



GHRP-6
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
GHRP-6: A Classic GH Secretagogue With Strong Research Biology and a Clear Logic of Action
GHRP-6 is one of the classic growth hormone-releasing peptides — a peptide which, in the research context, sharply stimulated the release of endogenous GH through the ghrelin/GHSR pathway, rather than acting as growth hormone itself.
In early human studies, it showed a strong acute GH response, and in combination with GHRH it often produced an even more pronounced synergy — which is precisely why it is so important for understanding neuroendocrine physiology. In published observations, GHRP-6 affected not only GH, but also other hormonal axes, making it a molecule with a broader pharmacological footprint than its name alone might suggest.
Its value lies in the fact that this is not some theoretical molecule from internet forums, but a genuinely studied GH secretagogue with clearly noticeable effects in research. GHRP-6 helps show how elegantly the growth system works at the level of the experimental model, without unnecessary myths or marketing fog. A peptide with real physiology is usually more interesting than a peptide with only dramatic promises — science does tend to prefer data over drama.
If you are interested in peptides with strong research biology and a clear logic of action, GHRP-6 is definitely not among the boring ones.
GHRP-6 (Growth Hormone Releasing Peptide-6): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
GHRP-6 has a unique position in growth hormone secretagogue pharmacology: it came first. Developed in 1984 by Cyril Y. Bowers at Tulane University, it was the founding member of the GHRP class — the synthetic peptide that opened the entire field. Every subsequent compound in the series (GHRP-2, hexarelin, ipamorelin, MK-677, anamorelin) descends conceptually from GHRP-6.[1]
Three features define GHRP-6 and distinguish it from its successors. First, it is the prototypical ghrelin mimetic: its appetite stimulation is not a quirky side effect — it is mechanistically central, making it the strongest appetite driver of any GHRP. Second, it has a second receptor, CD36, giving it a cytoprotective dimension that none of its successors fully replicate. Third, the cytoprotection is preclinical: the cardioprotective and organ-protective effects, while mechanistically compelling, remain almost entirely in animal models and have not been validated in controlled human trials.
| At a glance | |
|---|---|
| INN | None (no therapeutic approval) |
| Sequence | His-D-Trp-Ala-Trp-D-Phe-Lys-NH&sub2; |
| Development code | SKF-110679 |
| Class | First-generation synthetic hexapeptide GHRP |
| Molecular weight | ~873 Da |
| First characterised | 1984 (Bowers et al., Endocrinology) |
| Primary receptor | GHS-R1a (ghrelin receptor) |
| Second receptor | CD36 (scavenger receptor; mediates cytoprotective effects) |
| Key defining property | Strongest appetite stimulation of any GHRP |
| Off-target effects | ACTH, cortisol, prolactin (intermediate degree) |
| FDA status | ❌ Not approved; research compound only |
| WADA | ❌ Prohibited at all times (S2) |
Historical Significance: The Compound That Started It All
From morphine to growth hormone
Bowers and colleagues were not, initially, looking for a GH secretagogue. They were studying synthetic analogues of met-enkephalin — the endogenous opioid pentapeptide. In the course of this structure-activity work, they discovered that certain modifications produced an unexpected and potent effect in rat pituitary cell cultures: GH release, through a mechanism entirely unrelated to opioid receptors. Through systematic structure-activity relationship studies, GHRP-6 was developed and characterised in 1984 in Endocrinology as the first synthetic peptide to specifically and dose-dependently release GH both in vitro and in vivo through a mechanism entirely distinct from GHRH.[1]
The 12-year receptor mystery and ghrelin’s discovery
GHRP-6 generated an orphan receptor problem: a compound with demonstrable, potent, specific activity through a receptor no one had yet cloned. The receptor was cloned in 1996 by Howard et al. from pituitary and hypothalamic tissue.[3] The endogenous ligand — ghrelin — was isolated in 1999 by Kojima et al. from rat stomach.[4] Ghrelin turned out to have a primary physiological role in hunger signalling, explaining retroactively why GHRP-6 and all other GHRPs caused appetite stimulation. GHRP-6, in other words, had been mimicking the biology of a hunger hormone for fifteen years before that hormone was discovered.
