






Ipamorelin
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Ipamorelin: A Selective GH Secretagogue With Real Research Interest
Ipamorelin is a short synthetic peptide from the GH secretagogues class that, in the research context, attracted attention because of its idea of more selectively stimulating GH release through the ghrelin receptor. In early studies, it appeared more refined than some older GHRPs in terms of hormonal response profile, and in published human PK/PD data it showed clear and measurable pharmacological activity.
In preclinical data, it was also studied in models of growth and GI motility, so this is not a "peptide from nowhere," but a molecule with a real scientific biography. The most interesting thing here is not in loud promises, but in the fact that ipamorelin looks like an intelligently designed research tool for studying the GH axis and ghrelin signaling.
If peptides interest you not by the principle of "wow, it promises everything," but by the principle of "there is a clear rationale, early human pharmacology, and a real scientific track record," ipamorelin definitely deserves attention. In short: not magic, not a universal life hack, but a careful and intriguing candidate for research interest.
Ipamorelin Acetate: A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Ipamorelin occupies a pharmacologically unusual position in the GHRP class: it is simultaneously the cleanest, best-tolerated, and least clinically validated member of the group. It is the compound that virtually everyone in the peptide wellness community recommends, and the one with the least evidence.
Ipamorelin’s defining characteristic — established in the original 1998 Novo Nordisk paper — is selective GH release without the ACTH, cortisol, and prolactin stimulation that all previous GHRPs produced. Ipamorelin did not release ACTH or cortisol in levels significantly different from those observed following GHRH stimulation, even at doses more than 200-fold higher than the ED&sub5;&sub0; for GH release.[1] This was a genuine advance over GHRP-6, GHRP-2, and hexarelin.
That clinical development happened — once, for one indication. Helsinn Therapeutics ran a Phase 2 randomised controlled trial of ipamorelin for postoperative ileus (POI) in 117 patients. Ipamorelin was well tolerated. The directional effect (25.3 vs. 32.6 hours to first tolerated meal) was not statistically significant (p = 0.15), and the programme did not advance.[5] Ipamorelin was then handed to the compounding pharmacy and wellness clinic market, where it became the dominant GHRP in community use — often combined with CJC-1295 in a stack designed to simultaneously activate both arms of GH pulse amplification. This combination is widely used, widely recommended, and has never been evaluated in a controlled clinical trial.
| At a glance | |
|---|---|
| INN | Ipamorelin |
| Sequence | Aib-His-D-2-Nal-D-Phe-Lys-NH&sub2; |
| Class | Pentapeptide growth hormone secretagogue (GHRP); 3rd-generation GHRP |
| Developer | Novo Nordisk (Denmark); development code NNC 26-0161 |
| Molecular weight | ~711 Da |
| Key pharmacological distinction | GHS-R1a agonist with no significant ACTH/cortisol/prolactin elevation — unique among GHRPs |
| Human clinical data | Phase 2 POI trial (N=117): well tolerated; primary endpoint not met |
| Minimal desensitisation | Confirmed in comparative studies — significantly slower than hexarelin |
| FDA status | ⚠️ Not approved; Category 2 bulk substance (compounding concerns) |
| WADA | ❌ Prohibited at all times (S2) |
Development History: Novo Nordisk’s Chemistry Programme
Ipamorelin emerged from a deliberate drug design effort at Novo Nordisk in the mid-1990s aimed at improving on GHRP-1 and GHRP-6 by stripping away the features that produced off-target hormonal effects. The central design insight: the Ala-Trp dipeptide at positions 3–4 of GHRP-1, present in all first-generation GHRPs, was responsible for much of the ACTH/cortisol activation. Removing this dipeptide while maintaining the key structural pharmacophore for GHS-R1a activation produced a series of truncated pentapeptides, of which ipamorelin (NNC 26-0161) demonstrated the optimal profile.[1]
Novo Nordisk subsequently developed tabimorelin from ipamorelin as an orally bioavailable next-generation compound. Tabimorelin reached Phase 2 trials for GHD but was found to inhibit CYP3A4 — a drug-drug interaction concern that effectively ended the programme. Ipamorelin itself was licensed to Helsinn Healthcare for gastrointestinal applications and reached Phase 2 — the only completed controlled human trial of ipamorelin.[4]
Chemistry
Ipamorelin is a pentapeptide where three of the five residues are non-standard: Aib (α-aminoisobutyric acid) provides metabolic stability by resisting N-terminal aminopeptidases; D-2-Nal (D-2-naphthylalanine) is the large hydrophobic D-amino acid key for GHS-R1a binding; D-Phe contributes both protease resistance and receptor binding; Lys-NH&sub2; (C-terminal amide) prevents exopeptidase degradation. Despite being five amino acids vs. GHRP-6’s six, the structural simplification reduces molecular weight (~711 Da vs. ~873 Da for GHRP-6) while maintaining receptor activation capability.
