

Hexarelin Acetate
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Hexarelin Acetate: A Research GHRP at the Intersection of Neuroendocrine and Cardio-Metabolic Biology
Hexarelin acetate is not growth hormone, but a research GHRP peptide with very real endocrine activity and a much less "clean" profile than marketing likes to suggest. In human studies, it reliably stimulated the release of GH, but along with it also raised other hormonal axes — including prolactin, ACTH, and cortisol — so this is not a story about one neat little button.
In the research context, Hexarelin was interesting not only for the study of GH secretagogues, but also for the evaluation of possible cardiotropic effects, although the strongest signals here came mainly from preclinical models and limited human observations. That is exactly what makes it intriguing: the molecule stands at the intersection of neuroendocrine and cardio-metabolic biology, rather than collapsing into the banal category of a "growth peptide."
Strong physiology still does not make Hexarelin a standard therapy for anti-aging, body recomposition, or "safe GH enhancement." It is more a peptide for those who are interested not in a pretty legend, but in a live scientific zone where data do exist — but speculation around them exists even more.
Hexarelin Acetate (Examorelin): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Hexarelin is the most potent GH-releasing peptide (GHRP) characterised in humans. On a per-microgram basis, it produces larger GH pulses than GHRP-6, GHRP-2, or ipamorelin — a consequence of the D-2-methyltryptophan substitution at position 2 of its sequence, which increases GHS-R1a binding affinity and protease resistance.[1]
Two things define hexarelin’s pharmacological identity and make it genuinely unusual within the GHRP class. First, the desensitisation problem: its potency is not a free lunch. Aggressive GHS-R1a activation produces receptor downregulation and hypothalamic somatostatin counter-regulation faster and more completely than any other GHRP studied in humans — a 50–75% reduction in GH response documented within weeks of continuous administration. Second, the CD36 cardiac receptor: hexarelin is the only GHRP with a formally identified second binding site. Rat cardiac membranes were labelled with a radioactive photoactivatable derivative of hexarelin and purified; a binding protein of Mr 84,000 was identified and its N-terminal sequence was determined to be identical to rat CD36.[4] The cardioprotective effects operating through CD36 are independent of GH-releasing activity and persist even when the GH response has become fully desensitised.
| At a glance | |
|---|---|
| INN | Examorelin |
| Common name | Hexarelin |
| Developer | Mediolanum Farmaceutici (Milan, Italy) |
| Sequence | His-D-2-methyl-Trp-Ala-Trp-D-Phe-Lys-NH&sub2; |
| Class | Hexapeptide growth hormone secretagogue (GHRP) |
| Derived from | GHRP-6 (modified at position 2) |
| Molecular weight | ~887 Da |
| Primary receptor | GHS-R1a (ghrelin receptor) |
| Second receptor | CD36 scavenger receptor (cardiac; GH-independent effects) |
| Key feature vs. other GHRPs | Highest potency; fastest desensitisation; unique CD36 cardioprotection |
| Development status | Phase 2 trials completed; discontinued 2005; never marketed |
| FDA status | ❌ Not approved; not on 503A/503B bulks lists |
| WADA | ❌ Prohibited at all times (S2) |
Chemistry and Structure
Hexarelin is derived from GHRP-6 through a single structural modification: the L-tryptophan at position 2 of GHRP-6 is replaced by D-2-methyltryptophan (D-2-MeTrp). The 2-methyl group creates a more favourable steric fit within the GHS-R1a binding pocket, increasing receptor binding affinity. The D-stereochemistry and methyl group together reduce susceptibility to enzymatic degradation, extending the compound’s functional half-life. Despite sharing a receptor with ghrelin, GHRPs including hexarelin have no sequence similarity to ghrelin — they arrived at the same receptor through entirely different structural chemistry.[7]
Mechanism of Action
Primary pathway: GHS-R1a → pituitary GH release
Hexarelin’s primary pharmacological action is via the GHS-R1a, a Gq/11-coupled G-protein receptor expressed most densely on pituitary somatotrophs but also present in hypothalamic neurons, the heart, adrenal glands, adipose tissue, bone, and the gastrointestinal tract. Binding activates phospholipase C → IP&sub3; and DAG → intracellular Ca²+ rise → GH secretion. Hexarelin releases more GH than GHRH in humans, and produces synergistic effects on GH release in combination with GHRH, resulting in dramatically elevated plasma GH levels even with only low doses of examorelin.[1]
Secondary pathway: CD36 → GH-independent cardiovascular effects
The CD36 scavenger receptor is expressed on cardiomyocytes, microvascular endothelial cells, macrophages, and adipocytes. Hexarelin binds CD36 through a mechanism distinct from GHS-R1a signalling. Downstream consequences in cardiac tissue include activation of the PI3K/AKT survival pathway, ERK1/2 phosphorylation, Bcl-2 upregulation, reduced caspase-3 activity, and reduction of TNF-α and IL-1β. Hexarelin has been shown to improve atherosclerotic lesions by binding CD36, preventing the uptake of oxidised low-density lipoproteins — one of the earliest steps in atherosclerotic fatty streak formation.[4]
Cortisol, ACTH, and prolactin release
Like GHRP-2 but unlike ipamorelin, hexarelin dose-dependently stimulates ACTH, cortisol, and prolactin release in humans — a direct consequence of GHS-R1a activation in the HPA axis. Hexarelin does not affect plasma levels of glucose, LH, FSH, or TSH.[2] The cortisol elevation is clinically relevant: in protocols involving sustained or high-dose hexarelin, the cortisol and ACTH effects may counteract the anabolic GH effects and have implications for immune function and glucose handling.
