The main risk is to confuse a late-stage development programme with an already approved and established standard of care. That is not the case yet.





Cagrilintide
Product Usage: Research Only
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Sequence
Cagrilintide (long-acting amylin analogue)
Molecular Formula
C194H312N54O59S2.xH4O2
Molecular Weight
4409.01 g/mol
Form
Lyophilized powder
Purity
≥ 99% (HPLC)
CAS#
1415456-99-3
Storage
−20°C, dry & dark
Research use only
Not for human or veterinary use.
Cagrilintide: A Serious Amylin-Based Candidate With a Strong Clinical Story
Cagrilintide is not just "another trendy peptide," but a serious amylin-based drug candidate that has already drawn substantial attention in the clinical obesity field. In early studies and later-stage clinical programs, it showed dose-dependent body-weight reduction, and in combination with semaglutide, the clinical results looked even stronger.
Its main appeal lies in its amylin-based logic. In clinical and mechanistic discussion, cagrilintide has been associated with stronger satiety signaling and more controlled regulation of eating behavior, rather than with yet another vague promise to "speed up metabolism." That distinction matters, because it places the molecule in a much more serious pharmacological context.
What makes cagrilintide especially interesting is that behind it stands not forum hype, but a large-scale pharmaceutical development program and a real clinical research track. This is exactly the kind of case where the molecule is supported by more than marketing language. It has a clear therapeutic concept, a modern obesity-medicine rationale, and a development pathway that looks meaningfully stronger than the usual grey-market peptide narrative.
Cagrilintide: A Scientific Review of the Long-Acting Amylin Analogue
Based on peer-reviewed literature — see References. Last updated: April 2026.
⚠️ Disclaimer. This article is for informational and educational purposes only. It is not medical advice, a prescription, a treatment recommendation, or an instruction for use. Cagrilintide is not approved by the FDA or EMA as a standalone drug as of April 2026. A New Drug Application (NDA) for the combination product CagriSema (cagrilintide + semaglutide) was filed by Novo Nordisk in December 2025, with a regulatory decision anticipated in late 2026. Cagrilintide should only be used under the supervision of a qualified medical professional, if at all. Nothing in this article constitutes a recommendation to use this compound outside of an authorised clinical trial or approved indication.
The Short Version
Cagrilintide is a long-acting synthetic analogue of amylin — a pancreatic hormone that most people have never heard of, despite its central role in appetite regulation. Developed by Novo Nordisk and also known as AM833 or NN9838, it belongs to a class called dual amylin and calcitonin receptor agonists (DACRAs) — a mechanistically distinct pathway from the GLP-1 receptor agonists (semaglutide, liraglutide) that currently dominate anti-obesity pharmacology.
Unlike BPC-157 or TB-500, cagrilintide has a genuine, rigorous, and extensive human clinical evidence base. Its pivotal Phase 3 trial (REDEFINE 1) was published in the New England Journal of Medicine in June 2025, with 3,417 participants.[1] As a monotherapy, it produced 11.8% mean body weight reduction at 68 weeks. In combination with semaglutide (as CagriSema), it produced 20.4% — among the most significant weight loss results ever documented for any pharmacological agent. An NDA for CagriSema is currently under FDA review.[12]
This is not a research chemical. It is a pharmaceutical candidate in late-stage regulatory review.
| At a glance | |
|---|---|
| Also known as | AM833, NN9838, NN0174-0833 |
| Drug class | Dual amylin and calcitonin receptor agonist (DACRA) / long-acting amylin analogue |
| Developer | Novo Nordisk (Copenhagen, Denmark) |
| Combination product | CagriSema (cagrilintide 2.4 mg + semaglutide 2.4 mg, once-weekly) |
| Target receptors | AMY1R, AMY3R (amylin receptors), CTR (calcitonin receptor) |
| Administration | Subcutaneous injection, once weekly |
| Plasma half-life | ~7–8 days (enables weekly dosing) |
| Highest clinical phase | Phase 3 (REDEFINE programme, completed; RENEW programme initiating) |
| FDA status | Not approved standalone; CagriSema NDA filed December 2025 |
| NDA decision timeline | Anticipated late 2026 |
The Biological Foundation: Understanding Amylin
Amylin (also known as islet amyloid polypeptide, or IAPP) is a 37-amino acid peptide hormone co-secreted by pancreatic beta-cells alongside insulin in response to food intake. It acts on a distributed network of brain regions — including the area postrema, dorsal vagal complex, lateral parabrachial nucleus, and hypothalamus — to signal satiety, slow gastric emptying, and suppress post-meal glucagon secretion.[9] In obesity, amylin signalling is attenuated — analogous to leptin resistance, where the hunger-suppressing signal is present but not effectively received.