Mechanism of Action
GHS-R1a activation: comparable potency to GHRP-6
Ipamorelin activates the ghrelin receptor (GHS-R1a) on anterior pituitary somatotroph cells through the same Gq/11 pathway as all GHRPs: phospholipase C → IP&sub3;/DAG → intracellular Ca²+ rise → GH secretion. In vitro, ipamorelin released GH from primary rat pituitary cells with a potency and efficacy similar to GHRP-6 (EC&sub5;&sub0; = 1.3 ± 0.4 nmol/L and Emax = 85 ± 5% vs. 2.2 ± 0.3 nmol/L and 100%).[1] The GH pulse peaks at approximately 30–40 minutes post-injection and returns to baseline within 2–3 hours, mimicking natural pulsatile GH secretion.
Selectivity: the defining pharmacological feature
None of the GH secretagogues tested affected FSH, LH, PRL, or TSH plasma levels. Administration of both GHRP-6 and GHRP-2 resulted in increased plasma levels of ACTH and cortisol. Ipamorelin did not release ACTH or cortisol in levels significantly different from those observed following GHRH stimulation — even at doses more than 200-fold higher than the ED&sub5;&sub0; for GH release.[1] Ipamorelin also produces only minimal appetite stimulation, in contrast to GHRP-6’s pronounced NPY/AgRP pathway activation.
Gastrointestinal effects: a separate receptor population
Ipamorelin activates GHS-R1a in the enteric nervous system, accelerating gastric emptying in rodent POI models through a ghrelin receptor-mediated mechanism involving cholinergic excitatory neurons.[6] This GI prokinetic activity is the basis for the Helsinn clinical programme — pharmacologically distinct from the pituitary GH-releasing effect.
GHRH synergy
Like all GHRPs, ipamorelin acts synergistically with GHRH when co-administered, producing GH pulses substantially larger than either agent alone. GHRH activates GHRH-R via cAMP (pressing the accelerator); ipamorelin/GHRPs activate via Gq/phospholipase C and suppress hypothalamic somatostatin tone (releasing the brake). Combining them therefore produces near-maximal GH pulsatile amplitude while preserving physiological feedback — the pharmacological basis for the CJC-1295/ipamorelin community protocol.[7]
Desensitisation: The Minimal Tachyphylaxis Advantage
One of ipamorelin’s most practically relevant properties is its substantially reduced desensitisation rate compared to hexarelin and, to a lesser extent, GHRP-2. Comparative studies confirmed that ipamorelin produces a sustained GH response over weeks of administration with minimal attenuation, while hexarelin shows 50–75% GH response reduction over the same period.[3] The mechanistic basis: ipamorelin’s lower intrinsic efficacy at GHS-R1a (Emax 85% vs. GHRP-6’s 100% in vitro) means it drives less receptor internalisation and less compensatory somatostatin upregulation per dose. The compound that produces slightly less GH per dose but maintains that response for months is likely to produce more total GH secretion over a 12-week period than one that starts higher and rapidly declines.
Clinical Evidence
Foundational pharmacodynamics (Gobburu et al. 1999)
IV administration in healthy human volunteers produced a measurable GH increase peaking at approximately 40 minutes, with rapid return to baseline. Cortisol, ACTH, and prolactin were not significantly elevated — confirming in humans the selectivity demonstrated in swine. The compound was well tolerated, with no serious adverse events.[2] This was a PK/PD characterisation study, not a therapeutic trial.