Chemistry and Structure
GHRP-6’s sequence is: His – D-Trp – Ala – Trp – D-Phe – Lys – NH&sub2;. The D-configured tryptophan at position 2 is essential for GHS-R1a binding — all subsequent GHRPs preserve a D-amino acid at this position, usually with modifications to increase potency. The histidine at position 1 differentiates GHRP-6 from GHRP-2 (which has D-Ala at position 1) and reduces GHRP-6’s receptor binding affinity relative to GHRP-2, explaining its lower GH potency per unit dose. C-terminal amidation (–NH&sub2;) protects against carboxypeptidase degradation. Plasma half-life is approximately 15–20 minutes — the shortest of the classical GHRPs.[12]
Mechanism of Action
Receptor 1: GHS-R1a — the ghrelin receptor
GHRP-6 binds with moderate-high affinity to GHS-R1a, expressed on anterior pituitary somatotrophs (GH release via Gq/11 → PLC → IP&sub3; → Ca²+ → exocytosis), hypothalamic arcuate nucleus NPY/AgRP neurons (appetite stimulation via the orexigenic pathway), and peripheral tissues including the heart, adrenal, thyroid, and adipose tissue.[2]
The GHRH dependence finding
A critical mechanistic discovery clarified GHRP-6’s in vivo action: a substantial portion of its GH-releasing effect requires endogenous hypothalamic GHRH. In nine healthy men, GHRH antagonist administration eliminated most of the GH response to GHRP-6 (maximal increase over baseline: 33.8 ± 4.8 vs. 6.2 ± 1.8 µg/L; p < 0.0001), showing that endogenous GHRH is necessary for most of the GH response to GHRP-6 in humans.[6] This explains why combining GHRP-6 with a GHRH analogue produces synergistic — not merely additive — GH release.
The appetite mechanism: not a side effect
GHRP-6’s appetite-stimulating effect is mediated through GHS-R1a on arcuate nucleus neurons, activating NPY and AgRP neurons — the primary orexigenic pathway in the brain. The hunger is not a problem to be managed: it is ghrelin receptor pharmacology doing exactly what the ghrelin system does. Ghrelin rises before meals, signals hunger, and falls after eating. GHRP-6 activates this same signal. For cachexia research, this is therapeutic; for body composition protocols in adequately nourished adults, it is a significant liability.
Receptor 2: CD36 — the cytoprotective receptor
CD36 is a scavenger receptor (class B) expressed broadly across multiple tissue types — cardiomyocytes, hepatocytes, renal tubular cells, macrophages, platelets, and keratinocytes in wound granulation tissue. GHRP-6 binds the ectodomain of CD36, activating survival signalling cascades — particularly PI3K/AKT/Bcl-2 — that protect cells against apoptosis under ischaemic, toxic, or inflammatory stress. This CD36-mediated cytoprotection is GH-independent: it occurs in tissues regardless of whether GHS-R1a is present.[5]
| CD36 action | Mechanism |
|---|---|
| Cardioprotection | PI3K/AKT pro-survival; Ca²+ inotropic effect without chronotropy |
| Anti-fibrosis | PPARγ upregulation → TGF-β/CTGF/PDGF downregulation |
| Anti-inflammation | NFκB blunting → reduced pro-inflammatory cascade |
| Wound healing | Accelerated closure; reduced hypertrophic scarring via PPARγ |
| Hepatoprotection | Reduced liver fibrosis; LPS-attenuation of transaminases |
| Cell survival | HIF-1α induction; Bcl-2 upregulation; Bax downregulation |
Preclinical Evidence: The Cytoprotection Programme
The most scientifically distinctive body of GHRP-6 research is the cytoprotection and cardioprotection work, primarily from Cuba’s Center for Genetic Engineering and Biotechnology (CIGB).
Cardiac ischaemia and myocardial infarction
In a porcine acute myocardial infarction model, Berlanga et al. (2006) demonstrated that GHRP-6 reduced infarct mass by 78% and preserved wall thickness by 50% compared with saline, while decreasing oxidative stress markers and preserving antioxidant reserves.[7] This is a remarkable effect size in a large-animal model of a condition where cardioprotective drugs have consistently failed in Phase 3 trials.