Modulation by sex steroids and age
Testosterone, testosterone enanthate, and ethinylestradiol have been found to significantly potentiate the GH-releasing effects of examorelin in humans. Puberty also significantly augments the GH-elevating actions of examorelin.[7] Visceral adiposity attenuates GH response — consistent with the broader GH secretagogue literature.
Human Pharmacodynamic Data
Dose-response study (Imbimbo et al. 1994)
The foundational human characterisation: IV doses of 0.5, 1.0, and 2.0 µg/kg in 12 healthy young male volunteers. Peak GH at 30 minutes: 26.9 ng/mL (0.5 µg/kg), 52.3 ng/mL (1 µg/kg), 55.0 ng/mL (2 µg/kg) vs. 3.9 ng/mL placebo. The plateau between 1 and 2 µg/kg doses confirms GHS-R1a saturation at approximately 1 µg/kg IV. Half-life approximately 55 minutes. Well tolerated in all subjects; no serious adverse events.[1] The 52–55 ng/mL peak GH values significantly exceed those typically seen with equipotent doses of GHRP-2 or GHRP-6 in similar study designs.
Cortisol, ACTH, and prolactin (Arvat et al. 1997)
The direct comparative study between GHRP-2 and hexarelin in humans, alongside GHRH, TRH, and hCRH, confirmed that both hexarelin and GHRP-2 produced significant dose-dependent ACTH, cortisol, and prolactin elevations alongside the GH response. GHRH produced GH release but essentially no cortisol/ACTH effect — confirming cortisol stimulation is a GHRP-class effect, not a consequence of GH per se.[2]
Long-term desensitisation (Rahim et al. 1998)
The most clinically important human study: a partial and reversible tolerance to the GH-releasing effects of examorelin occurs with long-term administration — a 50–75% decrease in efficacy over the course of weeks to months.[3] Repeated daily administration produced progressive attenuation of peak GH levels, attributed to GHS-R1a receptor downregulation through ligand-induced internalisation, increased hypothalamic somatostatin tone, and negative feedback through elevated IGF-1. Critically, after a 4-week washout, GH responsiveness was restored to near-baseline — confirming that desensitisation is reversible.
Cardiac Evidence
Human cardiac effects: the Bisi et al. study
The most directly relevant human cardiac data: in 7 male volunteers given IV hexarelin vs. rhGH, both compounds elevated circulating GH levels to the same extent. Left ventricular ejection fraction (LVEF) was unaffected by rhGH. Hexarelin increased LVEF (70.7 ± 3.0% vs. 64.0 ± 1.5%; p < 0.03) without significant changes in mean blood pressure or heart rate, with the effect lasting up to 60 minutes.[5] This is the key finding: rhGH and hexarelin produced identical GH elevations, but only hexarelin improved LVEF, directionally confirming that the positive inotropic effect is not GH-mediated.
The same group extended this to 24 men with coronary artery disease undergoing bypass surgery, measuring cardiac function by transoesophageal echocardiography. Hexarelin improved LVEF, cardiac output, and cardiac index. Critically, cardiac improvements occurred in patients whose GH response had already become attenuated through desensitisation — providing early clinical evidence for a GH-independent mechanism and motivating subsequent CD36 pathway research.