The Phase 2 POI trial: the only completed efficacy trial
Helsinn Healthcare sponsored a Phase 2 randomised, double-blind, placebo-controlled trial (NCT00672074) in patients undergoing small and large bowel resection. IV ipamorelin 0.03 mg/kg twice daily vs. placebo, postoperative day 1 to 7 or hospital discharge. 117 patients enrolled; 114 in the analysis populations.
Median time to first tolerated meal was 25.3 hours (ipamorelin) vs. 32.6 hours (placebo). There were no significant differences between ipamorelin and placebo in the key and secondary efficacy analyses (p = 0.15). Ipamorelin 0.03 mg/kg twice daily for up to 7 days was well tolerated.[5] The 7.3-hour directional difference was clinically meaningful in direction but did not reach statistical significance. The programme did not advance to Phase 3.
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) | ❌ Not approved for any indication |
| FDA — compounding (503A) | ⚠️ Category 2 bulk drug substance — insufficient evidence of clinical use; compounding concerns [7] |
| FDA — compounding (503B) | ❌ Not on the 503B bulks list |
| FDA enforcement | Warning letters issued to pharmacies and wellness clinics marketing ipamorelin (2024–2025) |
| WADA | ❌ Prohibited at all times — S2 (Peptide Hormones, Growth Factors) |
The FDA’s PCAC review noted substantial real-world compounding use since at least 2017, but determined that ipamorelin does not meet standards for inclusion on either the 503A or 503B lists, based primarily on the failed POI clinical trial, the absence of any approved indication, and the lack of controlled clinical evidence for the GH-secretagogue applications in which it is primarily used.[7]
The CJC-1295/Ipamorelin Combination
The pharmacological rationale is sound. CJC-1295 (a GHRH analogue with albumin-binding modification for extended half-life) activates GHRH-R → cAMP → pituitary GH priming and release. Ipamorelin activates GHS-R1a and additionally suppresses hypothalamic somatostatin tone. These mechanisms are genuinely complementary and synergistic — analogous to simultaneously releasing the brake and pressing the accelerator on GH pulse generation.
⚠️ The clinical evidence for the combination is absent. No randomised trial of CJC-1295/ipamorelin vs. placebo for any outcome has been published in humans. No pharmacokinetic interaction, additive or synergistic adverse effects, or long-term hormonal consequences have been assessed. Any clinical recommendations for this combination are based on mechanistic inference, not controlled trial evidence.
Safety
What is established from clinical data
From the POI trial and the Gobburu PK/PD study: well tolerated at the doses studied; no ACTH or cortisol elevation confirmed in humans; no prolactin elevation; no LH, FSH, or TSH effects; injection site reactions are the primary local adverse effect.[2][5] The absence of cortisol elevation means no adrenal suppression concern with prolonged use and no catabolic counter-regulation that would partially negate the anabolic GH effects.
What is not established
Long-term safety beyond weeks of use; safety of the CJC-1295/ipamorelin combination; cancer risk from chronically elevated IGF-1 (the same concerns that apply to all GH secretagogues); effects in women including on gonadal function during reproductive cycles; safety in insulin-resistant or diabetic individuals (given the anti-insulin effects of chronically elevated GH).
Comparison: Ipamorelin vs. the GHRP Class
| Feature | Ipamorelin | GHRP-2 | GHRP-6 | Hexarelin |
|---|---|---|---|---|
| Peak GH potency | Moderate (comparable to GHRP-6) | High | Moderate | Highest |
| Cortisol/ACTH elevation | ✅ None — unique | Yes (dose-dependent) | Yes | Yes (dose-dependent) |
| Prolactin elevation | ✅ None/minimal | Yes | Yes | Yes |
| Appetite stimulation | ✅ Minimal | Moderate | Strong | Mild-moderate |
| Desensitisation rate | ✅ Slowest | Moderate | Moderate | ⚠️ Fastest |
| GI motility effects | Yes (studied in POI) | Limited data | Limited data | Limited data |
| Cardioprotection (CD36) | Not characterised | Limited | Yes (via class) | ✅ Confirmed |
| Human clinical trials | Phase 2 POI (N=117; failed efficacy) | Phase 3 (Japan — diagnostic use) | Extensive pharmacology | Phase 2 (unpublished) |
| Regulatory approval | ❌ None | Japan (diagnostic) | ❌ None | ❌ None |
Common Misconceptions
“Ipamorelin is the safest GHRP because it has no side effects.”
