



CJC-1295 No DAC
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
CJC-1295 No DAC: A Different Pharmacology, Not Just a Shorter Version of the Same Peptide
CJC-1295 No DAC is the GHRH-analogue form that lacks DAC modification — and that is the whole point. It should not be casually merged with the with DAC version, because the FDA explicitly describes them as different active moieties. In a research context, No DAC is interesting precisely as the shorter-acting branch of GHRH pharmacology, without the albumin-binding prolongation mechanism; in other words, the discussion here is really about a different pharmacology, not simply "the same peptide, just shorter."
In the published literature, the open human evidence base for No DAC is noticeably weaker than for the DAC version, which makes it especially easy to confuse a plausible physiologic concept with genuinely demonstrated data. And that is exactly what makes the molecule interesting to a careful reader: it sits at the intersection of a coherent mechanism, nomenclature confusion, and a very uneven evidence base.
Put more simply, this is one of those cases where one very small word — "No" — changes almost the entire meaning. If peptides interest you not because of forum mythology but because of how their logic changes at the level of structure and evidence, CJC-1295 No DAC is at the very least worth a closer look.
CJC-1295 Without DAC (Modified GRF 1-29): A Scientific Review
Based on peer-reviewed literature and regulatory documents — see References. Last updated: April 2026.
The Short Version
“CJC-1295 without DAC” is one of the most confusingly named compounds in the research peptide space. It sounds like a simpler version of CJC-1295 — as if the DAC technology were removed from an otherwise identical drug. That framing is backward.
The compound now widely sold as “CJC-1295 without DAC” is not derived from CJC-1295. It is better understood as a stabilised descendant of sermorelin — the synthetic GHRH(1-29) fragment that was genuinely FDA-approved for growth hormone deficiency in children from 1997 until its manufacturer discontinued it in 2008. Four amino acid substitutions were made to sermorelin’s sequence to extend its stability and resistance to enzymatic breakdown, producing a compound known properly as Modified GRF (1-29), or Mod-GRF.
The name “CJC-1295 without DAC” was popularised by the research chemical and fitness supplement communities, not by any pharmaceutical developer or scientific authority. It has caused extensive confusion — sometimes leading to the published human pharmacokinetic data from CJC-1295 with DAC being wrongly cited as evidence for this compound. Modified GRF 1-29 has genuine pharmacological plausibility, but it has no independent published human clinical trials demonstrating its safety or efficacy.
| At a glance | |
|---|---|
| Primary scientific name | Modified GRF (1-29), Mod-GRF(1-29), tetrasubstituted GRF(1-29) |
| Common market names | CJC-1295 without DAC, CJC-1295 no DAC, Mod GRF |
| Related compound | Sermorelin (GRF(1-29)) — same receptor, different sequence |
| Amino acid length | 29 amino acids |
| Molecular weight | ~3,368 Da |
| Half-life | ~30 minutes |
| Mechanism | GHRH receptor agonist → pituitary GH release |
| GH release pattern | Pulsatile burst — mimics physiological GHRH |
| FDA status | ❌ Not approved; not sermorelin |
| Sermorelin status | Commercially discontinued 2008 (not for safety) |
| Human trials published | ❌ None specific to Modified GRF(1-29) |
| WADA status | ❌ Prohibited (growth hormone secretagogue) |
The Identity Problem: What This Compound Actually Is
The family tree
Full-length human GHRH is a 44-amino acid peptide. In the 1980s, researchers discovered that the first 29 amino acids — GHRH(1-29) — retain the full biological activity of the 44-amino acid sequence at the GHRH receptor. This shorter fragment became known as GRF(1-29) and was developed into sermorelin — the compound that received FDA approval in 1997.[4]
Sermorelin has one critical pharmacological weakness: an extremely short half-life of about 5–12 minutes, due to rapid cleavage by dipeptidyl peptidase-4 (DPP-4) at the N-terminus. To address this, researchers introduced four amino acid substitutions:
| Position | Sermorelin (original) | Modified GRF(1-29) | Purpose of substitution |
|---|---|---|---|
| 2 | L-Alanine | D-Alanine | Blocks DPP-4 cleavage — primary stability gain |
| 8 | Asparagine | Glutamine | Reduces deamidation / structural rearrangement |
| 15 | Glycine | Alanine | Enhances receptor binding affinity |
| 27 | Methionine | Leucine | Prevents oxidation during manufacture and in vivo |
The resulting compound — Modified GRF(1-29) — has a half-life of approximately 30 minutes versus sermorelin’s 5–12 minutes. It is not a GHRH analogue with a radically novel mechanism — it is an optimised, more stable version of sermorelin.[1]
Why “CJC-1295 without DAC” is a misleading name
CJC-1295 with DAC was developed by ConjuChem as a 30-amino acid compound with the same four substitutions as Modified GRF(1-29) plus an additional lysine residue at position 30 bearing the maleimidopropionyl-DAC group. If you took CJC-1295 with DAC and literally removed the DAC technology, you would get a 30-amino acid peptide with a free reactive maleimido group — not a clean 29-amino acid GHRH analogue. “CJC-1295 without DAC” as typically sold is Modified GRF(1-29), which was never CJC-1295 minus its DAC. The name is a market construct that implies a lineage that does not exist.[2]
Mechanism of Action
GHRH receptor activation
Modified GRF(1-29) binds to the GHRH receptor (GHRHR) on somatotroph cells in the anterior pituitary — a Gs-coupled GPCR. Receptor activation increases intracellular cyclic AMP via adenylyl cyclase, activating protein kinase A, which drives both immediate GH secretion from vesicles and longer-term GH gene transcription. Because of the D-Ala substitution at position 2, the peptide resists DPP-4 cleavage, extending its active window to roughly 30 minutes.