Animal cardiac evidence
In rat ischaemia-reperfusion models, hexarelin pretreatment reduces infarct size by 25–50%. This protection was completely abolished in CD36 knockout animals — formally establishing CD36 as the necessary mediator.[4] In a mouse LAD ligation model, hexarelin reduced LV collagen concentration by ~53%, decreased inflammatory cytokines (TNF-α, IL-1β), and shifted autonomic balance toward parasympathetic predominance.[8] Anti-atherosclerotic activity was confirmed in Sprague-Dawley rats: hexarelin suppressed atherosclerotic plaque and neointima formation, partially reversed serum HDL/LDL ratio, and increased serum nitric oxide levels.
What the cardiac evidence does not establish
The cardiac data is scientifically compelling but carries important limitations: the human studies involve very small numbers (7 healthy volunteers; 24 surgical patients), short measurement windows, and surrogate endpoints. All preclinical data is from rodent models. No randomised controlled trial of hexarelin for any cardiac indication has been published — the Phase 2 congestive heart failure trial data was never publicly released. Whether chronic hexarelin administration maintains meaningful CD36 engagement in humans is unknown.
Development History and Programme Discontinuation
Hexarelin was developed by Mediolanum Farmaceutici in the early 1990s in collaboration with Ezio Ghigo’s group at the University of Torino. Phase 2 trials were initiated for GHD and congestive heart failure. Neither trial reached publication, and the company discontinued the programme in 2005 for “strategic reasons.”[6]
The most likely interpretations, not mutually exclusive: the desensitisation problem rendered the GHD indication scientifically problematic (a GH secretagogue that loses 50–75% of its activity within weeks is ill-suited for chronic GHD replacement); the cardiac indication may not have achieved primary endpoints; the competitive landscape shifted; or commercial licensing negotiations did not materialise. The absence of published Phase 2 data is a significant limitation — the scientific community has never been able to evaluate the trial results.
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) | ❌ Not approved; not on 503A or 503B compounding bulks lists |
| EMA (Europe) | ❌ Not approved; never registered |
| WADA | ❌ Prohibited at all times — S2 (Peptide Hormones, Growth Factors) |
| Research chemical market | Available; for in vitro and preclinical research only |
Comparative Pharmacology: Hexarelin vs. the GHRP Class
| Feature | Hexarelin | GHRP-2 | GHRP-6 | Ipamorelin |
|---|---|---|---|---|
| GH release potency | Highest | High | Moderate | Moderate |
| GHS-R1a binding affinity | Highest | High | Moderate | Selective |
| Cortisol/ACTH elevation | Yes (dose-dependent) | Yes (dose-dependent) | Yes | ✅ Essentially none |
| Prolactin elevation | Yes | Yes | Yes | Minimal |
| Desensitisation rate | ⚠️ Fastest (50–75% in weeks) | Moderate | Moderate | Slowest |
| CD36 cardiac activity | ✅ Yes — confirmed | Limited (less studied) | Yes (independently studied) | Not characterised |
| Human clinical data | Phase 2 (unpublished) | Phase 3 (Japan, diagnostic approved) | Extensive endocrine studies | Limited |
| FDA/regulatory approval | ❌ None | Japan (diagnostic) | ❌ None | ❌ None |
Safety
Published Phase 1 and Phase 2A-level data describes a well-tolerated compound at studied doses: no serious adverse events in published trials; principal hormonal side effects are cortisol/ACTH/prolactin elevation; transient facial flushing post-injection; mild appetite stimulation; no glucose perturbation; no LH/FSH/TSH effects.[1][2]
Two specific concerns merit attention. HPA axis activation: chronic cortisol elevation, even modest, has physiological consequences including immune modulation and potential impairment of muscle protein synthesis that partially offsets GH anabolic effects. The unpublished Phase 2 safety profile: the safety signals encountered in a larger, longer-duration human population are not publicly available — for a compound that reached Phase 2 in two indications, this is an unusual and significant information gap.
⚠️ Desensitisation and user awareness: users in community settings who apply continuous dosing protocols are likely experiencing substantially attenuated GH responses within the first few weeks, without knowing it. The GH axis is being meaningfully modified during active use; a washout period is required to restore responsiveness.[3]
Common Misconceptions
“Hexarelin is the best GHRP because it’s the most potent.”
Potency in terms of peak GH pulse is only one parameter. Hexarelin’s desensitisation rate means its absolute GH advantage over other GHRPs diminishes rapidly with continued use. For extended protocols, ipamorelin’s sustained response at week 8 may represent more total GH secretion than hexarelin’s declining response over the same period. Potency per dose is not the same as cumulative effectiveness.
“The cardioprotective effects mean hexarelin is good for the heart.”