Ipamorelin has the most favourable short-term hormonal side effect profile among GHRPs. It does not follow that it has no risks. Long-term IGF-1 elevation, the absence of any Phase 3 clinical trial, and the lack of long-term safety data mean that “no known side effects in short-term studies” should not be conflated with “safe for extended use.”
“CJC-1295/ipamorelin is clinically validated.”
⚠️ The pharmacological rationale for the combination is sound. The clinical validation does not exist. No controlled trial of this combination has been published.
“Ipamorelin was FDA-approved for gut motility.”
It was never approved. It was studied for postoperative ileus and failed to meet its primary endpoint. FDA Category 2 classification reflects insufficient clinical evidence, not approval.[8]
“Because ipamorelin doesn’t raise cortisol, it won’t modify natural GH secretion.”
Ipamorelin still modifies GHS-R1a receptor dynamics and the GHRH/somatostatin balance during and after a treatment period. The effects are milder than hexarelin but not zero.
Frequently Asked Questions
Why didn’t the POI trial work?
The trial was described as a “proof of concept” study — smaller than a pivotal trial, and explicitly powered with the expectation of demonstrating a signal rather than definitive efficacy. The directional difference (7.3 hours faster meal tolerance) suggests biological activity, but the study may have been underpowered (N=114) or enrolled a heterogeneous patient population. A second POI trial was registered (NCT01280344) — suggesting Helsinn believed the signal was worth pursuing — but its results were not published.
Is the subcutaneous form equivalent to the IV form used in the clinical trial?
Different routes of administration produce different pharmacokinetic profiles. The IV infusions in the POI trial produced a different exposure pattern than subcutaneous injection. Pharmacokinetic bridging studies between these two forms in healthy adults have not been published.
Does ipamorelin affect bone density?
Svensson et al. (2000) demonstrated in rats that chronic GHRP treatment including ipamorelin increases bone mineral content — an effect attributed to IGF-1 elevation from sustained GH secretion.[3] Whether this translates to clinically meaningful effects on human bone mineral density has not been tested.
Key Takeaways
- Ipamorelin’s defining pharmacological achievement is GHS-R1a agonism without ACTH/cortisol elevation — demonstrated in the foundational Raun et al. 1998 paper and confirmed in humans.[1] This selectivity was a genuine advance over all previous GHRPs.
- ⚠️ It is the most widely used GHRP in the wellness community — frequently combined with CJC-1295 — but this widespread use is not supported by controlled clinical evidence for body composition, sleep, anti-ageing, or any of the other applications for which it is prescribed.
- ⚠️ The only completed controlled human trial failed its primary endpoint. The Phase 2 POI trial in 114 patients showed a directional but statistically non-significant reduction in time to meal tolerance. The development programme did not advance.[5]
- Ipamorelin’s minimal desensitisation is a genuine pharmacological advantage for extended protocols compared to hexarelin. It produces sustained GH pulsatility over weeks with minimal tachyphylaxis.[3]
- ⚠️ The FDA’s Category 2 classification reflects the evidentiary reality: insufficient controlled clinical data to support compounding for any indication, despite years of widespread compounding use.[7]
- The CJC-1295/ipamorelin combination has sound pharmacological rationale and has become the community standard, but has never been evaluated in a controlled clinical trial. Any clinical recommendations are based on mechanistic inference, not randomised trial evidence.
References
Foundational Pharmacology
- Raun K, Hansen BS, Johansen NL, Thogersen H, Madsen K, Ankersen M, Andersen PH. Ipamorelin, the first selective growth hormone secretagogue. European Journal of Endocrinology. 1998;139(5):552–561. PMID: 9849822
- Gobburu JVS, Agersø H, Jusko WJ, Aarons L. Pharmacokinetic-pharmacodynamic modelling of ipamorelin, a growth hormone releasing peptide, in human volunteers. Pharmaceutical Research. 1999;16(9):1412–1416.
- Svensson J, Lall S, Dickson SL, et al. The GH secretagogues ipamorelin and GHRP-6 increase bone mineral content in adult female rats. Journal of Endocrinology. 2000;165(3):569–577.
