




GHRP-2
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
GHRP-2 (Pralmorelin): A Real Pharmacological Tool With a Clearly Visible Effect in the Endocrinological Context
GHRP-2, also known as pralmorelin, is not growth hormone itself, but a peptide from the ghrelin-pathway class that, in the research context, has been shown to rapidly and markedly stimulate the release of endogenous GH.
In published human observations, it did not act only through the GH response, but also through its influence on appetite, as well as on other hormonal axes, which makes it a molecule with a much broader neuroendocrine logic than its name might suggest.
In early and clinical studies, it was valued especially as a powerful secretagogue and diagnostic tool, and in Japan, pralmorelin even received diagnostic use for the assessment of GH secretion.
One important honest point: a vivid acute hormonal signal is not yet automatically the same thing as proven long-term benefit for growth, body composition, or "anti-aging." Science can be impressive without becoming magic, which is probably for the best. That is exactly why GHRP-2 is interesting not as yet another loud peptide legend, but as a real pharmacological tool with a clearly visible effect in the endocrinological context.
Practical Takeaway
If you are interested in peptides that actually do something at the level of the research model, rather than merely sounding impressive, GHRP-2 definitely deserves attention.
GHRP-2 (Pralmorelin): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
GHRP-2 occupies a distinctive position in the growth hormone secretagogue landscape: it is the most potent of the classical hexapeptide GHRPs by peak GH output, the first GHRP to reach clinical approval anywhere in the world, and a compound with more genuine human pharmacodynamic data than most research peptides in active use today.
The key facts: It works, reliably and powerfully. GHRP-2 causes robust GH release through the ghrelin receptor (GHS-R1a), independently replicated across decades of clinical pharmacology studies in healthy adults, elderly subjects, GH-deficient patients, and critically ill patients.[6][7] It is not selective — unlike ipamorelin, GHRP-2 also stimulates ACTH, cortisol, and prolactin in a dose-dependent fashion. It failed as a treatment — despite years of development, intranasal GHRP-2 failed to produce clinically significant height velocity improvements in children and the therapeutic programme was discontinued. The Japan approval is narrow: diagnostic use only, single dose, IV, in a medical setting.
| At a glance | |
|---|---|
| INN (pharmaceutical name) | Pralmorelin |
| Former codes | KP-102, GPA-748, WAY-GPA-748 |
| Brand name (Japan) | GHRP Kaken 100 |
| Sequence | D-Ala-D-(β-naphthyl)-Ala-Trp-D-Phe-Lys-NH&sub2; |
| Type | Synthetic hexapeptide; second-generation GHRP |
| Molecular weight | 817.97 Da |
| Primary mechanism | GHS-R1a (ghrelin receptor) agonist |
| Off-target effects | ACTH, cortisol, and prolactin stimulation; orexigenic |
| Developer | Cyril Y. Bowers (Tulane University); Kaken Pharmaceutical (Japan) |
| Japan approval | October 2004 (PMDA) — diagnostic agent for GHD assessment only |
| US status | ❌ Not approved; no 503A or 503B compounding |
| WADA status | ❌ Prohibited at all times (S2 — Growth Hormone Secretagogues) |
Historical Development: From Morphine Analogues to Ghrelin Receptor
The development of GHRP-2 traces directly to work by Cyril Y. Bowers and colleagues at Tulane University beginning in the mid-1970s. The programme emerged from an unexpected observation: certain synthetic analogues of met-enkephalin stimulated GH secretion from rat pituitary cells without producing analgesia. This initial finding launched a systematic medicinal chemistry programme. GHRP-6 emerged from this work in the early 1980s as the first well-characterised member. GHRP-2 was developed subsequently as a “second-generation” compound — a hexapeptide with modifications designed to increase GH-stimulating potency.[1]
For nearly two decades, GHRPs were described as a pharmacological curiosity: peptides that powerfully stimulated GH through an unknown receptor by an unknown mechanism. The resolution came in 1996 when Howard et al. cloned the growth hormone secretagogue receptor type 1a (GHS-R1a).[2] Then in 1999, Kojima et al. isolated the endogenous ligand for this receptor from rat stomach: ghrelin.[3] The discovery revealed that Bowers had independently mapped a complete endogenous regulatory system through a purely synthetic chemistry approach years before the natural ligand was identified. GHRP-2’s receptor and mechanism are therefore not idiosyncratic — they are the same receptor and mechanism used by ghrelin, one of the most thoroughly studied endocrine axes in modern biology.