The preclinical and limited human data is intriguing and scientifically credible. But the cardiac effects were studied as acute interventions or in disease models, not as chronic preventive supplementation in healthy people. Whether routine self-administration of hexarelin by healthy individuals produces meaningful cardiac benefit has not been tested.
“Because the Phase 2 trials were done, hexarelin is proven safe.”
Phase 2 trials test safety and preliminary efficacy in defined populations. The results were never published, so neither the safety findings nor the efficacy findings are in the public record. The Phase 2 data that would characterise the compound’s safety at therapeutic doses over months is simply not available.
Frequently Asked Questions
Why did Mediolanum discontinue hexarelin?
The publicly stated reason is “strategic” — not a safety finding. The most pharmacologically plausible reason is the desensitisation problem: a GH secretagogue that loses 50–75% of its activity within weeks faces fundamental problems as a chronic GHD treatment. The cardiac indication data was never disclosed.[6]
Is hexarelin orally active?
Hexarelin is a chemically stable hexapeptide that has oral activity — substantially lower than subcutaneous injection but present, reflecting its D-amino acid stability advantage over natural peptides. Intranasal administration has also been studied in paediatric growth research, where intranasal hexarelin at 20 µg/kg was shown equivalent to 1 µg/kg IV for GH release in children with familial short stature.
How does the CD36 finding change hexarelin’s research value?
Substantially. If hexarelin were simply the most potent but most desensitising GHRP, its unique value would be limited. The CD36 finding opens an independent research programme — developing selective CD36 agonists without GHS-R1a activity, or using hexarelin as a tool compound to study CD36-mediated cardioprotection. The azapeptide analogues of hexarelin that preferentially bind CD36 over GHS-R1a represent exactly this direction.[4]
Key Takeaways
- Hexarelin is the most potent GH-releasing peptide characterised in humans — exceeding GHRP-2, GHRP-6, and ipamorelin on a per-dose basis. This potency derives from the D-2-methyltryptophan substitution that increases GHS-R1a binding affinity and protease resistance.[1]
- ⚠️ The desensitisation problem is real and rapid. A 50–75% reduction in GH response occurs within weeks of continuous administration in humans. This reversible but substantial tachyphylaxis is hexarelin’s defining pharmacological limitation and likely explains why its clinical development was discontinued.[3]
- The CD36 cardiac receptor is a genuine and rigorous scientific finding — formally characterised by Ong et al. in a Circulation Research paper (2003) using photoaffinity labelling, protein sequencing, and knockout mouse validation. It is the only confirmed second receptor for any GHRP. The cardiac effects are GH-independent and confirmed in humans.[4]
- ⚠️ The Phase 2 data is unpublished and unavailable. Two Phase 2 trials were completed but the results were never disclosed. This represents a significant information gap about the compound’s clinical efficacy and full safety profile at therapeutic doses.[6]
- Compared with ipamorelin, hexarelin offers greater peak GH output but faster desensitisation and adds cortisol/ACTH stimulation that ipamorelin avoids. For chronic repeat-dose protocols, ipamorelin is pharmacologically better suited; for short-term maximum GH stimulation or cardiac research applications, hexarelin offers unique properties.
- ⚠️ Hexarelin has no approved indication anywhere, is not legally compoundable in the US, and is prohibited by WADA. Its community use in the peptide wellness market significantly outpaces its clinical evidence base.
References
Pharmacodynamics and Human GH Studies
- Imbimbo BP, Mant T, Edwards M, Amin D, Dalton N, Boutignon F, et al. Growth hormone-releasing activity of hexarelin in humans. A dose-response study. European Journal of Clinical Pharmacology. 1994;46(5):421–425.
- Arvat E, Di Vito L, Maccagno B, Broglio F, Boghen MF, Deghenghi R, et al. Effects of GHRP-2 and hexarelin, two synthetic GH-releasing peptides, on GH, prolactin, ACTH and cortisol levels in man. Peptides. 1997;18(6):885–891.
- Rahim A, O’Neill PA, Shalet SM. Growth hormone status during long-term hexarelin therapy. Journal of Clinical Endocrinology and Metabolism. 1998;83(5):1644–1649.
CD36 Cardiac Receptor Identification
- Ong H, McNicoll N, Escher E, Collu R, Deghenghi R, Locatelli V, et al. CD36 mediates the cardiovascular action of growth hormone-releasing peptides in the heart. Circulation Research. 2003. doi: 10.1161/01.res.0000016164.02525.b4
Human Cardiac Studies
- Bisi G, Podio V, Valetto MR, Broglio F, Bertuccio G, Del Rio G, et al. Acute cardiovascular and hormonal effects of GH and hexarelin, a synthetic GH-releasing peptide, in humans. Journal of Endocrinological Investigation. 1999;22(4):266–272. PMID: 10342360
Development History
- Suckling K. Discontinued drugs in 2005: cardiovascular drugs. Expert Opinion on Investigational Drugs. 2006;15(11):1299–1308.