Doxorubicin cardiotoxicity (2024)
A 2024 study in Frontiers in Pharmacology demonstrated that GHRP-6 prevented doxorubicin (an anthracycline chemotherapy agent) from inducing myocardial and extra-myocardial damage in rats. The cytoprotection extended broadly to hepatocytes, kidney tubular cells, and bronchial epithelia — consistent with the broad tissue distribution of the CD36 receptor.[9]
Wound healing (Mendoza Marí et al., 2016)
Topical GHRP-6 gel (400 µg/mL) applied twice daily to excisional full-thickness wounds in rats dramatically reduced the onset of exuberant scars by activating PPARγ and reducing the expression of fibrogenic cytokines. GHRP-6 showed no effect on the reversion of consolidated lesions.[8]
Hepatoprotection and liver fibrosis
Multiple CIGB studies demonstrated that GHRP-6 reduces liver fibrotic induration in CCl4-intoxicated rats, attenuates LPS-induced hepatocyte damage, and reduces transaminase and inflammatory marker elevation. This hepatoprotective effect appears to operate through PI3K/AKT signalling independent of the GH axis.[10]
Limitations of the preclinical evidence
All of this evidence is in animals — rats, rabbits, pigs, hamsters. None of it has been validated in controlled human trials. The CIGB has conducted Phase I/II studies in Cuba, but these have not been published in major peer-reviewed Western journals, preventing independent evaluation of methodology and outcomes. The concentration of research in one institution warrants the same caveat that applies to BPC-157 and Epithalon.
Human Evidence: The GH Secretagogue Data
GH stimulation in healthy adults (Bowers et al., 1990)
The foundational human GHRP-6 paper showed robust GH stimulation in normal men following IV GHRP-6 administration, with effects synergistic with GHRH.[2] Peak GH increases of 10–30-fold over baseline are documented across healthy adult studies, with effects appearing within 15–30 minutes and normalising within 60–90 minutes.
The GHRH/GHRP-6 combined stimulation test
A major clinical application of GHRP-6 is the GHRH/GHRP-6 combined stimulation test for GH deficiency diagnosis, validated in multiple European and Latin American centres. This combined test — administering both GHRH and GHRP-6 simultaneously — produces a stronger, more reproducible GH response than either alone, improving diagnostic sensitivity and specificity. It is considered by some endocrinologists superior to the insulin tolerance test because it combines potency with a better safety profile (no risk of hypoglycaemia).
Pharmacokinetics in healthy males (Fernandez-Perez et al., 2013)
A formal pharmacokinetic study in nine healthy male volunteers established GHRP-6’s biphasic profile: a rapid distribution phase of approximately 7.6 minutes, followed by an elimination phase of approximately 2.5 hours.[12] This confirms that despite GHRP-6’s short half-life, the compound persists in tissues at pharmacologically relevant concentrations for substantially longer than the plasma half-life suggests.
Human evidence summary
| Study type | Design | Key finding |
|---|---|---|
| GH stimulation (normal men) [2] | Multiple studies, IV/SC | 10–30-fold GH increase; synergistic with GHRH |
| GHRH/GHRP-6 combined test | Diagnostic validation | Superior diagnostic sensitivity for GHD vs. single agents |
| Pharmacokinetics [12] | 9 healthy males | Biphasic: t½α 7.6 min; t½β 2.5 hours |
| GHRH dependence [6] | 9 healthy men, GHRH antagonist | Endogenous GHRH necessary for most of GH response |
| Cardioprotection (Phase I/II, Cuba) | Not fully published in Western journals | Anecdotal positive reports; not formally evaluable |
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) | ❌ Not approved; not on 503A or 503B bulks lists; research compound only |
| Japan (PMDA) | ❌ Not approved (pralmorelin/GHRP-2 is approved for GH diagnostics; GHRP-6 is not) |
| EMA (Europe) | ❌ Not approved |
| Cuba (CIGB) | Investigational (Phase I/II); used in limited compassionate/investigational contexts |
| WADA | ❌ Prohibited at all times — S2 (Growth Hormone Secretagogues) |
Comparison with Other GH Secretagogues
| Feature | GHRP-6 | GHRP-2 | Ipamorelin | Hexarelin | MK-677 |
|---|---|---|---|---|---|
| Class | 1st gen hexapeptide | 2nd gen hexapeptide | 3rd gen pentapeptide | 2nd gen hexapeptide | Non-peptide |
| GH potency per dose | Moderate | Higher | Moderate-high | Highest | High |
| Appetite stimulation | Strongest | Moderate | Minimal | Moderate | Moderate |
| ACTH/Cortisol elevation | Intermediate | Intermediate | None ✅ | Strongest | Mild |
| CD36 cytoprotection | ✅ Yes | Limited | ❌ No | Yes | No |
| Oral bioavailability | Low | Low | No | No | >60% |
| Approved anywhere | ❌ No | Japan (diagnostic) | ❌ No | ❌ No | ❌ No |
Safety Profile
Well-characterised acute effects
Cortisol elevation: Intermediate (between ipamorelin’s zero and hexarelin’s pronounced). Dose-dependent, transient, within physiological range at standard doses. Prolactin elevation: Present, moderate, dose-dependent, transient. Appetite increase: Clinically significant. The 20–30% increase in food intake is not trivial for protocols where caloric control matters. For cachexia research, it is therapeutically useful; for body composition protocols in normally fed adults, unmanaged it can contribute to unintended caloric surplus. Flushing/injection site reactions: Common, transient.