The challenge with using native human amylin therapeutically is severe: it is highly prone to forming amyloid fibrils, which makes it toxic at therapeutic concentrations and impossible to formulate safely. Pramlintide (brand name Symlin) was the first analogue — FDA-approved in 2005 as an adjunct to insulin for type 1 and type 2 diabetes. It works but requires three daily injections due to its short half-life and produces only modest weight loss. The need for a long-acting, more potent, and safer formulation drove the next generation of amylin-based therapeutics, of which cagrilintide is the most clinically advanced.[10]
Development and Structure
Cagrilintide was developed by Novo Nordisk’s research and early development team. The development programme was led by Thomas Kruse and colleagues, with the key publication appearing in the Journal of Medicinal Chemistry in 2021.[4] A hallmark of the pancreatic hormone amylin is its high propensity toward the formation of amyloid fibrils, which makes it a challenging drug design effort. The amylin analogue pramlintide requires three daily injections due to its short half-life. Cagrilintide was engineered to solve these problems simultaneously.
| Modification | Purpose |
|---|---|
| N14E, V17R, P37Y amino acid substitutions | Reduce fibrillation risk; increase potency and receptor affinity |
| N-terminal C20 fatty diacid lipidation | Enables reversible albumin binding → extends half-life to ~7–8 days |
| C-terminal proline substitution (P37) | Further stability enhancement; contributes to helical structure |
| E14-R17 intramolecular salt bridge | Enhances helical stability in the receptor-bound conformation |
The result is a molecule that activates amylin receptors (AMY1R and AMY3R) and the calcitonin receptor (CTR) non-selectively — making it a “DACRA” — with a half-life appropriate for once-weekly subcutaneous dosing and substantially greater potency than pramlintide. A single dose of 3 nmol/kg of cagrilintide will cause a similar reduction to amylin pump infusion for up to 48–60 hours in the rat — a dramatic improvement over pramlintide’s ~6-hour duration of action.[4]
Mechanism of Action
Cagrilintide’s mechanism is distinct from GLP-1 receptor agonists in both the receptors it engages and the brain regions it primarily acts upon.
Receptor targets
Amylin receptors are heterodimers composed of the calcitonin receptor (CTR) paired with one of three receptor activity modifying proteins (RAMP1, RAMP2, or RAMP3): AMY1R = CTR + RAMP1; AMY2R = CTR + RAMP2; AMY3R = CTR + RAMP3. Cagrilintide binds non-selectively to all three amylin receptor subtypes and to CTR directly. Body weight loss was observed in wild-type cagrilintide-treated mice, and the absence of RAMP1 and RAMP3 impeded cagrilintide’s potency — demonstrating its dependency on AMY1R and AMY3R.[6] Cryo-EM structural studies have illuminated precisely how cagrilintide engages its receptors, revealing key molecular features including the F23Cagri residue anchoring the peptide at the receptor transmembrane bundle and an E14-R17 intramolecular salt bridge enhancing helical stability.[5]
Brain circuits involved
Unlike GLP-1 receptor agonists, which act primarily through receptors in the hypothalamus and hindbrain, cagrilintide’s primary sites of action include the area postrema (AP) and dorsal vagal complex (DVC) in the hindbrain, the lateral parabrachial nucleus (LPBN) — which integrates satiety signals with reward/hedonic feeding — and the mediobasal hypothalamus. This distributed neural mechanism means cagrilintide acts on both the homeostatic and hedonic dimensions of food intake — a combination thought to be critical for sustained weight management.
Key downstream effects
| Effect | Mechanism | Clinical significance |
|---|---|---|
| Reduced food intake | Satiety signalling via AP/LPBN circuits | Primary weight loss driver |
| Slowed gastric emptying | Peripheral amylin receptor action | Extends satiety after meals; may reduce post-meal glucose spikes |
| Post-prandial glucagon suppression | Pancreatic/peripheral amylin receptors | Improves glycaemic control |
| Additive/synergistic effect with GLP-1 | Complementary neural circuits | Basis for superior CagriSema outcomes |
Why combining with semaglutide is mechanistically logical
Semaglutide acts through GLP-1 receptors in the hypothalamus, increasing insulin production and reducing glucagon secretion, delaying gastric emptying. These separate, but related mechanisms of action of an amylin analogue and a GLP-1 receptor agonist appear to have an additive effect on appetite reduction.[8] The two compounds target overlapping but distinct receptor systems in complementary brain regions. Preclinical data in non-human primates had previously suggested a synergistic reduction in food intake when combining GLP-1 and amylin agonism. The clinical data have borne this out.
Clinical Trial Programme: The Evidence Base
Cagrilintide has progressed through a rigorous, properly conducted clinical development programme. This is a pharmaceutical candidate with peer-reviewed Phase 3 data — not a research chemical with anecdotal reports.
Phase 1 — Safety and pharmacokinetics
Single and multiple ascending dose studies established the favourable tolerability profile, pharmacokinetic properties (once-weekly dosing feasibility confirmed), and absence of serious safety signals. A Phase 1b combination study confirmed that cagrilintide and semaglutide could be co-administered without pharmacokinetic interaction or unexpected adverse events.
