



Tesamorelin
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Tesamorelin (Egrifta): A Peptide With a Real Clinical History, Not the Vibe of "Yet Another Anti-Aging Miracle"
Tesamorelin is a synthetic analogue of GHRH, developed not for abstract "biohacking," but as a peptide with a clear scientific rationale and a specific clinical history. In clinical studies in adults with HIV-associated lipodystrophy, it demonstrated statistically significant reductions in visceral fat, and in a research context has also been studied in the areas of liver fat and cognitive function.
Its distinguishing feature is that it does not introduce growth hormone from outside, but within the context of study stimulated the pituitary to produce it in a natural pulsatile rhythm — and it is precisely this that makes the molecule especially interesting for those who prefer not magic, but well-reasoned biology.
At the same time, an important boundary must be drawn clearly: beyond the approved indication begins not a "ready-made solution," but a zone of off-label use and preliminary data. If you need a peptide not with loud promises, but with a clear mechanism, Phase III trials, and a transparent regulatory status, tesamorelin certainly deserves attention.
Tesamorelin (Egrifta): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Tesamorelin is the most clinically rigorously validated GHRH analogue ever developed. Where sermorelin has a historical approval for paediatric GHD that was commercially withdrawn in 2008, tesamorelin has two large, randomised, double-blind, placebo-controlled Phase 3 trials in 806 patients, meta-analysis evidence from five RCTs, a Phase 2 RCT in NAFLD, FDA approval since 2010, and a new improved formulation approved in March 2025.[4]
The pharmacological engineering behind tesamorelin is clever. Endogenous GHRH has a plasma half-life of approximately 7 minutes because DPP4 cleaves it at the Tyr-Ala bond near the N-terminus. Theratechnologies’ solution: conjugate a trans-3-hexenoic acid (C6 fatty acid chain with a double bond at position 3) to the N-terminal tyrosine residue, creating steric hindrance that blocks DPP4 access. The result is a GHRH analogue with a half-life of approximately 26 minutes — sufficient for once-daily SC dosing to produce meaningful pulsatile GH stimulation while preserving somatostatin feedback regulation.
The approved indication — excess abdominal fat in HIV-infected adults with lipodystrophy — is specific and well-defined. Tesamorelin directly addresses a functional GH axis deficiency in this population and produces 15–20% VAT reduction in patients without other approved treatment options. The off-label interest in general visceral fat reduction and body composition is clinically comprehensible but lacks Phase 3 RCT evidence in the general population.
| At a glance | |
|---|---|
| INN / Generic name | Tesamorelin |
| Brand name | Egrifta; Egrifta SV; Egrifta WR (March 2025) |
| Structure | Full 44-amino acid human GHRH sequence + N-terminal trans-3-hexenoic acid modification |
| Molecular weight | 5,135.9 Da (free base) |
| Developer | Theratechnologies Inc. (Montreal, Canada) |
| Mechanism | GHRH receptor agonist → pulsatile GH secretion → visceral lipolysis via IGF-1 and direct GH effects |
| FDA approval | ✅ November 2010 (original Egrifta); ✅ March 2025 (Egrifta WR) |
| Approved indication | Reduction of excess abdominal fat in HIV-infected adults with lipodystrophy |
| EMA status | Not approved (US and Canada only) |
| WADA status | ❌ Prohibited — S2 (Growth Hormone Secretagogues) |
The Problem: HIV-Associated Lipodystrophy
HIV-associated lipodystrophy emerged in the late 1990s as a common and disfiguring complication of highly active antiretroviral therapy (HAART), particularly protease inhibitors. The syndrome has two components: central fat accumulation (visceral abdominal fat, dorsocervical fat, breast enlargement) and peripheral fat wasting lipoatrophy (loss of fat from face, buttocks, and extremities). Visceral adipose tissue is not merely cosmetic — it is an active endocrine organ producing inflammatory adipokines and contributing to insulin resistance, dyslipidaemia, and cardiovascular risk.