Chemistry and Structure
GHRP-2’s sequence is: D-Ala – D-(β-Naphthyl)-Ala – Trp – D-Phe – Lys – NH&sub2;. Several features distinguish it from natural peptides: D-amino acids at positions 1, 2, and 4 confer protease resistance and increase receptor binding affinity. The β-naphthyl-alanine at position 2 increases lipophilicity and receptor affinity relative to the tryptophan used in earlier analogues. C-terminal amidation (–NH&sub2;) protects the C-terminus from carboxypeptidase degradation. Despite being a peptide, GHRP-2 demonstrates measurable oral activity — though oral bioavailability is substantially lower than by injection, which is why the subcutaneous or IV route remains standard.[11]
| Property | Detail |
|---|---|
| Length | 6 amino acids (hexapeptide) |
| Molecular weight | 817.97 Da |
| D-amino acid content | Positions 1, 2, 4 |
| Half-life (plasma) | ~15–30 minutes |
| Route | Subcutaneous or IV (primary); some oral activity |
| Parent compound | Met-enkephalin analogue |
| Receptor | GHS-R1a (same as ghrelin) |
Mechanism of Action
GHS-R1a: the ghrelin receptor
GHRP-2 binds with high affinity to GHS-R1a — a Gq/11-coupled G-protein receptor expressed on somatotroph cells in the anterior pituitary and in the hypothalamic arcuate and ventromedial nuclei, as well as peripheral tissues including the heart, stomach, and adipose tissue. The intracellular cascade: Gq/11 protein coupling → phospholipase C (PLC) activation → IP&sub3; + diacylglycerol → intracellular Ca²+ release → GH vesicle exocytosis. This is distinct from the GHRH receptor (Gs-coupled → cAMP → PKA pathway). The two pathways are complementary and synergistic, which is why combining GHRP-2 with GHRH analogues produces 2–3-fold greater GH release than either compound alone.[12]
Dual pituitary and hypothalamic action
GHRP-2 stimulates GH release through two anatomical sites. At the pituitary, it directly stimulates somatotroph cells. At the hypothalamus, it activates arcuate nucleus neurones that suppress somatostatin (the endogenous GH inhibitor). The hypothalamic component amplifies the pituitary effect and helps maintain pulsatility.[7]
The dose-response plateau: GH vs. ACTH
One of GHRP-2’s most clinically important pharmacodynamic characteristics is a differential dose-response. GH release exhibits dose-proportional increases up to approximately 1 µg/kg IV, at which point the GH response plateaus while ACTH, cortisol, and prolactin responses continue to increase in a dose-dependent manner. The practical implication: higher doses do not produce more GH, but do produce more cortisol, ACTH, and prolactin. Optimal dosing is at or below the GH plateau — approximately 1 µg/kg IV in clinical pharmacology studies, or ~100 µg subcutaneously in most research protocols.[5]
Orexigenic effect: the appetite drive
GHS-R1a receptors in the hypothalamic arcuate nucleus mediate hunger signalling — the same pathway through which ghrelin (the “hunger hormone”) drives appetite before meals. GHRP-2 activates this pathway, producing a clinically measurable increase in food intake in humans, as directly confirmed in a controlled human study.[4]
Clinical Evidence
GHRP-2 has one of the more substantial human evidence bases of any compound in this series — concentrated in pharmacodynamic studies and, importantly, real randomised controlled trials in ICU patients.
Pharmacodynamic studies in healthy adults
Numerous studies across the 1990s–2010s established the dose-response profile: peak plasma GH of 30–100 ng/mL approximately 15–30 minutes after subcutaneous injection; 8–20-fold increases above baseline, dose-dependent up to ~1 µg/kg IV; cortisol elevation moderate and transient within normal physiological range; prolactin elevation present but transient; ACTH stimulation dose-dependent and comparable to hCRH at studied doses.[5]
Food intake in healthy men (Laferrère et al., 2005)
Seven lean, healthy males were subcutaneously infused with GHRP-2 (1 µg/kg/h) or saline for 270 minutes, then measured intake of an ad libitum buffet-style meal. Subjects ate 35.9 ± 10.9% more when infused with GHRP-2 vs. saline, with every subject increasing their intake. GH levels were significantly more elevated during GHRP-2 infusion (AUC 5,550 ± 1,090 µg/L/240 min vs. 412 ± 161, p=0.003). Serum cortisol levels increased transiently with GHRP-2 compared to placebo.[4] This was the first controlled demonstration that GHRP-2, like ghrelin itself, increases food intake in humans.