Phase 2 — Dose-finding and combination (2021, Lancet)
A multicentre Phase 2 dose-finding trial enrolled adults with overweight or obesity. Cagrilintide 4.5 mg produced approximately 10% mean weight loss over 26 weeks — significantly superior to liraglutide 3.0 mg (an approved anti-obesity drug) at the same timepoint.[2] A Phase 2 combination trial published in The Lancet in 2023 tested cagrilintide + semaglutide in type 2 diabetes and found significant weight loss and glycaemic improvement with an acceptable safety profile.[3]
Phase 3 — REDEFINE Programme
REDEFINE 1 (pivotal Phase 3a trial) — Published in the New England Journal of Medicine, June 2025.[1] In a phase 3a, 68-week, multicenter, double-blind, placebo-controlled and active-controlled trial, 3,417 adults without diabetes were enrolled. The estimated mean percent change in body weight from baseline to week 68 was −20.4% with cagrilintide–semaglutide as compared with −3.0% with placebo (estimated difference, −17.3 percentage points; 95% CI, −18.1 to −16.6; P<0.001). Study participants receiving cagrilintide monotherapy lost an average of 11.8% compared with 2.3% with placebo. Around one-third (31.6%) of participants receiving cagrilintide monotherapy achieved weight loss of 15% or more compared with approximately 4.7% of those who received placebo.
| Treatment arm | Mean weight loss | ≥15% weight loss | ≥20% weight loss | ≥30% weight loss |
|---|---|---|---|---|
| CagriSema (2.4 mg + 2.4 mg) | −20.4% | ~60%+ | 60% | 23% |
| Cagrilintide 2.4 mg monotherapy | −11.8% | 31.6% | — | — |
| Placebo | −2.3% to −3.0% | 4.7% | — | — |
Additional cardiometabolic findings from REDEFINE 1: significant improvements in systolic blood pressure, waist circumference, lipid profiles, and glycaemic control. Notably, 88% of participants with prediabetes returned to normoglycaemia.
REDEFINE 2 — In patients with type 2 diabetes, CagriSema produced 13.7% mean weight loss — slightly lower than in non-diabetic participants, consistent with the biology of weight loss in T2DM.
REDEFINE 4 — A head-to-head comparison against
15 mg. CagriSema did not meet non-inferiority versus tirzepatide at 84 weeks. This is a clinically important nuance: CagriSema is highly effective, but does not demonstrably outperform the best available approved option head-to-head.
REDEFINE 3 — Ongoing cardiovascular outcomes trial (MACE endpoints). RENEW programme — Dedicated Phase 3 programme for cagrilintide monotherapy, to be initiated following REDEFINE 1 data.
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) | CagriSema NDA filed December 2025; decision expected late 2026 [12] |
| EMA (Europe) | Under regulatory review |
| Cagrilintide standalone | Not approved; RENEW Phase 3 programme planned |
| CagriSema | Not yet approved; under active review |
Safety Profile
Across all clinical trials, cagrilintide has shown a safety profile consistent with other gut hormone-based anti-obesity therapies, with gastrointestinal effects as the primary concern. The most common adverse events were gastrointestinal — nausea, vomiting, diarrhoea, and constipation — all mostly mild to moderate in intensity and improving over time. Approximately 1.0% of participants treated with cagrilintide discontinued the trial due to gastrointestinal events.[1] The slow dose-titration schedule used in trials helps manage the onset of these symptoms.
Bone density / calcitonin receptor concern
One important safety consideration specific to cagrilintide’s pharmacology: it agonises the calcitonin receptor (CTR), which is involved in bone mineral metabolism. There have been suggestions that products containing calcitonin could be associated with malignancy.[11] The REDEFINE programme monitored for this concern, and no meaningful changes in bone mineral density or cancer signal have emerged from Phase 3 data published to date. Longer-term post-marketing surveillance will be informative.
Safety compared to GLP-1 agonists
The severity of gastrointestinal disorders observed for the combination of cagrilintide and semaglutide was comparable to that of GLP-1 in monotherapy[3] — suggesting that the combination does not meaningfully worsen the tolerability profile compared to semaglutide alone.