Clinical Development History
- Ishida J, Saitoh M, Ebner N, et al. Growth hormone secretagogues: history, mechanism of action, and clinical development. JCSM Rapid Communications. 2020;3(1):25–37. doi: 10.1002/rco2.9
POI Clinical Trial
- Beck DE, et al. Prospective, randomized, controlled, proof-of-concept study of the ghrelin mimetic ipamorelin for the management of postoperative ileus in bowel resection patients. International Journal of Colorectal Disease. 2014;29(12):1527–1534. PMID: 25331030
- Greenwood-Van Meerveld B, et al. Efficacy of ipamorelin, a ghrelin mimetic, on gastric dysmotility in a rodent model of postoperative ileus. Journal of Experimental Pharmacology. 2012. PMC4863553
Regulatory
- FDA PCAC Briefing Document — Ipamorelin Acetate. October 2024. fda.gov/media/182088/download
- FDA. Certain Bulk Drug Substances for Use in Compounding that May Present Significant Safety Risks (Category 2). fda.gov
Key Investigator
- Kjeld Raun, PhD — Novo Nordisk, Denmark; lead author on the 1998 ipamorelin characterisation paper; primary contributor to establishing ipamorelin’s selective pharmacological profile.
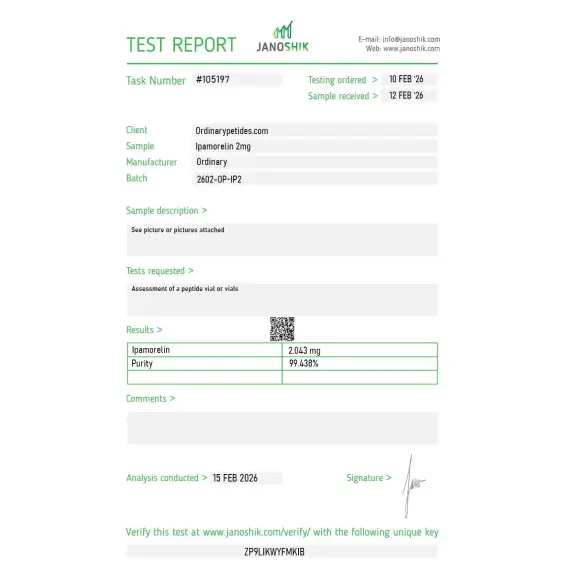
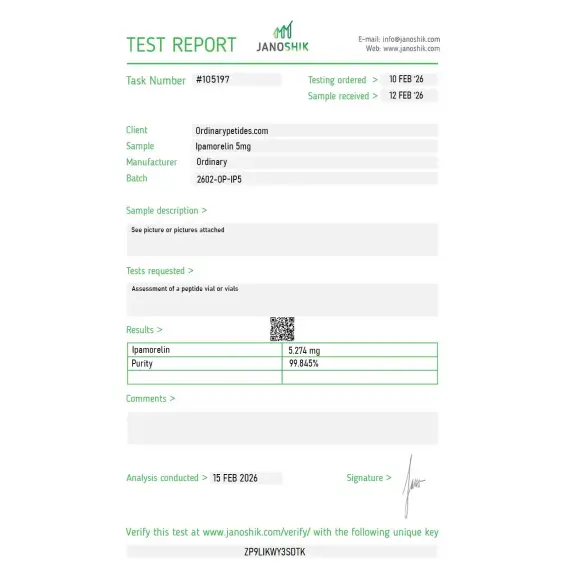
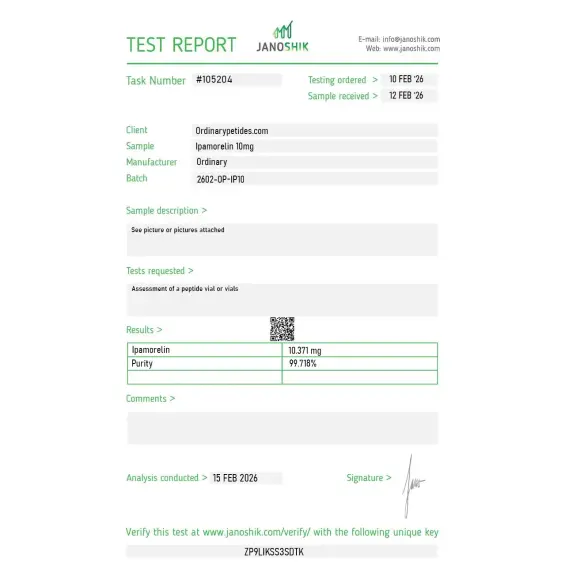
Certificate of Analysis
Independent test reports are available for Ipamorelin 2mg, 5mg, and 10mg batches. These reports provide batch-level documentation and analytical verification information for research reference.