Critical illness studies (Van den Berghe group, University of Leuven)
This is the most medically significant body of human GHRP-2 evidence. Van den Berghe and colleagues conducted an extended series of studies on GHRP-2 in critically ill adults — a population characterised by profound GH axis dysregulation: paradoxically elevated GH but reduced IGF-1, blunted pulsatility, and hypercatabolism. Key findings across this series:[6][7][8][9]
- GHRP-2 produced substantially more GH release than GHRH alone in critically ill patients; the combination produced the greatest effect
- Continuous GHRP-2 infusion (1 µg/kg/h) restored synchronised pulsatile GH release in prolonged critical illness
- The synchronising effect on GH, TSH, and prolactin was specific to GHRP-2 — not seen with GHRH or TRH alone
- Combined GHRP-2 + TRH + GnRH produced superior endocrine and metabolic effects vs. GHRP-2 alone, with improved IGF-1, restored thyroid function, and improved androgen levels
- GHRP-2-based protocols appeared safer than exogenous recombinant GH, which increases mortality in critical illness, because GHRP-2 works within the GH axis’s feedback control rather than bypassing it
These are real clinical trials — randomised, controlled, published in major endocrinology journals — not animal studies or mechanistic cell culture work. They represent some of the highest-quality human evidence available for any compound in this article series.
Japan diagnostic approval (multicenter trial, 2004)
The Japan PMDA approval was based on multicenter trials across 84 Japanese clinical facilities demonstrating that GH levels following a single 100 µg IV bolus of pralmorelin exceed 15 µg/L in healthy individuals but remain below 15 µg/L in patients with severe GH deficiency, reliably discriminating the two groups for diagnostic purposes. This is the compound’s only regulatory approval.
Intranasal short stature (Phase 2 — failed)
GHRP-2 was evaluated in Phase 2 clinical trials for growth promotion in GH-deficient children via intranasal spray. Despite increasing endogenous GH secretion, the treatment failed to translate into clinically significant height velocity improvements over 24 weeks, and the therapeutic development programme was discontinued.[10] This failure highlights a fundamental challenge with GH secretagogues: acutely stimulating GH pulse amplitude does not necessarily produce the sustained IGF-1 elevation required for meaningful growth promotion.
Human evidence summary
| Study type | Population | Route | GH outcome | Interpretation |
|---|---|---|---|---|
| Phase 2 RCT (intranasal) | Children, short stature | Intranasal | GH ↑, height velocity NS | ❌ Failed; programme discontinued |
| PD studies (healthy adults) [5] | Healthy volunteers | IV/SC | GH 8–20× baseline | ✅ Well-characterised; dose-ceiling at ~1 µg/kg |
| Food intake RCT [4] | 7 lean healthy men | SC infusion | GH ↑ 13×; food intake +36% | ✅ Orexigenic effect confirmed in humans |
| Critical illness studies [6]–[9] | ICU patients | IV infusion | GH ↑; pulsatility restored | ✅ Best clinical evidence; multiple RCTs |
| Japan diagnostic trials | Adults/children GHD | IV bolus | Reliable GHD discrimination | ✅ Basis of PMDA approval |
Regulatory Status
| Jurisdiction | Status |
|---|---|
| Japan (PMDA) | ✅ Approved — October 2004; Kaken Pharmaceutical; single-dose 100 µg IV diagnostic agent for GHD assessment only |
| USA (FDA) | ❌ Not approved; Wyeth sublicence from Kaken never completed FDA process; warning letters issued to pharmacies marketing for human use; not on 503A or 503B bulks lists |
| Europe (EMA) | ❌ Not approved |
| WADA | ❌ Prohibited at all times — S2 (Peptide Hormones, Growth Factors, Growth Hormone Secretagogues and Related Substances) |
Comparison with Other GH Secretagogues
| Compound | Class | Receptor | GH potency | ACTH/Cortisol | Prolactin | Appetite | Status |
|---|---|---|---|---|---|---|---|
| GHRP-2 | Hexapeptide GHRP | GHS-R1a | ★★★★★ | ★★★ | ★★★ | ★★ | Japan only (diagnostic) |
| GHRP-6 | Hexapeptide GHRP | GHS-R1a | ★★★★ | ★★★ | ★★★ | ★★★★ | Research only |
| Ipamorelin | Pentapeptide GHRP | GHS-R1a | ★★★ | None | None | ★ | Category 2 |
| Hexarelin | Hexapeptide GHRP | GHS-R1a | ★★★★★ | ★★★★ | ★★★★ | ★★★ | Research only |
| MK-677 | Non-peptide GHS | GHS-R1a | ★★★★ | ★★ | ★★ | ★★★ | Phase 3 (cachexia); not approved |
| Sermorelin | GHRH analogue | GHRH-R | ★★ | None | None | None | Discontinued (FDA 2008); 503B |
| Tesamorelin | GHRH analogue | GHRH-R | ★★★ | None | None | None | ✅ FDA-approved (HIV lipodystrophy) |
Safety Profile
Well-characterised acute effects (within physiological range at standard doses)
Cortisol elevation: Moderate, transient, returns to baseline within hours. Comparable to hCRH stimulation. At standard doses, remains within the normal physiological range — not associated with clinical hypercortisolaemia.[5] Prolactin elevation: Present but lower than TRH-induced; transient. Appetite increase: Clinically significant (+35% food intake in the controlled human study).[4] Relevant for any protocol where caloric intake needs controlling. Water retention: Reported anecdotally; plausible via GH-mediated fluid retention but not systematically characterised. Flushing/injection site reactions: Common, transient.