What Is Confirmed and What Remains Under Investigation
| Confirmed by Phase 3 data | Still under investigation |
|---|---|
| Cagrilintide monotherapy produces ~11.8% weight loss at 68 weeks [1] | Long-term cardiovascular outcomes (REDEFINE 3, ongoing) |
| CagriSema produces ~20.4% weight loss at 68 weeks [1] | Safety signal related to calcitonin receptor / bone / cancer over years |
| Significant cardiometabolic improvements (BP, lipids, HbA1c) [1] | Optimal dosing for specific subpopulations |
| 88% of prediabetes participants normalised glycaemia | Duration of effect after discontinuation |
| GI side effects are the primary concern; mostly mild-moderate [1] | Long-term lean mass preservation |
| CagriSema NDA filed December 2025 [12] | Whether RENEW monotherapy data will support standalone approval |
| Mechanistically distinct from GLP-1 agonists [4] | Head-to-head vs. tirzepatide (REDEFINE 4 did not show non-inferiority) |
How Cagrilintide Compares to Other Anti-Obesity Agents
| Drug | Mechanism | Mean weight loss (Phase 3) | Weekly dosing | FDA status |
|---|---|---|---|---|
| Semaglutide 2.4 mg (Wegovy) | GLP-1 RA | ~15% | Yes | Approved (2021) |
| Tirzepatide 15 mg (Zepbound) | GLP-1 + GIP dual agonist | ~21% | Yes | Approved (2023) |
| Cagrilintide 2.4 mg | DACRA (amylin + calcitonin receptor) | ~11.8% | Yes | Not yet approved |
| CagriSema 2.4+2.4 mg | DACRA + GLP-1 RA | ~20.4% | Yes | NDA filed Dec 2025 |
| Liraglutide 3.0 mg (Saxenda) | GLP-1 RA | ~8% | No (daily) | Approved (2014) |
| Pramlintide | Amylin analogue | ~3–7% | No (3×daily) | Approved (diabetes adjunct) |
The comparison with tirzepatide is instructive. In the REDEFINE 4 non-inferiority study, CagriSema did not meet the non-inferiority bar versus tirzepatide 15 mg. Absolute comparison of percentage weight loss numbers across different trials, patient populations, and endpoints is methodologically unreliable. CagriSema’s clinical value proposition depends on being a mechanistically distinct option for patients who don’t respond to or tolerate GLP-1/GIP-based approaches, and potentially on cardiovascular outcomes data from REDEFINE 3.
The Broader Amylin Revival
Cagrilintide represents the centrepiece of a broader renaissance in amylin-based pharmacology. Several other amylin analogues are in active development: Eloralintide (Eli Lilly), with Phase 2 data published in The Lancet (November 2025) and entering Phase 3 planning; Petrelintide (Zealand Pharma), a selective amylin receptor agonist (SARA) in Phase 2; GUBamy (Gubra / AbbVie), a DACRA in Phase 1 with an AbbVie licensing deal announced March 2025; and AZD6234 (AstraZeneca), an amylin agonist in Phase 1. The therapeutic logic across all of these: amylin agonism addresses parts of the hunger-satiety circuit that GLP-1 agonism alone does not, making it an attractive combination partner and potentially a standalone option for patients seeking a GLP-1-free mechanism.[10]
Common Misconceptions
“Cagrilintide is the same as semaglutide.”
Mechanistically completely different. Semaglutide is a GLP-1 receptor agonist; cagrilintide is an amylin and calcitonin receptor agonist.[4] They work through distinct receptor systems in partially distinct brain regions. Their combination (CagriSema) produces additive weight loss precisely because they are different.
“CagriSema is already FDA-approved.”
Not as of April 2026. An NDA was filed in December 2025; a regulatory decision is anticipated in late 2026.[12] Until that approval is granted, CagriSema is not an authorised drug in the US.
“20% weight loss means it’s better than tirzepatide.”
In a head-to-head comparison (REDEFINE 4), CagriSema did not meet non-inferiority versus tirzepatide 15 mg. Absolute comparison of percentage weight loss numbers across different trials is methodologically unreliable. The two compounds have not been shown to differ significantly in a direct randomised head-to-head study.
“It’s available as a research chemical.”
Cagrilintide does appear on some research chemical vendor websites. This product is entirely distinct from the pharmaceutical-grade compound used in clinical trials — different manufacturing standards, unverified purity, sterility, and peptide content. The impressive NEJM data[1] applies to Novo Nordisk’s precisely characterised pharmaceutical compound, not to unregulated commercial preparations.
Frequently Asked Questions
What is the difference between cagrilintide and pramlintide?
Both are amylin analogues, but they differ in potency, half-life, and receptor pharmacology. Pramlintide requires three daily injections, produces modest weight loss, and is approved only as a diabetes adjunct. Cagrilintide is a once-weekly injection, produces substantially greater weight loss (~11.8% monotherapy vs. ~3–7% for pramlintide), and is being developed for obesity as a primary indication.[4]
When might CagriSema be approved?
Novo Nordisk filed the CagriSema NDA in December 2025.[12] A regulatory decision is anticipated in late 2026, assuming standard FDA review timelines.
Does it affect the heart?
REDEFINE 3 is an ongoing cardiovascular outcomes trial. In REDEFINE 1, improvements in blood pressure, lipids, and glycaemia were observed.[1] Whether these translate into reduced cardiovascular events (MACE) — as semaglutide does in SELECT — is not yet established.
What about lean mass loss?
An emerging concern across all potent anti-obesity medications is loss of lean (muscle) mass along with fat. Cagrilintide-specific lean mass data from REDEFINE trials is not yet fully published, and this remains an active research question. The amylin mechanism does not appear to drive lean mass loss in the way that some GLP-1 agonists do, but this requires systematic evaluation.
Is it being studied for anything other than obesity?
REDEFINE 3 is studying cardiovascular outcomes. Amylin receptors are also present in the kidney and heart, suggesting potential applications in cardiorenal metabolic disease, but these are not yet the subject of dedicated trials for cagrilintide.