The GH axis contribution: mean GH levels, basal GH concentrations, and GH pulse amplitude are reduced in HIV-infected men with body-fat changes receiving ART, compared with men without body-fat changes and healthy control subjects. Nearly half (48%) of lipodystrophic patients did not achieve an adequate GH response to GHRH. This functional GH deficiency — driven by hypothalamic GHRH under-secretion and/or pituitary desensitisation — closely parallels and likely contributes to the visceral fat accumulation. Restoring pulsatile GH secretion through a GHRH agonist directly addresses the upstream endocrine defect.
Structure: Engineering DPP4 Resistance
Human GHRH is a 44-amino acid peptide with Tyr-Ala at positions 1-2. DPP4 (dipeptidylpeptidase-4; the enzyme also targeted by sitagliptin/gliptin diabetes drugs) cleaves the bond between positions 2 and 3, generating an inactive GHRH fragment. DPP4 is abundant in plasma, liver, and intestinal epithelium, resulting in a native GHRH half-life of approximately 7 minutes.
Tesamorelin consists of a synthetically produced 44-amino acid sequence of human GHRH with a hexenoyl moiety attached to the tyrosine residue at the amino terminus. The trans-3-hexenoic acid group (a C6 unsaturated fatty acid) is conjugated to the N-terminal tyrosine, sterically blocking DPP4 access to the Tyr-Ala cleavage site while preserving full GHRHR binding activity and somatostatin feedback regulation. The result: half-life extended from ~7 minutes to approximately 26 minutes. This is a fundamentally different engineering strategy from sermorelin (truncation to minimal active fragment) or CJC-1295 (amino acid substitutions + albumin binding) — tesamorelin retains the complete GHRH sequence; stability comes from a small N-terminal chemical modification alone.[9]
Mechanism of Action
Tesamorelin binds to the GHRH receptor (GHRHR) on pituitary somatotroph cells with the same affinity as endogenous GHRH. GHRHR is a class B GPCR coupling to Gαs → adenylyl cyclase → cAMP → PKA → calcium influx → GH vesicle exocytosis. Tesamorelin stimulates pulsatile GH secretion that mirrors the physiological pattern. The somatostatin feedback axis remains intact: if GH rises above physiological levels, somatostatin from the hypothalamus suppresses further GH release — preventing sustained supraphysiological GH exposure. GH then drives IGF-1 synthesis and release from the liver, mediating fat mobilisation from visceral adipocytes through hormone-sensitive lipase (HSL) activation via cAMP-PKA.
Why visceral fat is selectively affected
Tesamorelin preferentially reduces visceral fat while having minimal effect on subcutaneous fat. This visceral selectivity reflects fundamental adipocyte biology: visceral adipocytes have higher GH receptor density and are more lipolytically responsive to catecholamines and GH; the portal circulation drains visceral fat directly to the liver, making hepatic fat exposure particularly sensitive to visceral adipocyte activity. Reducing visceral fat specifically addresses the metabolically active fat compartment (which drives cardiovascular risk) while preserving subcutaneous fat, lean mass, and peripheral fat distribution.
The Egrifta WR Formulation (March 2025)
A new formulation — Egrifta WR (F8 formulation) — was approved by the FDA in March 2025. The F8 formulation provides daily dosing for 7 days from a single reconstitution, replacing the previous daily preparation requirement. Tesamorelin F8 maintains bioequivalence to the original tesamorelin formulation and requires less than half the injection volume of its predecessor. The underlying pharmacology and therapeutic profile are unchanged; the clinical advantage is reduced treatment burden and improved adherence in a patient population already managing complex antiretroviral regimens.[2]
Pivotal Phase 3 Clinical Evidence
The pooled analysis of two pivotal Phase 3 trials (LIPO-010 and a second North American trial; Falutz et al., JCEM, 2010; N=806): 26-week main phase (randomised, double-blind, placebo-controlled) + 26-week extension phase. Population: HIV-infected adults with lipodystrophy receiving stable antiretroviral therapy. Primary endpoint: change in visceral adipose tissue area (VAT) by CT scan at the L4-L5 level.[4]
Discontinuation finding: Patients switched from tesamorelin to placebo at 26 weeks re-accumulated VAT to near-baseline levels within the extension period, confirming the need for continuous therapy — the effect is maintained but not sustained after withdrawal, consistent with tesamorelin treating an underlying GH deficit rather than permanently remodelling fat distribution.