Important nuances
Visceral fat attenuates response: Abdominal visceral fat is a dominant negative predictor of both GHRH and GHRP-2 effectiveness. Individuals with higher visceral adiposity show blunted GH responses — an important finding for the wellness population most likely to seek GH axis optimisation. Somatostatin feedback intact: Unlike exogenous rhGH (which bypasses all feedback), GHRP-2 stimulates GH within the intact hypothalamic-pituitary feedback system. This limits the magnitude of GH release and may prevent the supraphysiological exposures associated with rhGH’s known mortality increase in critical illness. Desensitisation with chronic dosing: Some evidence suggests attenuation of the ACTH/cortisol response with longer-duration treatment while GH responses are better maintained — consistent with the critical illness literature.[8]
Long-term safety
No long-term safety data from controlled trials of therapeutic GHRP-2 administration exists. The compound never completed the clinical development process required to generate such data. The critical illness studies (7–21-day infusions in ICU patients) represent the longest controlled human exposures in the published literature. The theoretical risks associated with chronic GH axis elevation — insulin resistance, fluid retention, increased cancer risk in susceptible individuals — apply to GHRP-2 as to all GH secretagogues, though the magnitude of IGF-1 elevation achievable through endogenous stimulation is generally lower than with exogenous rhGH.
Common Misconceptions
“GHRP-2 is FDA-approved.”
It is approved in Japan only, as a single-dose diagnostic agent. Not FDA-approved, not approved in Europe, and not legally compoundable in the US.
“Because the Japan approval exists, we know it’s safe for chronic therapeutic use.”
⚠️ The Japan approval covers a single 100 µg IV bolus administered in a clinical setting to test pituitary function. This is categorically different from repeated subcutaneous self-injection for weeks or months. Diagnostic single-dose approval does not confer safety data for chronic therapeutic protocols.
“GHRP-2 works better than ipamorelin.”
GHRP-2 produces greater peak GH output than ipamorelin at matched doses. Whether “better” is accurate depends entirely on the goal: if maximising GH pulse amplitude is the priority, GHRP-2 is more potent. If avoiding cortisol, ACTH, and prolactin stimulation is a priority — as it typically is in repeated-dosing wellness protocols — ipamorelin’s selective profile is superior.
“The critical illness studies prove it works for anti-ageing and muscle building.”
The Van den Berghe studies demonstrated that GHRP-2 restores GH pulsatility in critically ill patients with blunted GH secretion.[7] Critically ill patients have different physiology from healthy adults seeking body recomposition. These findings establish mechanism and safety in a specific clinical context; they do not validate the compound for its most common off-label uses.
“Combining GHRP-2 with CJC-1295 is synergistic.”
The synergy of combining a GHS-R1a agonist (GHRP-2) with a GHRH-R agonist (CJC-1295) is pharmacologically real — the two receptors operate through complementary pathways and combining them produces substantially greater GH release than either alone. This is well-supported in the research literature. What is not established is whether this synergistic GH release translates into clinically meaningful long-term benefits for healthy adults.
Frequently Asked Questions
Why didn’t GHRP-2 receive FDA approval when it works so well at stimulating GH?
Regulatory approval requires demonstration of clinical benefit (not just pharmacodynamic activity) plus safety in the target population for the specific indication. GHRP-2 stimulates GH reliably, but Phase 2 data failed to show meaningful height velocity improvement in children — the intended therapeutic population.[10] For adult indications (anti-ageing, body recomposition), no adequately powered trials with validated clinical endpoints were conducted. Diagnostic approval in Japan requires much simpler evidence than therapeutic approval.
Is the Japan diagnostic use relevant to bodybuilding/anti-ageing protocols?
No. The Japan approval covers 100 µg IV, administered once, to distinguish GH-deficient patients from healthy controls. Repeated subcutaneous injection to maintain chronically elevated GH/IGF-1 is an entirely different use case with no regulatory basis in any country.
How does GHRP-2 compare to direct GH injection?
GHRP-2 stimulates the pituitary to release its own GH — maintaining normal feedback loop function and pulsatility. Exogenous rhGH bypasses this, directly raising GH regardless of endogenous signals. Consequences: rhGH suppresses endogenous GH secretion; GHRP-2 does not. rhGH can produce supraphysiological GH levels and was associated with increased ICU mortality; GHRP-2 is constrained by feedback. The physiological constraint built into secretagogue use may reduce some risks of the exogenous approach.