Key Takeaways
- Cagrilintide is a well-characterised, properly developed pharmaceutical compound — not a research chemical. It has undergone years of structure-activity optimisation, extensive preclinical work, and a rigorous Phase 3 programme.[4]
- The REDEFINE 1 Phase 3 results are among the most impressive in obesity pharmacology — 20.4% mean weight loss for CagriSema in 3,417 participants, published in NEJM.[1]
- Cagrilintide monotherapy is also clinically meaningful at 11.8% mean weight loss — a level that delivers genuine health benefits even if it trails the combination or tirzepatide.
- The mechanism is genuinely distinct from GLP-1 agonists,[5][6] offering a different biological approach that may serve patients who cannot tolerate or do not adequately respond to GLP-1-based therapy.
- Important questions remain open — cardiovascular outcomes (REDEFINE 3), long-term safety of calcitonin receptor agonism, lean mass impact, and how CagriSema compares to tirzepatide in more balanced head-to-head studies.
- CagriSema is under active FDA review with a decision expected in late 2026.[12] Until that approval is granted, it is not an authorised treatment.
References
Pivotal Clinical Trial
- Kushner RF, et al. Coadministered Cagrilintide and Semaglutide in Adults with Overweight or Obesity (REDEFINE 1). New England Journal of Medicine. Published June 22, 2025. doi: 10.1056/NEJMoa2502081
Key Phase 2 Trials
- Lau DCW, Erichsen L, Francisco AM, et al. Once-weekly cagrilintide for weight management in people with overweight and obesity: a multicentre, randomised, double-blind, placebo-controlled and active-controlled, dose-finding phase 2 trial. Lancet. 2021;398:2160–2172.
- Frias JP, Deenadayalan S, Erichsen L, et al. Efficacy and safety of co-administered once-weekly cagrilintide 2.4 mg with once-weekly semaglutide 2.4 mg in type 2 diabetes. Lancet. 2023;402(10403):720–730.
Mechanistic and Structural Studies
- Kruse T, Hansen JL, Dahl K, et al. Development of Cagrilintide, a Long-Acting Amylin Analogue. Journal of Medicinal Chemistry. 2021;64:11183–11194. doi: 10.1021/acs.jmedchem.1c00565
- Cao J, Belousoff MJ, Johnson RM, et al. Structural and dynamic features of cagrilintide binding to calcitonin and amylin receptors. Nature Communications. 2025;16:3389. doi: 10.1038/s41467-025-58680-y. PMID: 40204768
- Cagrilintide lowers bodyweight through brain amylin receptors 1 and 3. eBioMedicine (Lancet). 2025. PMID: 40609154
- Structural and mechanistic insights into dual activation of cagrilintide in amylin and calcitonin receptors. Acta Pharmacologica Sinica. 2025.
Reviews
- D’Ascanio AM, Mullally JA, Frishman WH. Cagrilintide: A Long-Acting Amylin Analog for the Treatment of Obesity. Cardiology in Review. 2024;32(1):83–90. PMID: 36883831
- Amylin as a Future Obesity Treatment. PMC8735818
- Amylin: From Mode of Action to Future Clinical Potential in Diabetes and Obesity. 2025. PMC12085449
- Mono and dual agonists of the amylin, calcitonin, and CGRP receptors and their potential in metabolic diseases. PMC8085567
Regulatory and Institutional Sources
- Novo Nordisk. CagriSema NDA filing announcement. December 2025.
- Novo Nordisk. REDEFINE 1 Phase 3 data presentations at EASD 2025 (Vienna, September 2025).
- ClinicalTrials.gov. REDEFINE 1 — NCT05567796
Key Investigators
- Timothy Garvey, MD — Professor of Medicine, Director of the Diabetes Research Center, University of Alabama at Birmingham. Lead investigator, REDEFINE 1.
- Thomas Kruse, PhD — Research & Early Development, Novo Nordisk. Principal developer of cagrilintide chemistry.
- Kirsten Raun, PhD — Research & Early Development, Novo Nordisk. Key contributor to pharmacology characterisation.