2025 Meta-analysis
Five RCTs evaluating tesamorelin were included. Tesamorelin was associated with significant reduction in visceral adipose tissue (MD = −27.71 cm², 95% CI [−38.37, −17.06]; P<0.001). Tesamorelin improves body composition, hepatic fat, lean body mass, and IGF-1 levels in HIV-associated lipodystrophy, without serious side effects or perturbation of glucose.[6]
Beyond HIV: NAFLD and Liver Fat
Stanley et al., Lancet HIV, 2019 (N=61): 61 men and women with HIV-infection and hepatic fat fraction (HFF) ≥5% by proton MRS were randomised to tesamorelin 2 mg/day vs. placebo for 12 months. Tesamorelin reduced HFF compared to placebo with an absolute effect size of −4.1% (95% CI −7.6, −0.7; P=0.02), corresponding to a −37% relative reduction.[7]
Additional outcomes: patients with higher NAFLD Activity Scores (NAS) at baseline had greater NAS score reductions; tesamorelin appeared to prevent fibrosis progression — a critical endpoint because fibrosis stage is the primary predictor of NAFLD mortality; CRP reduction; and ALT reduction in patients with elevated baseline ALT. Treatment with tesamorelin reduced liver fat content and reduced the progression of liver fibrosis in people with HIV who had non-alcoholic fatty liver disease. The liver fat reduction is mechanistically explained by GH axis restoration suppressing de novo hepatic lipogenesis and increasing lipolysis.
This finding is important beyond HIV: NAFLD affects approximately 25–38% of the general population and has only recently gained its first approved therapies (resmetirom, semaglutide ). A Phase 2 trial for non-HIV NAFLD was registered (NCT03375788) but general-population approval has not been achieved.
Cognitive Effects
Baker et al. (Archives of Neurology, 2012): A randomised trial of GHRH administration in adults with mild cognitive impairment and healthy older adults found improved verbal memory and executive function. This cognitive data is for GHRH administration rather than tesamorelin specifically, but given tesamorelin’s mechanism of GHRH receptor agonism, the findings are directly relevant. Proposed mechanisms include GH/IGF-1 effects on hippocampal neurogenesis, BDNF signalling, and synaptic plasticity. These findings have driven community interest in tesamorelin for age-related cognitive decline — a use that has not been tested in Phase 2/3 trials for tesamorelin specifically.[10]
Comparison: Tesamorelin vs. Sermorelin vs. rhGH
| Feature | Tesamorelin | Sermorelin | rhGH |
|---|---|---|---|
| Amino acids | 44 (full GHRH + hexenoic acid) | 29 (truncated GHRH fragment) | 191 (complete GH) |
| FDA approval | ✅ Yes (HIV lipodystrophy, 2010) | Historical (paediatric; withdrawn 2008) | ✅ Yes (multiple indications) |
| Phase 3 RCT data | ✅ Yes (N=806 + additional trials) | No (for adult indications) | Extensive |
| NAFLD data (RCT) | ✅ Yes (N=61, Lancet HIV) | No | Limited |
| DPP4 resistance | ✅ Yes (trans-3-hexenoic acid) | No | N/A |
| Somatostatin feedback | Preserved | Preserved | Bypassed |
| Supraphysiological GH risk | Very low (pituitary-regulated) | Very low | Real at higher doses |
| Half-life | ~26 minutes | ~11–12 minutes | ~0.5–1 hour (SC) |
| WADA | ❌ Prohibited | ❌ Prohibited | ❌ Prohibited |
The community preference for sermorelin (primarily on cost grounds, as compounded sermorelin is cheaper) is understandable economically, but the evidence base unambiguously favours tesamorelin for body composition endpoints.