Can GHRP-2 be legally prescribed in the US?
Not through standard compounding channels — it is not on the 503A or 503B bulks lists. Its regulatory status in the US is as an unapproved drug for human use. FDA warning letters have been issued to pharmacies marketing it for therapeutic purposes.
Key Takeaways
- GHRP-2 has the most well-characterised human pharmacodynamic profile of any GHRP in this series. Decades of clinical pharmacology studies across multiple populations, including real randomised controlled trials in ICU patients, provide a genuine evidence base that most research peptides lack.[6]–[9]
- Its GH-stimulating potency is real and substantial — peak increases of 8–20-fold over baseline are reproducible and independently documented. The synergy with GHRH-class compounds is pharmacologically genuine.
- ⚠️ The off-target ACTH/cortisol/prolactin activation is meaningful. It is moderate and transient at standard doses, but it distinguishes GHRP-2 from ipamorelin and makes it less suitable for repeated-dosing protocols where hormonal selectivity is prioritised.
- ⚠️ The Japan approval is narrow and not generalisable to the therapeutic uses for which GHRP-2 is most commonly sought. Diagnostic single-dose IV use bears no relationship to chronic subcutaneous therapeutic administration.
- The failed short stature programme demonstrates that GH stimulation on its own does not guarantee clinically meaningful outcomes — the gap between pharmacodynamic activity and therapeutic efficacy is a recurring theme across the GH secretagogue class.
- The critical illness research is the most clinically significant human evidence. It reveals GHRP-2’s mechanistic importance in normal GH axis orchestration and suggests a genuinely promising research direction — but one distinct from its predominant off-label use in wellness contexts.
References
Development History
- Bowers CY, et al. Derivative forms of met-enkephaline selectively promote GH secretion. Studies from 1976–1980. Tulane University.
- Howard AD, Feighner SD, Cully DF, et al. A receptor in pituitary and hypothalamus that functions in growth hormone release. Science. 1996;273:974.
- Kojima M, Hosoda H, Date Y, et al. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature. 1999;402:656–660.
Human Pharmacodynamic Studies
- Laferrère B, Abraham C, Russell CD, Bowers CY. Growth hormone releasing peptide-2 (GHRP-2), like ghrelin, increases food intake in healthy men. Journal of Clinical Endocrinology and Metabolism. 2005. PMC2824650
- Arvat E, Di Vito L, Maccagno B, et al. Effects of GHRP-2 and hexarelin, two synthetic GH-releasing peptides, on GH, prolactin, ACTH and cortisol levels in man. Journal of Endocrinological Investigation. 1997.
Critical Illness Studies (Van den Berghe series)
- Van den Berghe G, de Zegher F, Bowers CY, et al. Pituitary responsiveness to GH-releasing hormone, GH-releasing peptide-2 and thyrotrophin-releasing hormone in critical illness. Clinical Endocrinology. 1996;45(3):341–351. PMID: 8949573
- Van den Berghe G, de Zegher F, Veldhuis JD, et al. The somatotropic axis in critical illness: effect of continuous GHRH and GHRP-2 infusion. Journal of Clinical Endocrinology and Metabolism. 1997;82:590–599.
- Van den Berghe G, Wouters P, Bowers CY, et al. Growth hormone-releasing peptide-2 infusion synchronizes growth hormone, thyrotrophin and prolactin release in prolonged critical illness. European Journal of Endocrinology. 1999. PMID: 10037246
- Van den Berghe G, Baxter RC, Weekers F, et al. The combined administration of GH-releasing peptide-2 (GHRP-2), TRH and GnRH to men with prolonged critical illness evokes superior endocrine and metabolic effects compared to treatment with GHRP-2 alone. Clinical Endocrinology. 2002;56(5):655–669. PMID: 12030918
Regulatory and Reviews
- Pralmorelin. Wikipedia. en.wikipedia.org/wiki/Pralmorelin
- Furuta S, et al. General pharmacology of KP-102 (GHRP-2), a potent growth hormone-releasing peptide. Arzneimittelforschung. 2004;54(12):868–880. PMID: 15646371
- Ishida J, et al. Growth hormone secretagogues: history, mechanism of action, and clinical development. JCSM Rapid Communications. 2020. doi: 10.1002/rco2.9
Key Investigators
- Cyril Y. Bowers, MD, PhD — Professor of Medicine, Tulane University; discoverer of GHRP-6 and principal developer of the GHRP class including GHRP-2; received Monsanto Clinical Investigator Award from Endocrine Society (1998).