Batch Documentation
Certificate of Analysis
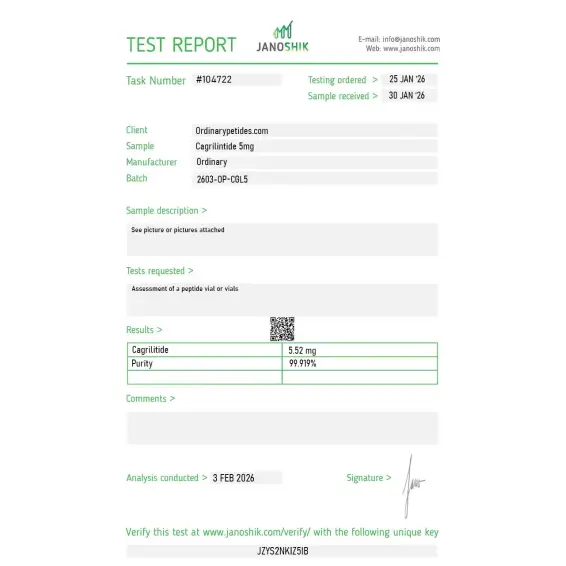
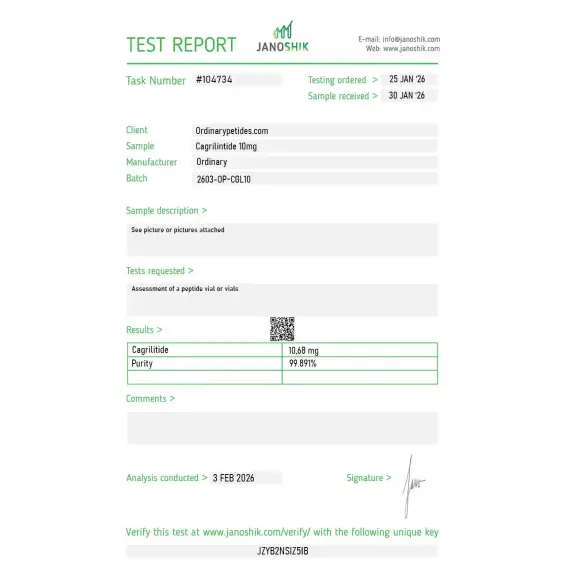
Independent test reports are available for Cagrilintide 5mg and 10mg batches. These reports provide batch-level documentation and analytical verification information for research reference.
Product: Cagrilintide
Available Reports: 5mg • 10mg
Documentation: Batch-specific COA
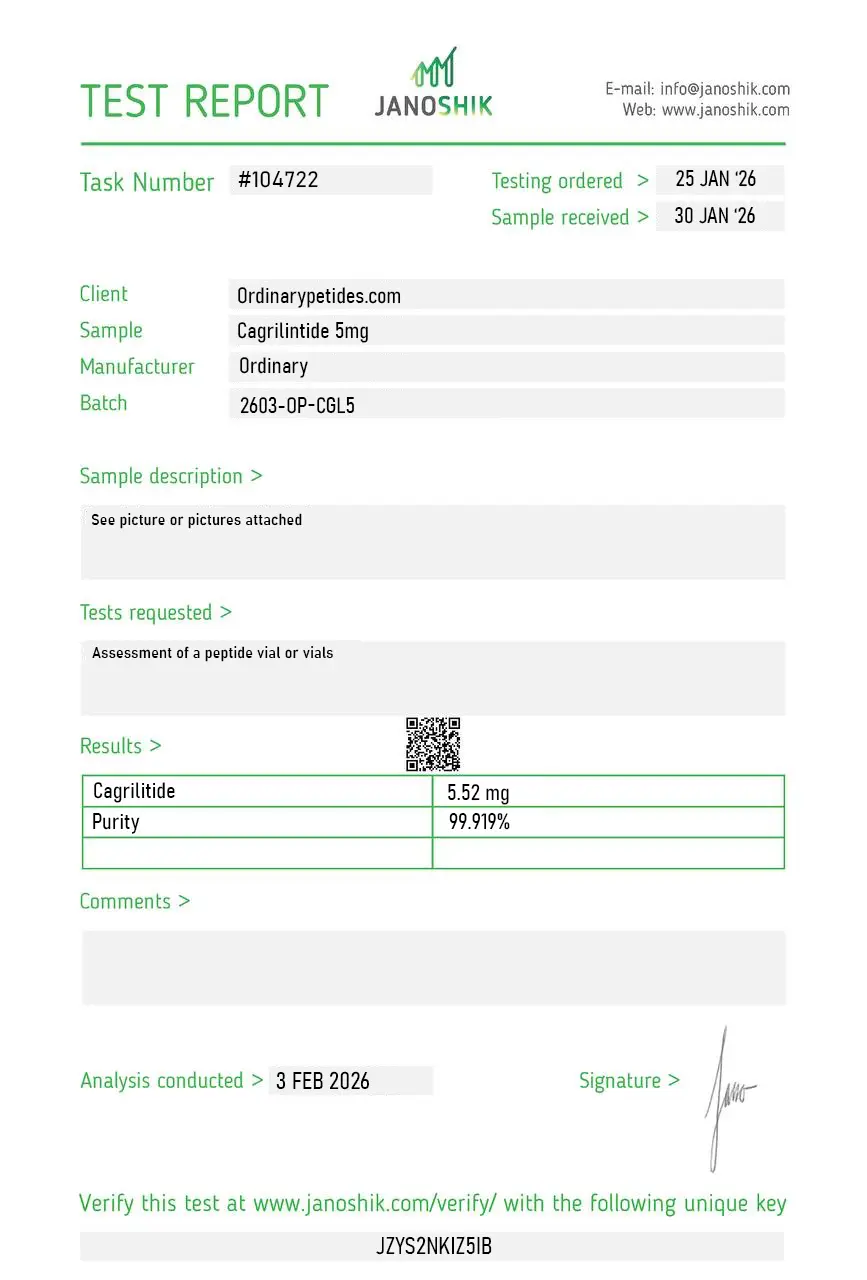
Cagrilintide 5mg
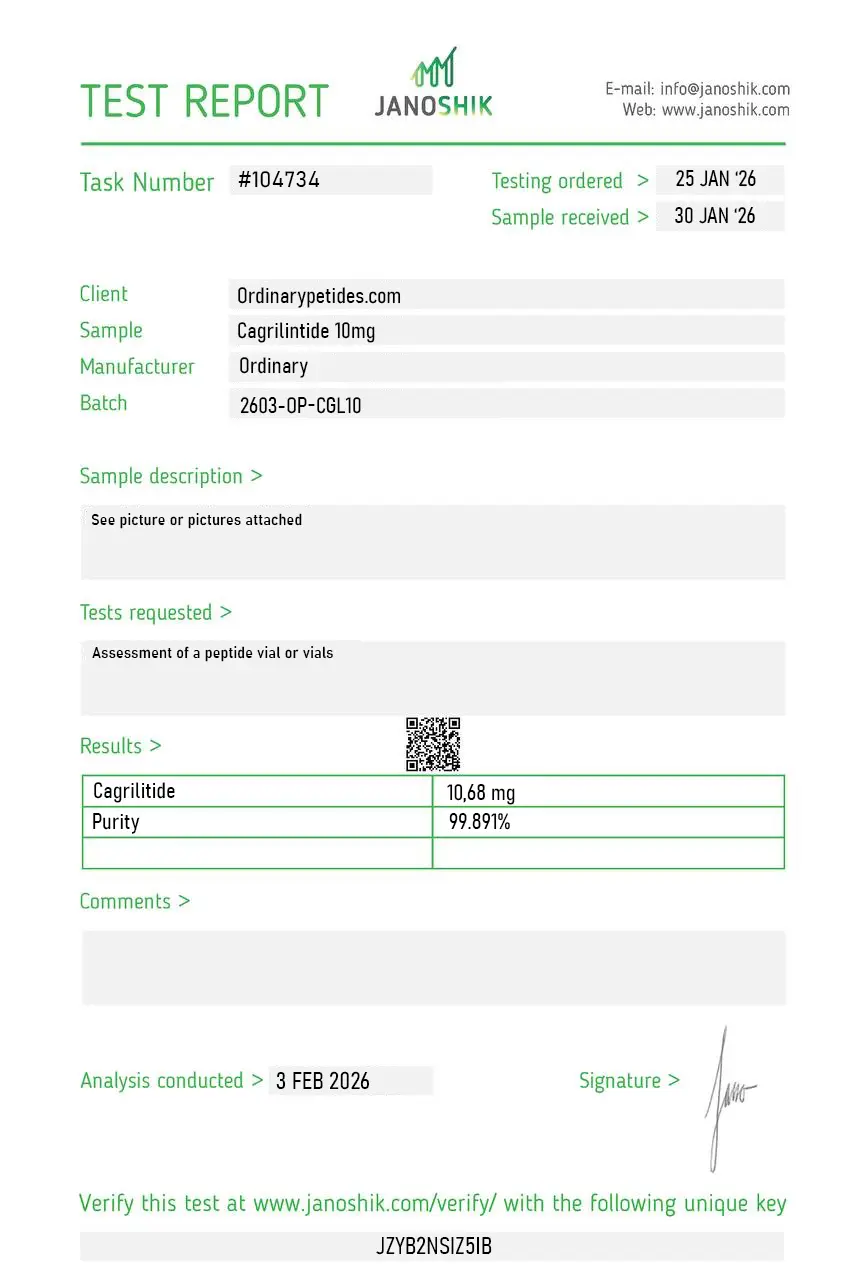
Cagrilintide 10mg
Click any report preview to open the full Certificate of Analysis.
Warren Woods
- April 18, 2026
We run it paired with semaglutide deliberately — the CagriSema combination is the whole reason cagrilintide is interesting clinically, amylin plus incretin hitting appetite through two separate receptor systems. Studying the two co-administered, at controlled ratios from one source, is the only clean way to ask what the amylin component adds over the incretin alone. Both held their profiles across our conditions.
R. Wallace
- March 8, 2026
The acylation is what converts native amylin's hours-long half-life into something weekly, and that lipidation is exactly the part I'd want characterized — the fatty-acid attachment site and the linker, not just overall purity. The COA gave purity but didn't break out the acylation chemistry. Compound performed in our receptor work; I'd just rather verify the modification than trust it on a lipidated analog where the whole pharmacokinetic profile hangs on that one feature.
Paul Sullivan
- January 2, 2026
What pulled us to source it here is the amylin-receptor angle specifically — most of the catalog's metabolic compounds are incretins, and cagrilintide is the rare amylin analog, signaling through the calcitonin-receptor-plus-RAMP complexes rather than GLP-1R. For anyone studying the amylin arm of appetite regulation rather than the incretin arm, it fills a genuine gap. The material activated our AMY-receptor readouts cleanly.
It targets amylin receptors instead of GLP-1 receptors, offering complementary appetite regulation pathways.