Safety
Most common adverse reactions (Phase 3 data, N=740): hypersensitivity reactions (rash, urticaria — resolved in most patients with continued treatment or dose interruption); oedema-related reactions (peripheral oedema, arthralgia, extremity pain, muscle pain — consistent with GH/IGF-1 class effects); and injection site reactions (erythema, pruritus, pain — typically mild and transient).
⚠️ IGF-1 elevation and monitoring: Tesamorelin raises IGF-1 above the upper limit of normal in a subset of patients. IGF-1 monitoring is recommended, with dose adjustment or interruption if levels exceed the age-appropriate normal range. Elevated IGF-1 is associated with arthralgia, myalgia, and uncommon carpal tunnel syndrome; a theoretical long-term cancer risk concern exists.
⚠️ Glucose metabolism: Tesamorelin causes mild impairment of glucose tolerance in some patients — a class effect of GH/IGF-1 elevation. Patients who developed diabetes were more likely in the tesamorelin group than placebo in the Phase 3 trials. Regular HbA1c monitoring is indicated. The 2025 meta-analysis found no population-level glucose perturbation, but individual patients may develop glucose abnormalities — the absence of population-level signal does not eliminate individual risk.[6]
Anti-tesamorelin antibody formation: IgG antibodies developed in approximately 56% of patients after 26 weeks, with ~60% showing cross-reactivity with endogenous GHRH. Antibody formation did not significantly reduce VAT-reduction efficacy or IGF-1 response, suggesting neutralising activity is limited. Contraindications: active malignancy; pituitary tumours or prior pituitary surgery/radiation; pregnancy (teratogen warning from rat data); hypersensitivity to tesamorelin.
Common Misconceptions
“Tesamorelin is just a more potent sermorelin.”
This is a category error. Tesamorelin is the full 44-amino acid GHRH sequence with an N-terminal modification; sermorelin is a truncated 29-amino acid fragment. The pharmacokinetic profiles differ (26 min vs. 11 min half-life), the clinical evidence is entirely different in quality and quantity, and tesamorelin has FDA approval based on Phase 3 trials while sermorelin’s approval for adults was never established. They share a receptor (GHRHR) but are not pharmacological equivalents.
“Tesamorelin is approved for general visceral fat reduction.”
The FDA approval is specifically for HIV-infected adults with lipodystrophy. Off-label use in non-HIV patients is legal with a physician prescription but is not supported by Phase 3 evidence in that population and is not covered by insurance.
“Because tesamorelin is FDA-approved, it’s safe for everyone.”
FDA approval is indication-specific. The safety data comes from HIV-infected adults with lipodystrophy receiving antiretroviral therapy — a population with specific metabolic characteristics. The safety profile in healthy adults without HIV-related GH axis dysregulation is less well-characterised.
Frequently Asked Questions
Why is tesamorelin approved in the US but not in Europe?
Theratechnologies pursued FDA approval for the HIV lipodystrophy indication but did not pursue the EMA approval pathway with equal priority. Regulatory approval is a business decision as much as a scientific one — the relatively small affected population and specialised indication make parallel regulatory filings economically constrained.
Can tesamorelin be used for general body composition improvement without HIV?
Off-label prescribing is legal in the US. The mechanistic rationale is sound — visceral fat in non-HIV individuals involves similar GH axis changes with obesity and aging. The clinical evidence for this use, however, rests primarily on extrapolation from the HIV lipodystrophy data. No Phase 3 trial has been conducted in a non-HIV population for this indication.
How does the Egrifta WR formulation change clinical practice?
The F8 formulation’s main advantage is convenience — once-weekly reconstitution instead of daily preparation reduces treatment burden and is expected to improve adherence. The pharmacological effect is identical to the original formulation.[2]
Key Takeaways
- ✅ Tesamorelin has the strongest clinical evidence base of any GHRH analogue currently available. Two Phase 3 RCTs in 806 patients, five RCTs in meta-analysis, a Phase 2 RCT in NAFLD, and 15 years of post-marketing safety data in the approved population — this is a rigorously validated compound.[4][6]
- The trans-3-hexenoic acid modification is pharmacologically elegant. Preserving the complete GHRH sequence while blocking DPP4 cleavage at the N-terminus achieves DPP4 resistance without altering GHRHR binding — a targeted engineering solution that preserves receptor selectivity and the somatostatin feedback architecture.