- Ishida J, Saitoh M, Ebner N, et al. Growth hormone secretagogues: history, mechanism of action, and clinical development. JCSM Rapid Communications. 2020;3(1):25–37. doi: 10.1002/rco2.9
Animal Cardiac Studies
- McDonald H, Peart J, Kurniawan ND, et al. Hexarelin targets neuroinflammatory pathways to preserve cardiac morphology and function in a mouse model of myocardial ischaemia-reperfusion. Biomedicine & Pharmacotherapy. 2020;127:110165.
- Locatelli V, Rossoni G, Schweiger F, et al. Growth hormone-independent cardioprotective effects of hexarelin in the rat. Endocrinology. 1999;140(9):4024–4031.
Key Investigators
- Ezio Ghigo, MD — University of Torino; principal investigator on the Italian-Swiss hexarelin human pharmacodynamic studies (1994–2000).
- Huy Ong, PhD — Université de Montréal; lead investigator on the CD36 identification work (2003); established the molecular basis for hexarelin’s GH-independent cardiac effects.
- Romano Deghenghi, PhD — Europeptides, Argenteuil, France; co-developer of hexarelin alongside Mediolanum Farmaceutici.
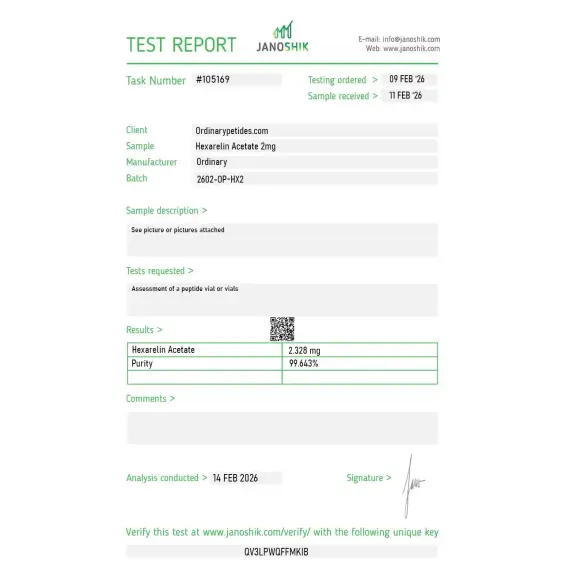
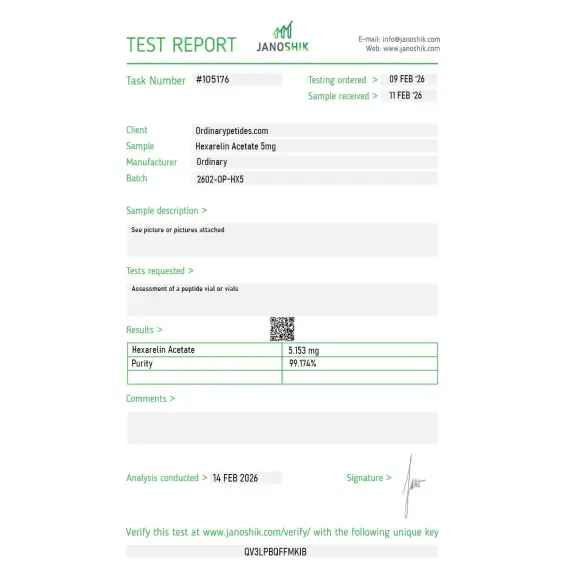
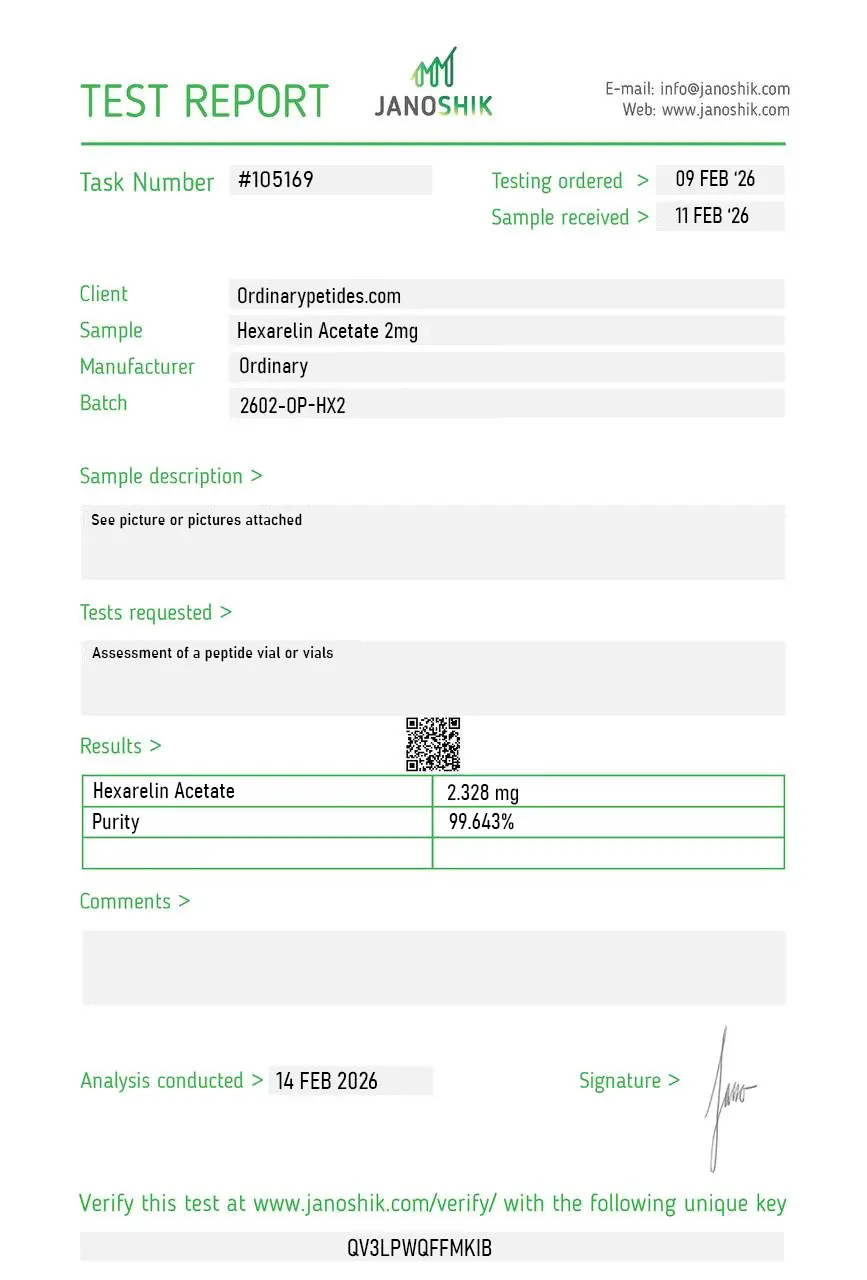
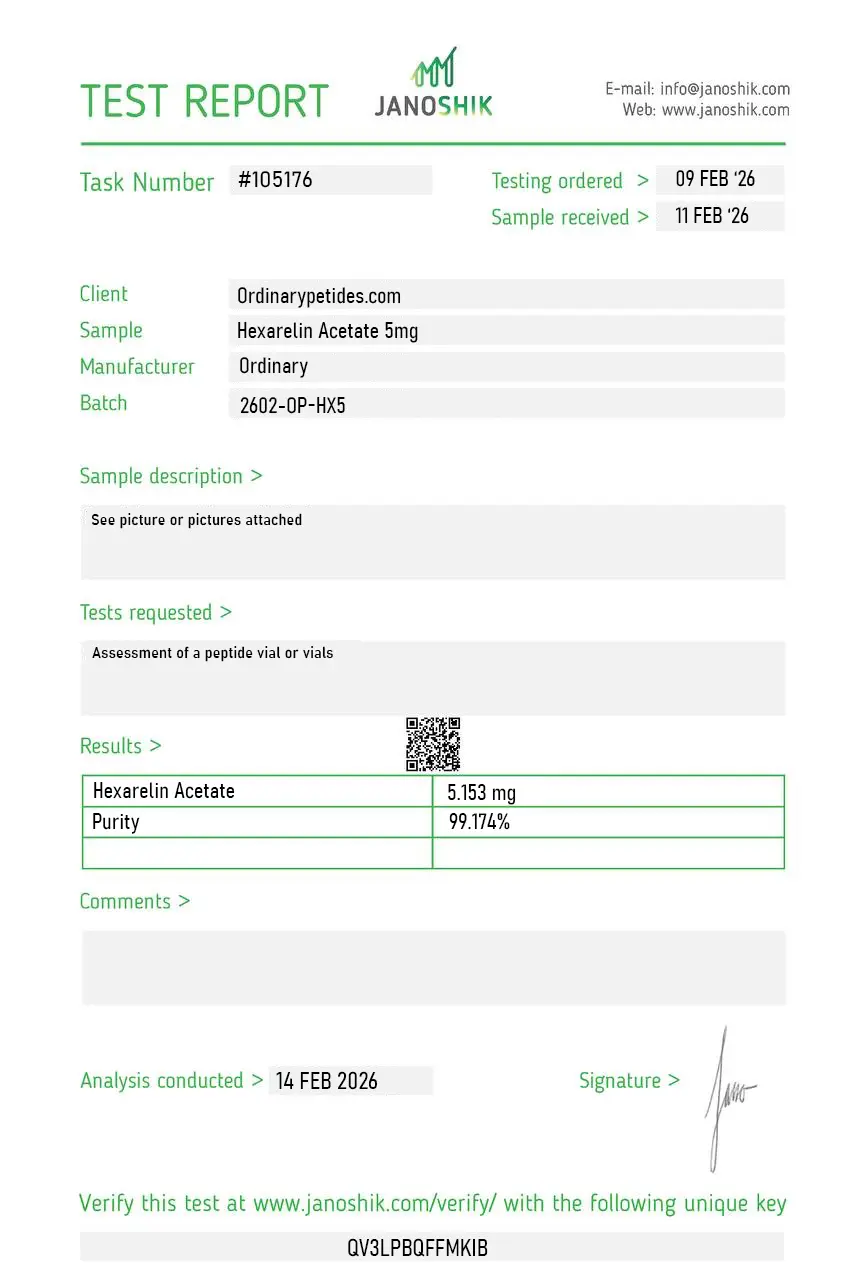
Certificate of Analysis
Independent test reports are available for Hexarelin Acetate 2mg and 5mg batches. These reports provide batch-level documentation and analytical verification information for research reference.