Important nuances
GH axis feedback intact: Like all secretagogues, somatostatin rises in response to GH elevation, limiting response duration. This feedback preservation distinguishes GHRP-6 from exogenous rhGH, which produces sustained GH elevation bypassing this regulation. GHRH dependence: GHRP-6 works best when the hypothalamic-pituitary axis is intact — patients with hypothalamic damage show severely blunted responses.[6] Desensitisation: More pronounced with GHRP-6 than with ipamorelin, which is one reason cycling is conventionally recommended.
Long-term safety
No controlled long-term human safety study of GHRP-6 exists. The compound has not entered formal clinical development in Western regulatory environments. The theoretical risks associated with chronic GH axis elevation — insulin resistance, fluid retention, increased cancer risk in susceptible individuals — apply as with all GH secretagogues.
Common Misconceptions
“GHRP-6 causes intense hunger because it’s misdosing or a product quality issue.”
The intense hunger is GHS-R1a pharmacology — identical to what ghrelin does before a meal. It is not a formulation defect or dose error. It is the signature effect of activating the ghrelin receptor in the hypothalamus.[4]
“GHRP-6 is weaker than GHRP-2, so it’s inferior.”
GHRP-6 produces somewhat lower peak GH per unit dose than GHRP-2 and has a shorter half-life. But it has CD36-mediated cytoprotective effects that GHRP-2 has in limited form and that ipamorelin entirely lacks.[5] Comparing them as “stronger/weaker” misses the pharmacological distinction between selectivity and pleiotropic activity.
“The cardioprotection data means GHRP-6 is heart-healthy to use.”
The cardioprotective data is in animal models of injury. It does not mean GHRP-6 protects the cardiovascular system of a healthy adult using it for body recomposition. The data is relevant to ischaemia/reperfusion injury contexts — not ongoing preventative use in healthy individuals.[7]
Frequently Asked Questions
Is the GHRH/GHRP-6 combined diagnostic test the same as Japan’s pralmorelin test?
They are different tests. Japan’s approved pralmorelin (GHRP-2) test uses GHRP-2 alone as a single agent. The GHRH/GHRP-6 combined test uses both simultaneously and is not formally approved but is used clinically in some European and Latin American centres as an alternative to the insulin tolerance test.
Why hasn’t GHRP-6’s cardioprotective effect been developed into a drug?
The CIGB group in Cuba has pursued this but faces barriers of publication in major Western journals, limiting uptake by Western pharmaceutical companies. The compound itself (a small peptide without broad patent protection) offers limited commercial incentive. The cardioprotection field generally has a poor record of translating animal findings into human benefit — 30+ years of failed translation. These factors together explain the gap between promising preclinical data and clinical reality.[11]
Does GHRP-6 interact with common medications?
A formal drug interaction study with metoprolol (a beta-blocker) showed no pharmacological interaction. No other formal drug interaction studies have been published. Given its activation of the ACTH-cortisol axis, concomitant use with glucocorticoids warrants consideration.
Key Takeaways
- GHRP-6 is the founding compound of the GHRP class, characterised in 1984 by Bowers at Tulane, and the synthetic peptide that ultimately led to the discovery of ghrelin.[1] It holds a historically significant position in endocrinology research.
- Its appetite stimulation is not a side effect — it is the ghrelin receptor working exactly as intended. The hunger GHRP-6 produces is mechanistically identical to the pre-meal ghrelin surge. For cachexia research, this is therapeutic; for body recomposition in adequately fed adults, it is a liability.