Yes, it is commonly studied alongside GLP-1 receptor agonists due to synergistic metabolic effects.
After reconstitution, store refrigerated at 2–8°C and use within 30 days.
Nausea and mild gastrointestinal discomfort are the most frequently observed effects in research settings.
It is supplied strictly for research purposes and not for unsupervised human use.
Yes. It is a peptide analogue of amylin developed for once-weekly subcutaneous administration.
No. As of March 2026, the FDA explicitly states that cagrilintide has not been recognized as safe and effective for any indication.
Yes. There is phase 2 monotherapy, officially disclosed phase 3 monotherapy results, and published phase 3 papers for the combination of cagrilintide + semaglutide.
Because the CagriSema combination produces greater weight reduction than each component alone or placebo.
Based on phase 2 and the official REDEFINE 1 summary, it appears meaningfully effective. But the most powerful publicly published data right now are still for the combination rather than pure monotherapy.
Cagrilintide is a long-acting synthetic amylin analog developed by Novo Nordisk — the same company behind semaglutide (Ozempic, Wegovy). It is engineered to mimic amylin, a naturally occurring peptide hormone co-secreted alongside insulin by pancreatic beta cells after meals. Natural amylin plays a key role in satiety signaling, gastric emptying regulation, and post-meal glucose control, but has a very short half-life of only 15 to 20 minutes. Cagrilintide is molecularly modified to extend that duration to approximately one week, enabling convenient once-weekly subcutaneous dosing. It is currently in Phase 3 clinical development and represents the first next-generation amylin therapy to reach this stage.
Cagrilintide binds to amylin receptors and calcitonin receptors — primarily in the brainstem and hypothalamus — where it activates both homeostatic and hedonic satiety pathways. This dual activation signals fullness through brain regions controlling both biological hunger regulation and reward-driven eating. It slows gastric emptying to prolong post-meal satiety, reduces post-meal blood glucose spikes, and suppresses appetite through central nervous system pathways distinct from those targeted by GLP-1 receptor agonists. This is its key differentiating feature — it activates a completely separate satiety pathway from semaglutide and other GLP-1s, which is the mechanistic basis for combining the two.
Clinical trial results are among the most impressive seen in obesity pharmacotherapy. In the Phase 3 REDEFINE 1 trial of over 3,400 adults with obesity or overweight without type 2 diabetes, cagrilintide monotherapy at 2.4 mg once weekly achieved an average body weight reduction of 11.8% over 68 weeks compared to 2.3% in the placebo group, with 31.6% of treated patients achieving more than 15% weight loss. The combination of cagrilintide with semaglutide 2.4 mg — known as CagriSema — produced even more striking results, achieving mean weight reductions of 20.4 to 22.7% at 68 weeks, with 53.6% of patients achieving at least 20% weight loss and 34.7% achieving at least 25% weight loss. In REDEFINE 2 in patients with type 2 diabetes, CagriSema achieved 15.7% mean weight reduction with 73.5% of patients achieving HbA1c of 6.5% or below. These results significantly surpassed semaglutide monotherapy.
Semaglutide activates GLP-1 receptors in the hypothalamus — reducing appetite, suppressing glucagon, stimulating insulin, and slowing gastric emptying through one pathway. Cagrilintide activates amylin and calcitonin receptors in the brainstem — enhancing satiety through a separate, complementary pathway. Because they target different receptor systems and different brain regions, their effects on appetite reduction appear genuinely additive rather than merely overlapping. This dual-pathway suppression of hunger creates a stronger and more sustained satiety signal than either compound can achieve alone, which is why CagriSema has produced weight loss results approaching or exceeding surgical outcomes in some trial populations.
Cagrilintide is given as a once-weekly subcutaneous injection using a prefilled autoinjector pen. Doses studied in trials range from 0.3 mg to 4.5 mg, with 2.4 mg being the primary dose in Phase 3 trials. A gradual titration schedule is used — starting at lower doses and increasing over several weeks — to minimize gastrointestinal side effects during the adjustment period. When used as CagriSema, both components are injected on the same day once weekly.
The side effect profile closely mirrors that of GLP-1 therapies. The most common are gastrointestinal — nausea affecting 20 to 47% of participants depending on dose, constipation, diarrhea, vomiting, and abdominal discomfort — all of which are typically mild to moderate in severity and improve as patients adjust and titrate gradually. Injection site reactions including redness and mild irritation are also reported. Gallbladder-related events are a potential concern with rapid weight loss, consistent with the class effects seen with GLP-1 therapies. Serious adverse events are rare across Phase 2 and 3 trials, and the drug was generally well tolerated even at the highest studied doses.
Pregnant or breastfeeding women should not use it as it has not been evaluated in these populations. Those with severe renal impairment should use caution pending further safety data. People with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia type 2 should avoid it, consistent with class precautions for amylin and GLP-1 based therapies. As it is currently only available through Phase 3 clinical trial participation, access outside of formal trial settings is not yet possible through legitimate pharmaceutical channels.
Related Products





