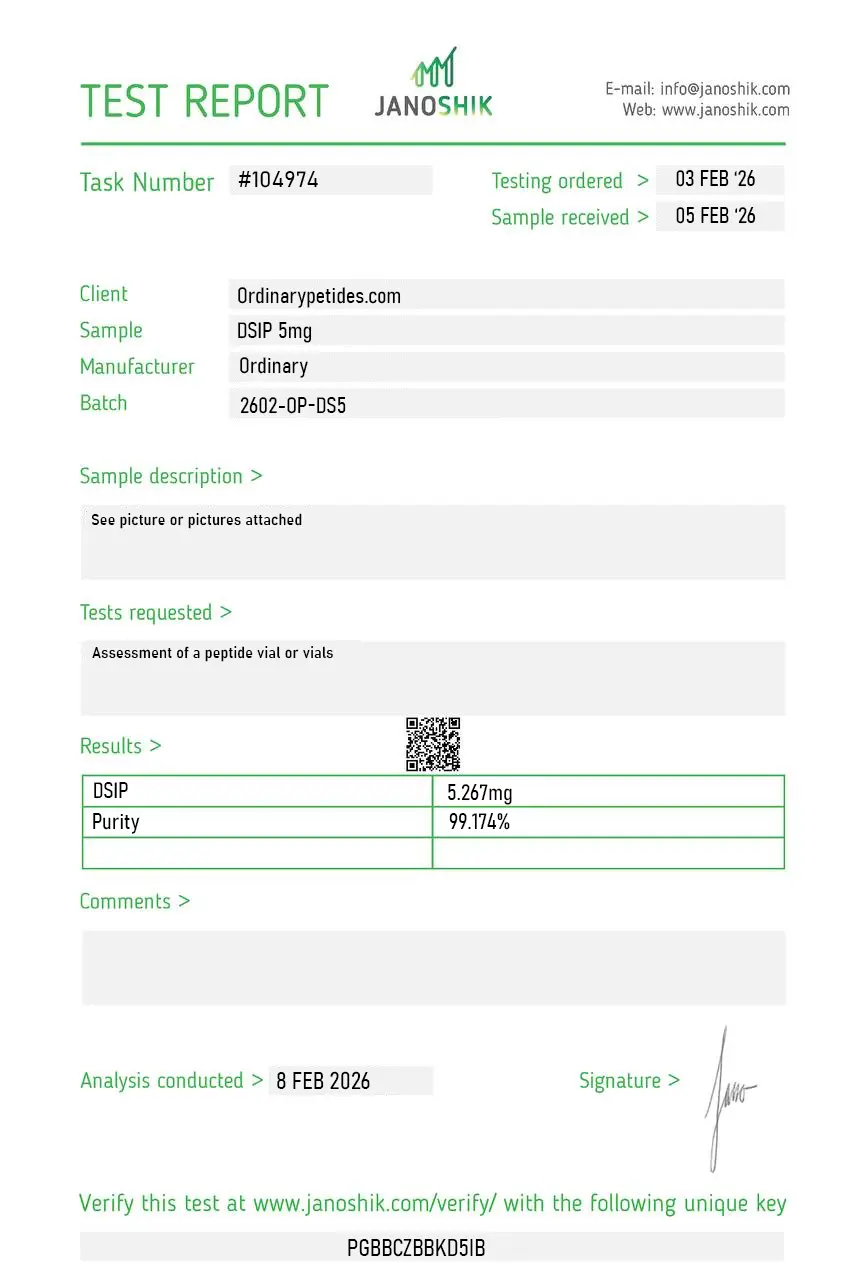
Certificate of Analysis
Independent test reports are available for DSIP 2mg and 5mg batches. These reports provide batch-level documentation and analytical verification information for research reference.
The honest appeal of DSIP for us is that it's a well-defined molecule attached to a famously underdetermined biology — perfect for methods development, where you want a real compound that won't surprise you chemically while you debug the assay around it. Reconstituted clean, ran reproducibly, sequence checked out by MS. A reliable known quantity standing in for an unknown one, which is exactly the contradiction we needed.
What I respect is that the listing carries the 1977 isolation name without building a sleep-marketing pitch on top of it. The original delta-EEG observation never resolved into a mechanism, and a compound page that states the historical name plainly while leaving the unproven claim alone is being honest about a genuinely unresolved piece of neuropeptide history. We study its stress-axis signaling, not sleep, and the framing didn't get in our way.
The instability is the thing that needs documenting and didn't get documented. DSIP is reported to undergo spontaneous deamidation and possible cyclization in solution — the Asn and the Asp-Gly motifs are vulnerable — and a vendor selling it without a word on reconstituted-form storage is leaving the buyer to rediscover that the hard way. We handled it conservatively. The lyophilized material itself was fine; the missing handling guidance for such a known-labile peptide is the gap.
Our interest is the blood-brain-barrier transport question — DSIP was originally isolated from cerebral venous blood, which raises the still-unresolved problem of how a nonapeptide crosses into or out of the CNS at all. We use it as a model substrate in BBB transport-model work, entirely apart from the sleep story it's named for. The material behaved consistently in our transcytosis assays, which is what the model needs.
DSIP (Delta Sleep-Inducing Peptide), also known as emideltide, is a naturally occurring nonapeptide — nine amino acids — with the sequence Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu. It was first isolated in 1977 from the cerebral venous blood of rabbits during slow-wave sleep induction experiments by Swiss researchers Monnier and Schoenenberger. It has since been found in small quantities in human brain tissue, plasma, and at notably higher concentrations in breast milk — leading some researchers to hypothesize a role in post-feeding sleep in newborns. One of its most unusual properties for a peptide is that it can cross the blood-brain barrier and shows oral bioavailability, making it pharmacologically distinct from most neuropeptides.