- Visceral fat selectivity is a genuine and pharmacologically important property. The preferential reduction of visceral (not subcutaneous) fat reflects fundamental adipocyte biology and addresses the metabolically active fat compartment that drives cardiovascular risk.
- ✅ The NAFLD/liver fat data is clinically significant and medically underappreciated. A 37% relative reduction in liver fat with prevention of fibrosis progression in a population without approved NAFLD therapy (Lancet HIV, 2019) is a meaningful finding that deserves attention in the broader NAFLD field.[7]
- ⚠️ Off-label use requires honest acknowledgement of the evidence gap. The mechanistic rationale for general visceral fat reduction in non-HIV adults is sound; the Phase 3 evidence supporting this use in the general population does not exist.
References
FDA Approval and Regulatory
- FDA approval of Egrifta (tesamorelin) for HIV-associated lipodystrophy. November 2010. NDA 022505.
- FDA approval of Egrifta WR (tesamorelin F8 formulation). March 2025.
- Egrifta WR full prescribing information. Accessdata FDA. 2025.
Pivotal Phase 3 Trials
- Falutz J, Mamputu J-C, Potvin D, et al. Effects of tesamorelin (TH9507), a growth hormone-releasing factor analog, in HIV-infected patients with excess abdominal fat: a pooled analysis of two multicenter, double-blind, placebo-controlled Phase 3 trials with safety extension data. Journal of Clinical Endocrinology & Metabolism. 2010;95:4291–4304.
- Falutz J, Allas S, Blot K, et al. Metabolic effects of a growth hormone-releasing factor in patients with HIV. New England Journal of Medicine. 2007;357(23):2359–2370.
Meta-analysis
- Body composition, hepatic fat, metabolic, and safety outcomes of tesamorelin, a GHRH analogue, in HIV-associated lipodystrophy: a meta-analysis of randomised controlled trials. ScienceDirect. Published 2026. (Five RCTs through July 2025)
NAFLD
- Stanley TL, Feldpausch MN, Oh J, et al. Effects of tesamorelin on non-alcoholic fatty liver disease in HIV: a randomised, double-blind, multicentre trial. Lancet HIV. 2019. PMC6981288
- Stanley TL, Feldpausch MN, Oh J, et al. Effect of tesamorelin on visceral fat and liver fat in HIV-infected patients with abdominal fat accumulation: a randomised clinical trial. JAMA. 2014;312(4):380–389.
Pharmacology and Structure
- Growth hormone and tesamorelin in the management of HIV-associated lipodystrophy. Journal of the International AIDS Society. 2011. PMC3218714
Cognitive Effects
- Baker LD, Barsness SM, Borson S, et al. Effects of growth hormone-releasing hormone on cognitive function in adults with mild cognitive impairment and healthy older adults. Archives of Neurology. 2012;69(11):1420–1429.
Key Investigators
- Julian Falutz, MD — McGill University Health Centre, Montreal; led the pivotal Phase 3 trials and long-term safety extension data.
- Steven K. Grinspoon, MD — Massachusetts General Hospital; Harvard Medical School; principal investigator of the NAFLD trials; leader in HIV metabolic complications research.
- Theratechnologies Inc. — Montreal, Canada; developer of tesamorelin and the trans-3-hexenoic acid modification; holds the patents and maintains the Egrifta brand.