- Greet Van den Berghe, MD, PhD — University of Leuven, Belgium; led the critical illness GHRP-2 research programme; foremost investigator of GH secretagogues in intensive care medicine.
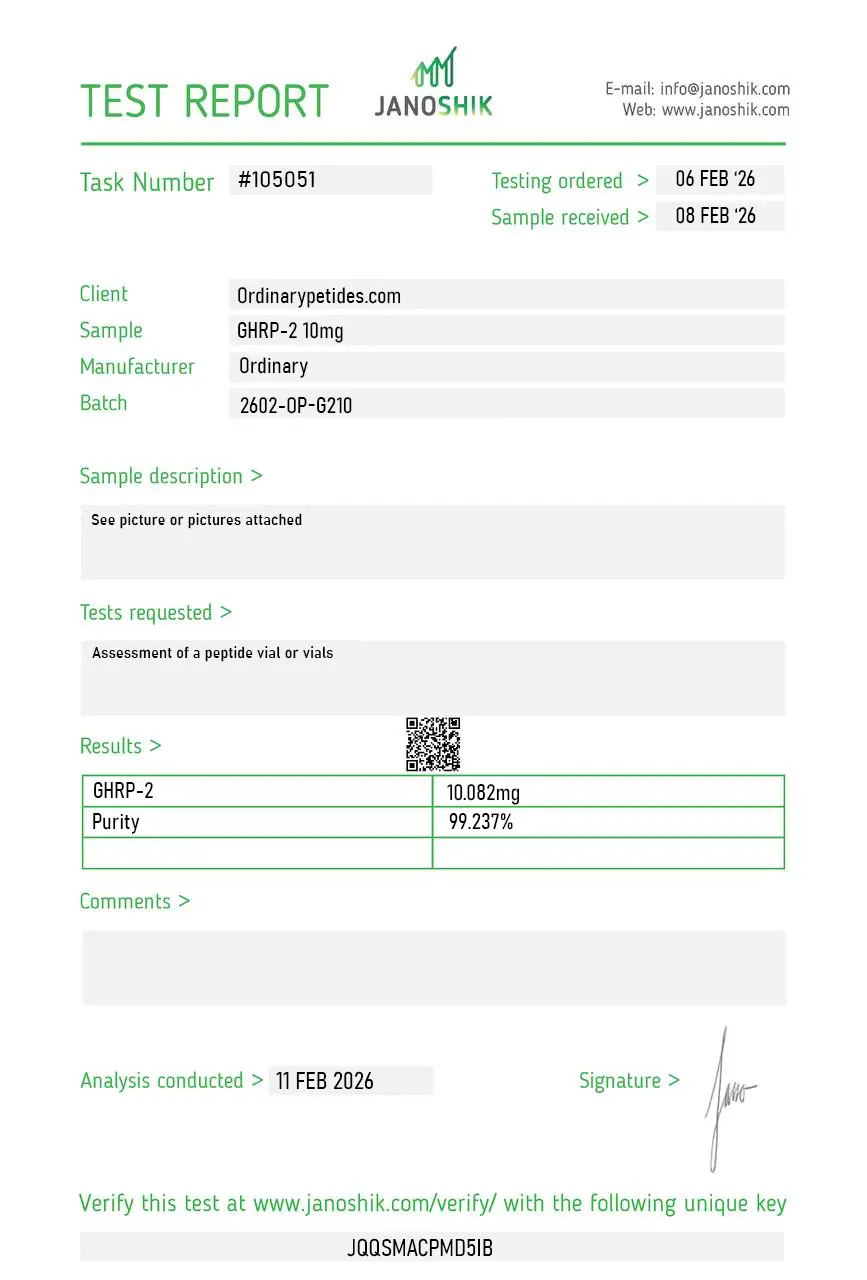
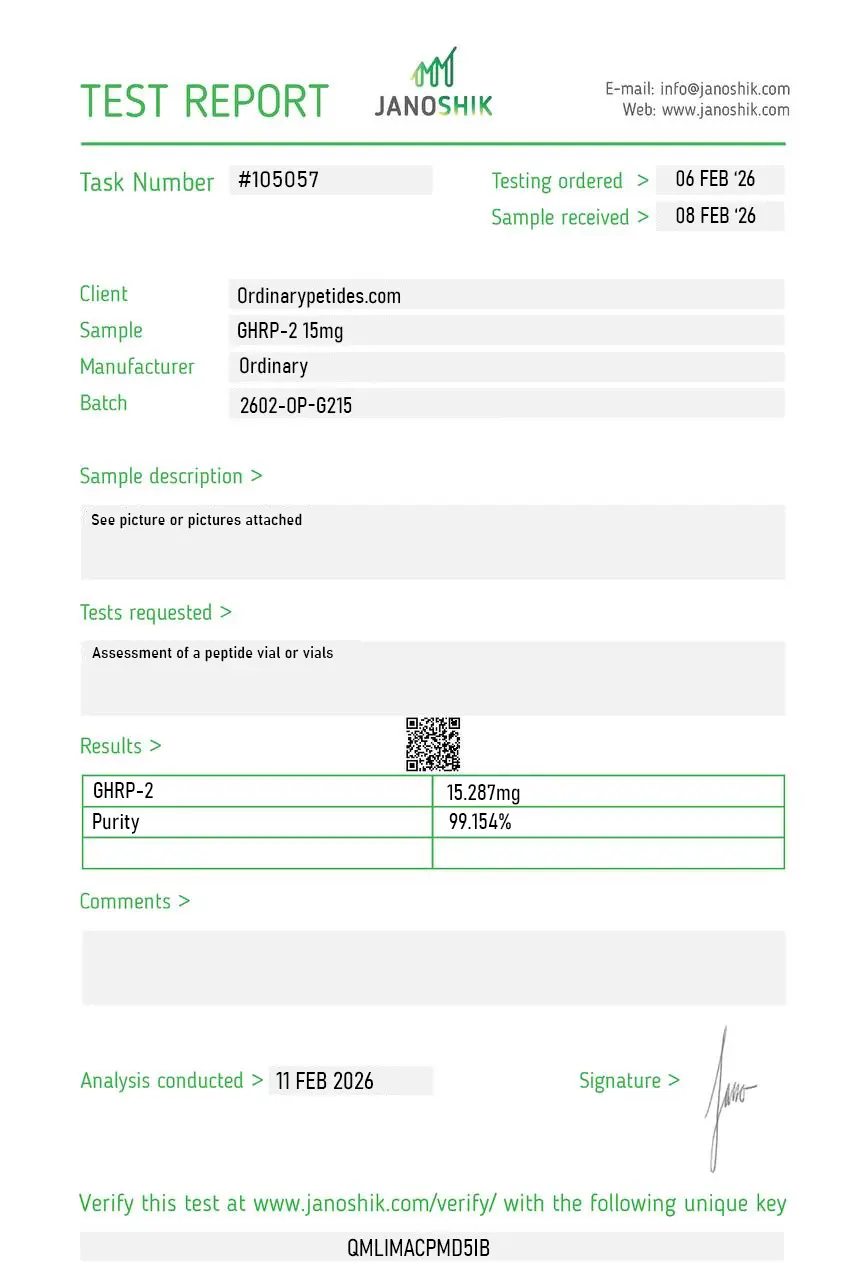
Certificate of Analysis
Independent test reports are available for GHRP-2 5mg, 10mg, and 15mg batches. These reports provide batch-level documentation and analytical verification information for research reference.
Based on 2 reviews
5.0
We use it as the diagnostic-test reference — pralmorelin had a defined role as a GH-stimulation provocative agent in Japanese clinical endocrinology, and that history gives it a characterized response curve we can anchor in-vitro work against. Most secretagogues lack that kind of validated provocative-test pedigree. The material gave a reproducible somatotroph response consistent with that reference profile.
What earned the order is that the listing references the Bowers-era GHRP pharmacology and the pralmorelin diagnostic lineage rather than the secretagogue marketing — for someone doing GH-stimulation-mechanism work, that academic framing is what signals the vendor understands the compound. For receptor-pathway work anchored to the provocative-test literature, that precision was the deciding factor. Consistent across two orders.
GHRP-2 (Growth Hormone Releasing Peptide-2), also known by its INN pralmorelin and its developmental code KP-102, is a synthetic hexapeptide — six amino acids — with the sequence D-Ala-D-(β-naphthyl)-Ala-Trp-D-Phe-Lys-NH₂. It is a non-natural super-analog of the earlier GHRP-6 and belongs to the first generation of GH secretagogues developed from the 1980s onward. It is the first ghrelin receptor agonist class drug to reach clinical introduction — it is approved in Japan by Kaken Pharmaceutical under the brand name GHRP Kaken 100 as a single-dose diagnostic agent for assessing growth hormone deficiency (GHD). Outside Japan it is not approved for therapeutic use and exists as a research compound. Unlike CJC-1295 and Ipamorelin which act on GHRH receptors, GHRP-2 acts on a completely different receptor — the ghrelin receptor (GHS-R1a) — and is structurally derived from met-enkephalin rather than GHRH.
Because GHRP-2 activates ghrelin receptors involved in appetite signaling, increased hunger has been observed in experimental settings.
It binds to growth hormone secretagogue receptors (GHS-R1a) in the hypothalamus and pituitary, triggering pulsatile growth hormone secretion.