For a peptide where the salt form matters experimentally, the certificate should confirm the counterion exchange was complete — residual TFA below a specified threshold, ideally with an ion-chromatography or 19F-NMR figure showing the TFA-to-acetate conversion. The compound performed without obvious TFA artifacts in our culture work, but the salt-form purity is the specific verification that distinguishes a properly acetate-exchanged preparation from a nominally-acetate one. That data should be on the certificate.
The acetate salt is the standard pharmaceutical form for cationic peptides like Hexarelin, and worth ordering specifically — TFA-counterion preparations leftover from solid-phase synthesis can interfere with cell-culture assays at low concentrations because residual TFA has its own cellular effects. Acetate-exchanged material removes that confound. The listing specified acetate cleanly, and the compound behaved without the TFA-related background we've seen from other sources.
Usually, yes. Hexarelin acetate is simply the acetate salt form of Hexarelin, so the active peptide being discussed is essentially the same.
No. Hexarelin is not growth hormone itself. It is a growth hormone secretagogue, meaning it stimulates the body to release growth hormone.
Yes. One of the most consistently reported findings about Hexarelin is that it can increase growth hormone levels in humans.
No. Studies suggest that Hexarelin may also increase prolactin (PRL), ACTH, and cortisol, so its effects are broader than GH alone.
There are some interesting early findings, including limited human data, but that is not enough to call it a proven cardiovascular therapy.
No convincing clinical evidence supports Hexarelin as an established anti-aging treatment.
Yes. As a growth hormone secretagogue, Hexarelin falls into a prohibited anti-doping category.
Hexarelin Acetate (also known as examorelin, INN) is a synthetic hexapeptide — six amino acids — with the sequence His-D-2-methyl-Trp-Ala-Trp-D-Phe-Lys-NH₂. It was developed in the mid-1980s by Dr. Cyril Bowers and colleagues at Tulane Medical School as part of the same research program that produced GHRP-2 and GHRP-6. Structurally it is a 2-methyl-D-tryptophan derivative of GHRP-6, a modification that makes it chemically more stable and functionally more potent than its predecessors. It is the most potent GH-releasing peptide in the GHRP class — stimulating larger GH pulses than GHRP-2, GHRP-6, or Ipamorelin at equivalent doses. It is unique among GHRPs in having a clearly documented second receptor — the scavenger receptor CD36 — through which it exerts direct cardiovascular effects entirely independent of GH release. It is not FDA-approved for any therapeutic indication and is available only as a research compound.