Certificate of Analysis
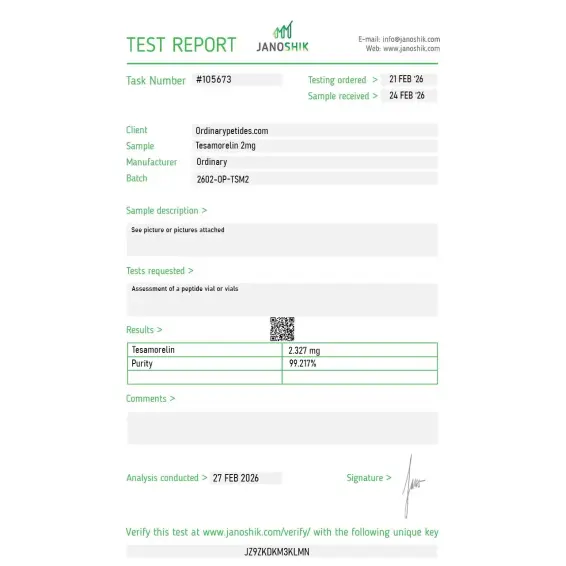
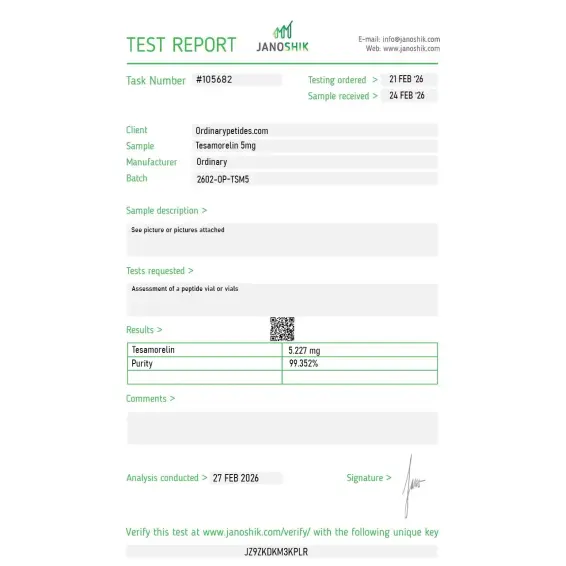
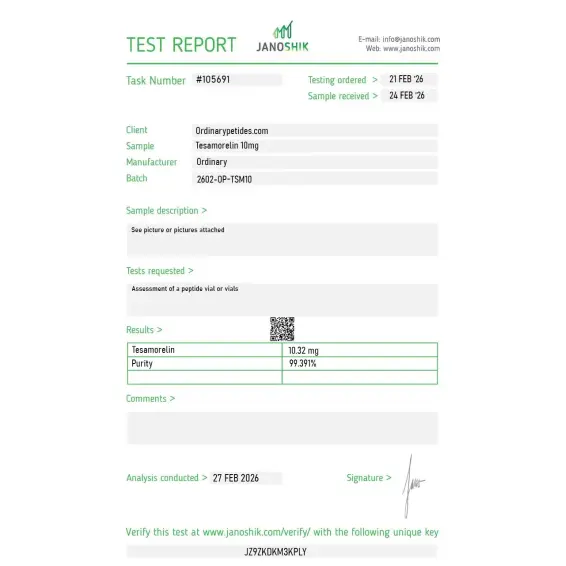
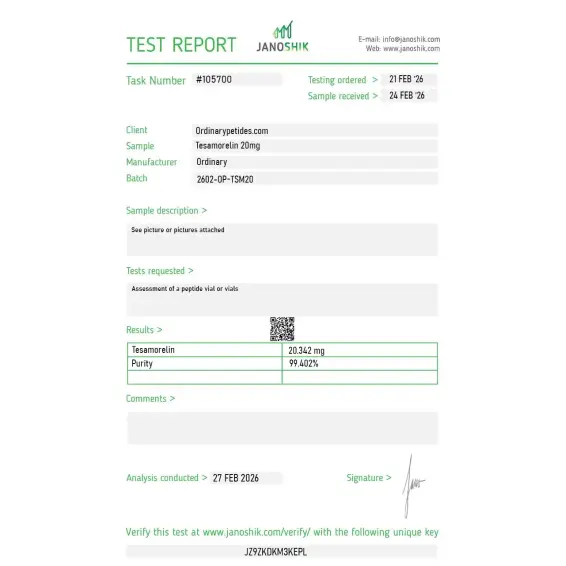
Independent test reports are available for Tesamorelin 2mg, 5mg, 10mg, and 20mg. These reports provide batch-level documentation and analytical verification information for research reference.