What earned the order is that the listing acknowledges the selectivity is sometimes overstated — Ipamorelin is cleaner than GHRP-2 and GHRP-6 but it's still a ghrelin-mimetic with some weak prolactin elevation at higher concentrations, not a perfect single-receptor agonist. That honest qualification rather than the "clean GHRP" oversimplification is what signals the vendor understands the actual pharmacology. For receptor-pathway work where I need the cleaner secretagogue with realistic expectations about its limits, that framing was the deciding factor.
Good that the listing identifies Ipamorelin by the IUPAC sequence rather than just "GHRP-type peptide," but it could go further and note the synthesis-difficulty implications — the three non-standard residues make Ipamorelin meaningfully more demanding to manufacture cleanly than the L-amino-acid GHRPs, which is part of why batch-to-batch quality varies more across vendors for this compound than for simpler peptides. A buyer should know synthesis complexity is part of the QC landscape here. Material itself was reliable.
We use Ipamorelin in a chronic-exposure desensitization study where its selectivity matters experimentally — extended GHS-R1a activation without the confounding HPA-axis activation that the dirtier secretagogues introduce. For studying receptor downregulation kinetics in isolation from the stress-axis crosstalk, the cleanness of Ipamorelin's profile is what makes the experiment interpretable. The material held its selective activation across our timecourse without drift into off-target pathways.
The Aib at position 1 is the structural feature people skip past — alpha-aminoisobutyric acid is a non-proteinogenic amino acid that locks helical conformation and confers protease resistance, and it's part of why Ipamorelin survives long enough in serum to be useful where most natural pentapeptides wouldn't. For studying Aib-containing peptide design as a stabilization strategy, Ipamorelin is a clean worked example of the substitution applied to a bioactive sequence. The material behaved with the expected stability profile in our extended-incubation assays.
Ipamorelin is a synthetic pentapeptide — five amino acids — with the sequence Aib-His-D-2-Nal-D-Phe-Lys-NH₂. It was developed in the late 1990s as a third-generation growth hormone releasing peptide (GHRP) specifically engineered to address the selectivity limitations of the earlier GHRPs — GHRP-6 and GHRP-2 — which stimulated GH release alongside unwanted elevations in cortisol, prolactin, and ACTH. Ipamorelin was the first GHRP designed from the outset for near-complete hormonal selectivity, retaining potent GH-releasing activity while producing negligible effects on any other pituitary hormone. It is not FDA-approved for any therapeutic indication, cannot be legally compounded in the United States, and is banned by WADA.
No. Ipamorelin is not growth hormone itself. It works by stimulating the body to release its own endogenous growth hormone.
Early studies suggested that Ipamorelin had a more selective growth hormone-release profile, with less effect on ACTH and cortisol than some older growth hormone-releasing peptides.
Yes. Human studies have included a PK/PD study in healthy volunteers and a clinical study in postoperative ileus.
No. There is no convincing clinical evidence showing that Ipamorelin is a proven treatment for anti-aging, athletic performance, or body recomposition.
No. Based on the official materials cited, Ipamorelin is not FDA-approved.
The sequence commonly listed for Ipamorelin is Aib-His-D-2-Nal-D-Phe-Lys-NH2. Product and chemical reference sources consistently identify it as a 5-amino-acid peptide.
Ipamorelin is listed with the molecular formula C38H49N9O5 and a molecular weight of about 711.8 to 711.9 g/mol, depending on source rounding.
Ipamorelin is commonly supplied as a lyophilized powder. Some product pages also list it simply as powder, but the standard research-product format is lyophilized peptide material.