Like all GHRPs, hexarelin activates GHS-R1a (the ghrelin receptor) in the anterior pituitary and hypothalamus, triggering calcium influx, inhibiting somatostatin, and producing a potent pulsatile GH surge. Compared to GHRP-2 and Ipamorelin, hexarelin's GHS-R1a activation is more potent and produces larger GH pulses — but this also comes with more pronounced off-target hormonal effects including cortisol, prolactin, and ACTH elevation comparable to GHRP-6. Its defining pharmacological distinction is the CD36 receptor. CD36 is a scavenger receptor expressed on cardiac muscle cells, endothelial cells, monocytes, and adipose tissue. Hexarelin binds CD36 directly and through this non-GHS-R1a pathway exerts cardioprotective effects — improving left ventricular function, reducing ischemia-reperfusion injury, reducing cardiac fibrosis and inflammation, and increasing coronary perfusion pressure — all in a GH-independent manner. No other GHRP in this series has this dual-receptor cardiovascular mechanism documented to the same degree.
Hexarelin has more published human data than most research peptides in this series. A study in seven healthy male volunteers demonstrated that hexarelin administration significantly increased left ventricular ejection fraction (LVEF) from 64% to 70.7% within 15 to 30 minutes, with the effect lasting up to 60 minutes, without changing blood pressure or heart rate. In 24 male patients with coronary artery disease undergoing bypass surgery, IV hexarelin at 2 mcg/kg produced rapid increases in LVEF, cardiac output, and cardiac index while reducing wedge pressure — suggesting improved cardiac contractility and reduced preload. A dose-finding study in 12 healthy male volunteers confirmed GH-releasing activity with an ascending IV dose protocol that was well tolerated. Human studies also documented its effect on ACTH and cortisol, showing that the ACTH response to hexarelin varies with age — present in prepubertal children, increasing at puberty, declining in adulthood, and rising again in aging.
Hexarelin is the most potent GH stimulator in the GHRP class but carries the broadest non-GH hormonal profile. Compared to Ipamorelin — which is highly selective for GH with negligible cortisol, prolactin, or ACTH effects — hexarelin stimulates cortisol and prolactin at comparable or slightly higher levels than GHRP-2, making it less favorable for long-term continuous use without cycling. Its main advantages over GHRP-2 and GHRP-6 are greater GH potency, greater chemical stability, longer duration of GH elevation per dose, and the unique CD36-mediated cardiovascular effects. Its main disadvantage relative to Ipamorelin is the less selective hormonal profile. It does not significantly stimulate appetite — unlike GHRP-6 — which is a practical advantage for body composition protocols.
Hexarelin is given by subcutaneous injection. Research studies have also used IV administration. Typical wellness protocols use 100 to 200 mcg per injection, one to two times daily. Like all GHRPs it should be injected on an empty stomach for maximal GH response. GH concentrations peak approximately 30 to 45 minutes after injection. Receptor desensitization is a documented concern with hexarelin — more so than with Ipamorelin — particularly with continuous daily dosing, requiring cycling protocols typically of 12 to 16 weeks on followed by 4-week breaks. Combining hexarelin with a GHRH analog like CJC-1295 No DAC produces synergistic GH pulses through dual-pathway activation. Higher doses do not proportionally increase GH release — a plateau effect is observed — suggesting there is a ceiling beyond which additional dose provides diminishing returns.
The most commonly reported effects are fluid retention, injection site reactions, increased appetite at higher doses though less pronounced than GHRP-6, fatigue, headache, and tingling or numbness in the extremities. Cortisol elevation is a relevant concern — chronic cortisol elevation can impair sleep, promote fat accumulation, suppress immunity, and affect mood. Prolactin elevation can cause gynecomastia in men at sustained higher doses. Receptor desensitization with continuous use is well-documented and requires cycling to preserve efficacy. It does not suppress endogenous testosterone, is not androgenic, does not cause androgenic side effects such as hair loss or acne, and does not negatively affect cholesterol or blood pressure based on available data.
People with active cancer or cancer history should not use it given IGF-1 elevation's role in cell growth promotion. Those with Cushing's disease or elevated cortisol should not use it as it exaggerates ACTH and cortisol responses — documented specifically in Cushing's disease where hexarelin produces exaggerated ACTH responses compared to CRH. People with diabetes or insulin resistance should be cautious given GH's anti-insulin effects. Pregnant or breastfeeding women should not use it. Children should not use it given the age-dependent endocrine responses documented. Competitive athletes are prohibited from use under WADA. It cannot be legally compounded in the United States.