- The CD36 receptor gives GHRP-6 a cytoprotective dimension that its successors lack. The cardioprotection, hepatoprotection, anti-fibrosis, and wound healing data from preclinical models is scientifically compelling and mechanistically coherent — but it is almost entirely animal data.[7][8][9]
- GHRP-6’s GH-stimulating profile is well-characterised in humans across decades of clinical pharmacology — it works robustly, synergistically with GHRH, and within the intact pituitary feedback system.[2]
- No therapeutic approval exists anywhere in the world for GHRP-6. The Japan PMDA approval covers pralmorelin (GHRP-2), not GHRP-6. GHRP-6 remains an unapproved investigational compound in every jurisdiction.
- The compound’s unique value is its CD36 cytoprotection — a biological property worth tracking as the CIGB and other groups continue developing evidence. Whether this ever translates into a therapeutic approval for cardioprotection or wound healing will depend on completing the human trial validation that has so far only been partially conducted.
References
Discovery and Characterisation
- Bowers CY, Momany FA, Reynolds GA, Hong A. On the in vitro and in vivo activity of a new synthetic hexapeptide that acts on the pituitary to specifically release growth hormone. Endocrinology. 1984;114(5):1537–1545.
- Bowers CY, Reynolds GA, Durham D, et al. Growth hormone (GH)-releasing peptide stimulates GH release in normal men and acts synergistically with GH-releasing hormone. Journal of Clinical Endocrinology and Metabolism. 1990;70(4):975–982.
Receptor Biology
- Howard AD, Feighner SD, Cully DF, et al. A receptor in pituitary and hypothalamus that functions in growth hormone release. Science. 1996;273:974.
- Kojima M, Hosoda H, Date Y, et al. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature. 1999;402:656–660.
- Demers A, McNicoll N, Febbraio M, et al. Identification of the growth hormone-releasing peptide binding site in CD36: a photoaffinity cross-linking study. Biochemical Journal. 2004;382:417–424.
GHRH Dependence
- Pandya N, DeMott-Friberg R, Bowers CY, et al. Growth hormone (GH)-releasing peptide-6 requires endogenous hypothalamic GH-releasing hormone for maximal GH stimulation. Journal of Clinical Endocrinology and Metabolism. 1998. PMID: 9543138
Cardioprotection and Cytoprotection
- Berlanga-Acosta J, et al. Cardiac and extracardiac cytoprotective effects of GHRP-6 peptide. Biotecnología Aplicada. 2008.
- Mendoza Marí Y, et al. Growth Hormone-Releasing Peptide 6 Enhances the Healing Process and Improves the Esthetic Outcome of the Wounds. Plastic Surgery International. 2016. PMC4854984
- Sosa-Hernandez V, et al. Growth hormone releasing peptide-6 (GHRP-6) prevents doxorubicin-induced myocardial and extra-myocardial damages by activating prosurvival mechanisms. Frontiers in Pharmacology. 2024. PMC11169835
- Berlanga-Acosta J, et al. Growth hormone-releasing peptide-6 (GHRP-6) and other related secretagogue synthetic peptides: A mine of medical potentialities for unmet medical needs. OAText Immunology. 2017.
Historical Review and Pharmacokinetics
- Berlanga-Acosta J, et al. Synthetic Growth Hormone-Releasing Peptides (GHRPs): A Historical Appraisal of the Evidences Supporting Their Cytoprotective Effects. Clinical Medicine Insights: Cardiology. 2017. PMC5392015
- Fernandez-Perez L, et al. GHRP-6 pharmacokinetics in healthy male volunteers. Clinical Endocrinology. 2013.
Key Investigators
- Cyril Y. Bowers, MD, PhD — Tulane University Medical Center, New Orleans; discoverer of GHRP-6 (1984) and founder of the GHRP field; Monsanto Clinical Investigator Award from the Endocrine Society (1998).
- Jorge Berlanga-Acosta, MD, PhD — Center for Genetic Engineering and Biotechnology (CIGB), Havana, Cuba; principal investigator of the GHRP-6 cardioprotection and cytoprotection programme.