The pricing on this is genuinely reasonable for what's structurally the most complex GHRH analog in this class — synthesizing a 44-residue peptide with a defined N-terminal modification is meaningfully harder than the 29-residue fragments, and the price-to-complexity ratio here is more favorable than at the major pharma reagent suppliers we've used historically.
The 44-residue length matters for receptor-binding geometry research — tesamorelin retains the full extracellular receptor-engaging region of native GHRH while the truncated analogs lose portions of that interface. For studying GHRH receptor-ligand interaction at high resolution, the full-length analog with stability modifications is the structurally-relevant tool. The material gave consistent receptor engagement in our binding kinetics work
The reconstituted solution is more viscous than typical GHRH analogs at our working concentration, which initially made me suspect aggregation — turned out to be normal for full-length tesamorelin once I checked against published handling notes, but the unexpected viscosity caused a few minutes of concern. Not the vendor's issue, just compound behavior, but a one-line note about reconstituted-solution viscosity for newer researchers would prevent the moment of doubt. Material was fine.
Tesamorelin is a synthetic 44-amino acid polypeptide analogue of growth hormone releasing hormone (GHRH). Its N-terminal portion has been modified to improve stability and pharmacokinetics compared to native GHRH. It is marketed under the trade name Egrifta™ and was the first FDA-approved treatment specifically indicated for lipodystrophy.
Tesamorelin activates GHRH receptors in the pituitary, which leads to synthesis and release of growth hormone. That growth hormone then stimulates production of insulin-like growth factor-1 (IGF-1), which mediates many downstream effects including lipolysis. A key distinction is its selectivity for visceral adipose tissue (VAT) — the metabolically active fat around internal organs.
Tesamorelin injection is used to decrease the amount of extra fat in the stomach area in adults with HIV who have lipodystrophy (increased body fat in certain areas of the body). Importantly, it is not used to help with general weight loss.
Tesamorelin is also being evaluated as therapy for insulin resistance, obesity, and nonalcoholic fatty liver disease. Research also explores its potential for age-related conditions including muscle wasting, decreased bone density, and cognitive decline, as growth hormone levels naturally decline with age.
Tesamorelin comes as a powder to be mixed with a provided liquid and injected subcutaneously (under the skin) once a day, at around the same time each day. It should be injected into the stomach area below the navel, avoiding scarred, irritated, or previously injected areas.
Side effects can include injection site reactions, itching, arthralgia, myalgia, and peripheral edema. Potential rare adverse events include stimulation of malignant tumor growth, glucose intolerance, diabetes, and hypersensitivity reactions. Using tesamorelin during pregnancy can harm an unborn baby, and it may cause changes in blood sugar levels requiring monitoring.
Its growth hormone-stimulating properties make it unsafe for people with active cancer, and its action on the pituitary gland means it is unsuitable for people with a pituitary gland disorder. Current research has also not established its safety for women who are pregnant or breastfeeding. People who have had radiation therapy to the head or brain, recent head trauma, or pituitary gland surgery or tumors should also inform their doctor before use.
The pivotal evidence comes from two large Phase 3 randomized double-blind placebo-controlled trials — LIPO-010 and CTR-1011 — enrolling a combined 806 HIV-infected patients with excess abdominal adiposity. In these trials tesamorelin 2 mg daily produced visceral adipose tissue reductions of approximately 15 to 20% over 26 weeks compared to minimal change with placebo — with the LIPO-010 trial showing 19.6% VAT reduction and CTR-1011 showing 11.7%, both reaching statistical significance. Subcutaneous fat was largely spared, confirming the selective visceral effect. Secondary endpoints showed meaningful reductions in triglyceride levels and improvements in glucose homeostasis markers in responders. These effects were not durable after discontinuation — VAT returned toward baseline when tesamorelin was stopped, indicating the requirement for ongoing therapy to maintain benefit. Research into off-label applications has documented benefit in non-alcoholic fatty liver disease with reductions in liver fat content, and studies in non-HIV populations with excess visceral adiposity show similar VAT reduction signals though without FDA approval for these populations.