In research contexts, DSIP has been explored for its potential influence on stress adaptation, recovery, and hormonal axis regulation, which may be of interest in male-focused endocrine studies. However, it is not classified as a testosterone replacement or performance-enhancing compound.
Research findings on DSIP are mixed, with some experimental models suggesting effects on sleep regulation and stress response. Outcomes depend heavily on study design, dosing protocols, and research conditions.
There is limited evidence suggesting DSIP directly increases testosterone. Some studies have explored hypothalamic-pituitary interactions, but it is not established as a primary testosterone-enhancing peptide.
In research settings, DSIP is typically administered prior to sleep-cycle evaluation periods or during stress-response protocols, depending on study objectives.
Reported onset timing varies in experimental settings, with some observations suggesting effects within a short window after administration. Response timing may depend on dosage and research model conditions.
The "15 minute sleep trick" is a behavioral sleep strategy suggesting that if sleep does not occur within approximately 15 minutes, the individual temporarily leaves the sleep environment before returning. It is not specific to DSIP but relates to general sleep hygiene principles.
Reported observations in research settings may include mild dizziness, fatigue, vivid dreams, or temporary changes in sleep patterns. Effects appear to be dose-dependent and variable across models.
It is a real peptide, historically known as delta sleep-inducing peptide; in official FDA nomenclature, the name emideltide appears as a synonym for DSIP.
The most accurate answer is: older small human studies reported improved sleep in some patients, but there is no modern large confirmatory evidence base.
Yes, but they are mostly small older studies from the 1980s to early 1990s on sleep, pain, and related states.
No approval is visible in the reliable sources. On the contrary, the FDA treats emideltide (DSIP) as a substance associated with potential significant safety risks in the compounding context.
No. The evidence base is insufficient for that.
Because it is a beautiful and biologically intriguing idea: a short peptide potentially linked to sleep, pain, and stress. But that beauty is also what can make it harder to see how scientifically unfinished the story still is.
DSIP's precise mechanism of action remains incompletely understood despite nearly five decades of research — which is itself a defining characteristic of this peptide. It is found in the hypothalamus, limbic system, and pituitary where it co-localizes with ACTH, MSH, TSH, and other regulatory peptides. Its proposed mechanisms include promotion of slow-wave (delta) sleep through interactions with NMDA receptors and GABAergic systems, modulation of melatonin and serotonin signaling to regulate the sleep-wake cycle, reduction of corticotropin-releasing factor (CRF) and cortisol to blunt stress responses, stimulation of LH, GH, and somatoliberin secretion while inhibiting somatostatin, and antioxidant effects through enhanced mitochondrial oxidative phosphorylation. It appears to act as a stress-limiting and homeostatic regulatory factor across multiple endocrine and neurological systems simultaneously.
Human studies exist but results are notably inconsistent — a recurring theme in the DSIP literature. In a 1981 double-blind crossover study in healthy volunteers, intravenous DSIP at 25 nmol/kg in the morning increased total sleep time by 59% within a 130-minute window and improved subsequent night sleep efficiency and onset latency. A 1992 double-blind parallel-group study in 16 chronic insomniac patients showed higher sleep efficiency and shorter sleep latency with DSIP versus placebo, though the effects were described as statistically weak. Clinical pain studies from 1984 reported therapeutic effects in patients with chronic pain. Importantly, human and animal studies have also shown variable results including no effect on sleep or even paradoxical insomnia in some cases, which prevents any firm conclusions about consistent efficacy.
Beyond sleep, research has suggested multiple additional properties. In animal studies it demonstrated anticonvulsant effects in epilepsy models, significant antinociceptive (pain-reducing) properties, antiedematic effects through GABAergic activation, neuroprotective effects in cerebral ischemia models, antioxidant activity through antioxidant system activation, and remarkably — anti-tumor and geroprotective effects in a lifetime mouse study where DSIP decreased spontaneous tumor incidence 2.6-fold and increased maximum lifespan by 24.1%. Abnormal DSIP plasma and CSF levels have been found in patients with major depressive disorder, suggesting a potential role in mood regulation.
Research protocols and clinical studies have primarily used intravenous administration at approximately 25 nmol/kg body weight. In wellness and biohacking contexts it is most commonly given by subcutaneous injection, typically 100 to 500 mcg administered 30 to 60 minutes before bedtime. Some use it on an as-needed basis rather than nightly, and short cycles of 2 to 4 weeks are recommended to avoid potential adaptation. Its oral bioavailability — unusual for a peptide — also makes oral administration a theoretical option that some researchers have explored.
DSIP has a generally favorable safety profile in available research. The most commonly reported effects are daytime drowsiness or grogginess if dosing is too high or mistimed, mild headache or dizziness, occasional nausea, and mild injection site reactions. Potential hormonal fluctuations are a consideration given its effects on LH, GH, and cortisol. The paradoxical wakefulness effect observed in some studies — including one where it actually increased heart rate and reduced anesthesia depth when used as an adjunct to isoflurane — demonstrates that its effects are not uniformly sedating and can be unpredictable. Long-term safety data is absent.
People with severe psychiatric conditions — particularly depression given abnormal DSIP levels found in MDD — should consult a physician before use. Those with untreated severe sleep apnea should not use additional CNS-modulating compounds without medical oversight. Pregnant or breastfeeding women should avoid it despite its natural presence in breast milk, as pharmacological concentrations are different from physiological ones. Given the inconsistency of effects across studies and individuals, people with significant neurological or endocrine disorders should approach with particular caution. As with all research peptides it should only be used under qualified medical supervision.