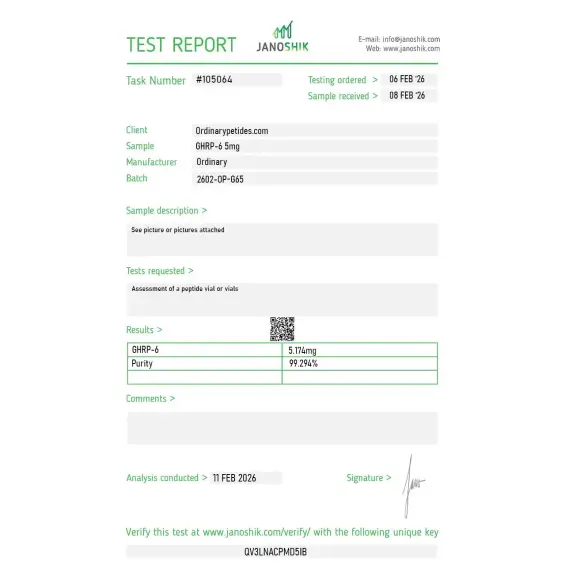
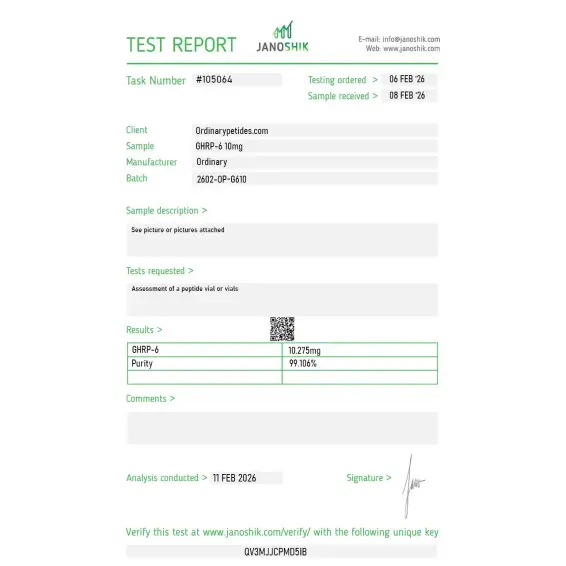
Certificate of Analysis
Independent test reports are available for GHRP-6 5mg and 10mg batches. These reports provide batch-level documentation and analytical verification information for research reference.
The orexigenic profile that defines GHRP-6 depends on the ghrelin-receptor activation being clean, so a contaminating related sequence could quietly shift the appetite-versus-GH balance the compound is supposed to show — and that's exactly why I'd want tighter impurity characterization than a single purity figure. The material behaved with the expected strong appetite signal in our hands, but for a compound whose research value is its specific receptor profile, impurity documentation is what protects the experiment.
We use it as the orexigenic-pathway probe in feeding-circuit work — GHRP-6 drives the appetite signal harder than any other secretagogue in the family, and that strong, reproducible orexigenic activation is precisely what makes it a clean pharmacological handle for the ghrelin-receptor appetite arm. For dissecting feeding behavior at the receptor level, the appetite potency is the feature, not a side effect. The material gave consistent activation in our hypothalamic-circuit assays.
No. It is a peptide that stimulates the release of endogenous GH, but it is not growth hormone itself.
Through the GHSR / ghrelin receptor, not through the classical GHRH receptor.
Yes. That is the best-established effect of GHRP-6 in humans.
Because an acute GH response is not evidence of long-term clinical benefit, and there are few high-quality long-term studies.
No. The literature describes effects on GH, as well as on ACTH/cortisol and certain sleep-related parameters.
In the sources reviewed, there is no confirmation of FDA approval as a broad therapy; on the contrary, the FDA specifically describes risks associated with compounded GHRP-6.
No. WADA includes GHRP-6 on the list of prohibited growth hormone-releasing peptides.
The key point is that GHRP-6 reliably raises GH acutely, but that does not make it a proven, safe, and approved therapy for growth, muscle gain, anti-aging, or athletic progress.
GHRP-6 (Growth Hormone Releasing Peptide-6) is a synthetic hexapeptide — six amino acids — with the sequence His-D-Trp-Ala-Trp-D-Phe-Lys-NH₂. It was one of the earliest growth hormone secretagogues developed, emerging from enkephalin analog research in the 1980s primarily through the work of Cyril Bowers at Tulane University. It was the first GHRP shown to potently stimulate GH release in humans, making it the foundational compound from which the entire GHRP class — including GHRP-2 and Ipamorelin — was developed. It is not approved for therapeutic use by the FDA or any major Western regulatory authority, though it has been used as a research and diagnostic tool for decades.