In research models, GHRP-2 is associated with increased GH release, possible IGF-1 elevation, appetite stimulation, and endocrine pathway activation.
Preclinical research indicates predictable endocrine activation; however, long-term human safety data are limited. It is supplied strictly for research use and is not FDA-approved.
GHRP-2 binds to and activates the ghrelin receptor (GHS-R1a), which is expressed primarily on somatotrope cells in the anterior pituitary but also in the hypothalamus, pancreas, and cardiac tissue. This binding triggers intracellular calcium ion influx and activates cAMP/PKA and IP3/DAG signaling cascades, producing a potent, high-amplitude pulsatile GH release. It achieves this through two complementary mechanisms — directly stimulating pituitary somatotropes to release stored GH, and inhibiting somatostatin, the natural brake on GH secretion, thereby both amplifying each pulse and prolonging its duration. It also acts on the hypothalamus to promote additional GHRH release. Combining GHRP-2 with a GHRH analog like CJC-1295 or Mod GRF 1-29 produces synergistically larger GH pulses than either compound alone — GHRP-2 inhibits somatostatin and increases the number of somatotropes involved in the pulse, while GHRH increases pulse amplitude per cell. GHRP-2 is not lipogenic unlike ghrelin itself, meaning it does not promote fat storage despite sharing the same receptor.
Both are ghrelin receptor agonists producing pulsatile GH release, but with important differences. GHRP-2 is a more potent GH stimulator than Ipamorelin and also stimulates cortisol, prolactin, and ACTH — though at lower levels than the first-generation GHRP-6. Ipamorelin was specifically engineered for high selectivity to avoid these hormonal side effects entirely. GHRP-2 also reliably and significantly stimulates appetite — in a published human study subjects ate 35.9% more when infused with GHRP-2 versus saline — making it relevant in cachexia and appetite research but a practical consideration for body composition protocols. Ipamorelin does not meaningfully stimulate appetite at standard doses. GHRP-2 produces somewhat larger GH pulses than Ipamorelin but at the cost of less hormonal selectivity.
GHRP-2 has been studied across several domains. In GH deficiency assessment it is approved in Japan as a diagnostic provocative test agent. In body composition research it has shown increases in lean muscle mass, myofiber diameter, and skeletal muscle volume in animal studies. Sleep quality research suggests it enhances deep slow-wave sleep by amplifying nocturnal GH pulses. It has been studied for cachexia and appetite stimulation in conditions involving muscle wasting. Anti-inflammatory properties have been documented, with GHS-R1a receptors present in cardiac and immune tissue playing a role in tissue protection. Connective tissue repair through IGF-1-driven collagen synthesis and matrix remodeling is also a researched application, commonly leading to its use alongside BPC-157 and TB-500 in recovery-focused stacks.
GHRP-2 is given by subcutaneous or intramuscular injection. It has a short half-life — peak GH concentrations occur approximately 15 minutes after injection and return toward baseline within 60 minutes. This rapid clearance requires dosing two to three times daily to maintain GH optimization. Research and anecdotal protocols typically use doses of 100 to 300 mcg per injection. Like Ipamorelin, it should be timed on an empty stomach to avoid insulin blunting of the GH response. Bedtime dosing is particularly valued for amplifying the natural nocturnal GH surge during deep sleep. It is commonly stacked with CJC-1295 No DAC or Mod GRF 1-29 for synergistic dual-pathway GH stimulation.
GHRP-2 has a broader side effect profile than Ipamorelin due to its less selective receptor activity. The most commonly reported effects are significantly increased appetite — a direct and reliable effect that must be factored into any body composition protocol — water retention, lethargy, and tingling or numbness in the extremities. Elevated cortisol is a documented effect, though generally modest at standard doses. Elevated prolactin can occur and is relevant for anyone with prolactin-sensitive conditions. These hormonal side effects are considerably more pronounced with GHRP-6 and considerably less pronounced with Ipamorelin — GHRP-2 sits in the middle of the GHRP selectivity spectrum. Long-term sustained GH and IGF-1 elevation carries the same theoretical concerns — insulin resistance, joint discomfort, and potential effects on cell growth — applicable to all compounds in this class.
People with active cancer or a history of cancer should not use it given IGF-1's established role in cell growth promotion. Those with diabetes or significant insulin resistance should exercise caution as GH elevation worsens glucose control and GHRP-2's appetite stimulation compounds caloric intake management. People with elevated prolactin, pituitary tumors, or cortisol-related conditions should avoid it. Competitive athletes are prohibited from its use under WADA regulations — it is banned under the Peptide Hormones, Growth Factors, and Related Substances category. Pregnant or breastfeeding women should not use it. It cannot be legally compounded in the United States as it has no FDA approval for therapeutic use.