Storage guidance varies slightly by source, but consistent recommendations are to keep Ipamorelin desiccated and frozen below about -18°C to -20°C, protect it from light, and avoid repeated freeze-thaw cycles. One product source also states that, after reconstitution, it may be stored at 4°C for 2 to 7 days, with longer-term storage below -18°C
Commercial research-product listings commonly state that Ipamorelin is for research use only and not for human use. Some vendors also explicitly say it is not intended for human or veterinary use and is not for diagnostic or therapeutic procedures.
Ipamorelin binds to and activates GHS-R1a — the ghrelin receptor — on somatotrope cells in the anterior pituitary gland and in the hypothalamus. This binding triggers calcium ion influx and downstream signaling that drives pulsatile GH release. Simultaneously it inhibits somatostatin, the natural brake on GH secretion, thereby amplifying and prolonging each GH pulse. Unlike GHRP-2 and GHRP-6, Ipamorelin's activation of GHS-R1a does not substantially cross-activate the pathways responsible for ACTH, cortisol, or prolactin release — its selectivity appears to stem from specific structural features that allow high affinity for GHS-R1a without the non-selective neuroendocrine activation of earlier compounds. It does not act through GHRH receptors — it is pharmacologically distinct from CJC-1295, Sermorelin, and Tesamorelin.
This is the most clinically important comparison in the GHRP class. GHRP-6 produces the most pronounced appetite stimulation and the broadest cortisol and prolactin elevation. GHRP-2 is more potent than GHRP-6 for GH release and somewhat more selective, but still produces meaningful cortisol and prolactin elevation. Ipamorelin produces GH pulses of similar or slightly lower amplitude than GHRP-2 but with no meaningful cortisol, prolactin, ACTH, or appetite stimulation at standard doses — making it the preferred GHRP for most body composition and optimization protocols where minimizing cortisol exposure is important. Hexarelin is more potent than Ipamorelin for GH stimulation but has the same cortisol and prolactin liability as GHRP-2 and the added receptor desensitization risk. For long-term wellness and optimization protocols Ipamorelin's safety and tolerability profile is unmatched in the GHRP class.
CJC-1295 No DAC activates GHRH receptors — a completely separate receptor system from GHS-R1a. GHRH receptor activation primes pituitary somatotropes and increases the pool of releasable GH, while GHS-R1a activation through Ipamorelin provides the trigger to fire that release. When both receptors are activated simultaneously the resulting GH pulse is 2 to 10 times larger than either compound produces alone — true dual-pathway synergy rather than simple addition. This combination closely mimics the natural physiology in which the hypothalamus uses both GHRH and ghrelin-like signals to coordinate each GH pulse. The short half-lives of both compounds — approximately 30 minutes — ensure the combined GH pulse is sharp and physiologically timed, preserving the pulse-and-rest rhythm that protects receptor sensitivity over time.
Through GH and downstream IGF-1 elevation Ipamorelin is associated with improved body composition including increased lean muscle mass and reduced fat particularly visceral fat, enhanced recovery from exercise and injury, improved deep slow-wave sleep quality — often reported as one of the first and most noticeable effects — increased energy and vitality, improved skin quality and collagen synthesis, bone density support, and connective tissue repair. In clinical research Ipamorelin has also been studied for its effects on gastrointestinal motility — it has been investigated as a treatment for postoperative ileus, with Phase 2 clinical trial data showing accelerated return of gastrointestinal function after surgery.
Ipamorelin is given by subcutaneous injection. Standard doses range from 200 to 300 mcg per injection, typically once to three times daily. Like all GHRPs it should be injected on an empty stomach — at least two hours after eating and at least 30 minutes before the next meal — as insulin from food blunts GH release. Bedtime injection is particularly effective for amplifying the natural nocturnal GH surge. When used in the CJC-1295 / Ipamorelin stack both peptides are drawn into the same syringe and injected together. It is supplied as lyophilized powder reconstituted with bacteriostatic water.
People with active cancer or a history of cancer should not use it given IGF-1's established mitogenic role. Those with diabetes or significant insulin resistance should exercise caution as GH elevation can worsen glucose metabolism. People with pituitary tumors or acromegaly should not use it. Pregnant or breastfeeding women should not use it. Competitive athletes subject to WADA testing are prohibited from its use — it is listed under Peptide Hormones, Growth Factors, and Related Substances and is banned at all times. It cannot be legally compounded in the United States following FDA Category 2 designation.