GHRP-6 and GHRP-2 share the same fundamental mechanism — both bind to GHS-R1a (ghrelin receptors) in the pituitary and hypothalamus, triggering calcium influx and pulsatile GH release, inhibiting somatostatin, and stimulating additional GHRH release from the hypothalamus. The key practical difference is selectivity. GHRP-6 is the least selective of the three main GHRPs — it produces the most pronounced elevations in cortisol, prolactin, and ACTH alongside its GH release, and causes the strongest appetite stimulation of the class, significantly exceeding even GHRP-2 in hunger induction. GHRP-2 was developed specifically as a more potent and somewhat more selective improvement over GHRP-6, and Ipamorelin was engineered later for near-complete selectivity. In terms of GH stimulation potency GHRP-2 surpasses GHRP-6 over prolonged use because GHRP-2 maintains maximum GH elevation more consistently, while GHRP-6's GH release can attenuate faster with repeated dosing.
GHRP-6 has been studied across the broadest range of applications of any GHRP given its longer research history. Body composition research documents increased lean muscle mass, myofiber diameter, and skeletal muscle volume. Appetite stimulation makes it a uniquely relevant research tool and potential therapeutic agent in cachexia, anorexia, and conditions involving pathological muscle wasting — it is one of the most potent appetite-stimulating peptides studied in humans. Sleep quality improvement through amplified nocturnal GH pulses has been documented. Cardioprotective effects have been studied — GHS-R1a receptors in cardiac tissue mediate cytoprotective effects, and GHRP-6 has shown reduced ischemic damage in animal cardiac models. Anti-inflammatory and organ-protective effects including liver protection and anti-fibrotic properties have also been studied. Like other GHRPs it elevates IGF-1, supporting connective tissue, bone, and muscle repair through that downstream pathway.
GHRP-6's hunger-inducing effect is its most practically distinctive characteristic. It is substantially stronger than GHRP-2 and dramatically stronger than Ipamorelin. In research settings GHRP-6 administration reliably produces acute and pronounced hunger within minutes of injection through both central GHS-R1a activation in hypothalamic appetite centers and peripheral ghrelin pathway engagement. This makes it a liability in fat loss or body recomposition protocols where appetite control matters — and a potential asset in clinical contexts involving pathological appetite loss such as cancer cachexia, HIV wasting syndrome, anorexia nervosa, or recovery from severe illness or surgery. This is the domain where GHRP-6's unique profile relative to GHRP-2 and Ipamorelin is most therapeutically interesting.
GHRP-6 is given by subcutaneous or intramuscular injection. Its half-life is short — similar to GHRP-2, peak GH concentrations occur within 15 to 30 minutes and return toward baseline within 60 minutes — requiring dosing two to three times daily. Research protocols typically use doses of 100 to 300 mcg per injection. Like all GHRPs it should be injected on an empty stomach as food and elevated insulin blunt GH release. Bedtime dosing is particularly valued. It synergizes with GHRH analogs such as CJC-1295 No DAC or Mod GRF 1-29 for amplified dual-pathway GH pulses, and the GHRP-6 / GHRH combination has been one of the most extensively studied combinations in clinical endocrinology research.
GHRP-6 has the broadest side effect profile of the three main GHRPs. The most significant is intense and reliable appetite stimulation — this is not a mild effect and can substantially increase caloric intake if not managed. Cortisol elevation is more pronounced than with GHRP-2 and significantly more pronounced than with Ipamorelin. Prolactin elevation can occur and is relevant for individuals with prolactin-sensitive conditions. Water retention, lethargy, and tingling or numbness in the extremities are reported. Injection site reactions are common. The cortisol elevation is a particular concern in protocols aimed at body composition improvement as cortisol promotes fat storage and muscle catabolism — somewhat counteracting the desired GH-driven anabolic effects. For these reasons many practitioners in the GH optimization space prefer GHRP-2 for better GH potency with less cortisol, or Ipamorelin for highest selectivity and cleanest profile.
The same contraindications apply as for all GHRPs. People with active or historical cancer should not use it given IGF-1's role in cell growth. Those with diabetes or insulin resistance should exercise caution as GH elevation worsens glucose control and the pronounced appetite stimulation makes caloric management significantly harder. People with elevated cortisol, Cushing's syndrome, or adrenal conditions should avoid it given its ACTH and cortisol-stimulating effects. Those with elevated prolactin or prolactin-sensitive conditions should avoid it. Competitive athletes are banned from use under WADA. Pregnant or breastfeeding women should not use it. It cannot be legally compounded in the United States under current FDA regulatory designations.