Pulsatile GH release
The 30-minute half-life means Modified GRF(1-29) produces a discrete, time-limited burst of GH secretion following injection — pharmacologically analogous to the natural episodic GHRH releases the hypothalamus generates. Critically, this pulsatile pattern remains subject to the normal somatostatin feedback loop. Because the compound is gone from circulation within 30–60 minutes, the somatostatin counter-regulation has time to fully reset between doses. This makes it pharmacodynamically very similar to sermorelin and quite different from CJC-1295 with DAC, which continuously occupies GHRH receptors across a 6–8 day window.
The physiological argument for pulsatile GH
Many practitioners and researchers who favour Modified GRF(1-29) over the DAC version argue that pulsatile GH exposure is more physiologically appropriate than sustained elevation. There is a genuine pharmacological basis: many of GH’s anabolic effects are pulse-amplitude dependent rather than area-under-the-curve dependent; continuous GH exposure leads to downregulation of GH receptors over time; and the pulsatile pattern preserves the normal hypothalamic-pituitary feedback architecture. The counter-argument is that the clinical data for compounds with sustained GH/IGF-1 elevation (tesamorelin, CJC-1295 with DAC) demonstrates measurable physiological effects, while Modified GRF(1-29)’s brief exposure window generates a smaller integrated GH signal per dose. Neither argument is settled in the absence of head-to-head human comparisons.
The Combination with Ipamorelin: The Standard Clinical Use Case
Modified GRF(1-29) is rarely discussed in isolation in clinical or wellness settings. The combination of “CJC-1295 without DAC + ipamorelin” has become one of the most commonly prescribed peptide protocols in the US and other markets — routinely offered by anti-ageing, men’s health, and functional medicine practices.
Ipamorelin is a growth hormone-releasing peptide (GHRP) that acts through the ghrelin receptor (GHS-R) rather than the GHRH receptor. Where Modified GRF(1-29) tells the pituitary “release GH now via the GHRH pathway,” ipamorelin tells the pituitary “release GH now via the ghrelin pathway.” Because the two signals reach the same somatotroph cells through different receptors, co-administering them is pharmacologically logical. A key practical advantage of ipamorelin is selectivity: unlike older GHRPs (GHRP-6, hexarelin), ipamorelin does not meaningfully elevate cortisol or prolactin alongside GH.[8]
| Feature | Modified GRF(1-29) alone | Ipamorelin alone | Combination |
|---|---|---|---|
| GH release mechanism | GHRH receptor (Gs-cAMP) | Ghrelin receptor (GHS-R) | Dual receptor activation |
| GH pulse magnitude | Moderate | Moderate | Greater than either alone |
| IGF-1 elevation | Transient (pulse-dependent) | Transient (pulse-dependent) | Transient but larger |
| Cortisol/prolactin elevation | No | No | No |
| Published combination human trial data | ❌ None | ||
Comparison with Sermorelin: Essentially the Same Mechanism, Slightly Different Structure
| Feature | Sermorelin (GRF 1-29) | Modified GRF(1-29) / CJC-1295 no DAC |
|---|---|---|
| Amino acid length | 29 | 29 |
| Key modifications | None (native sequence) | 4 substitutions (D-Ala², Gln⁸, Ala¹⁵, Leu²⁷) |
| Half-life | ~5–12 minutes | ~30 minutes |
| GH release pattern | Pulsatile | Pulsatile |
| GHRH receptor | Yes | Yes |
| DPP-4 resistance | No | Yes (D-Ala at position 2) |
| FDA approval history | ✅ Approved 1997 (Geref); commercially discontinued 2008 | ❌ No |
| Published human trials | Multiple (children: GHD; adults: diagnostic use) | ❌ None independent |
| Compounding availability (US) | Yes — available through licensed compounders | Yes — widely available; less regulatory clarity |
Sermorelin was discontinued in 2008 due to manufacturing difficulties — not safety issues. The FDA has published a determination confirming that sermorelin (Geref) was not withdrawn for reasons of safety or effectiveness — a legally significant finding that allows compounding pharmacies to continue preparing it.[5] Modified GRF(1-29) does not have this history. No FDA-approved product based on its sequence has ever been marketed.
The Human Evidence Situation: Borrowed Evidence and Genuine Gaps
What sermorelin evidence establishes
Sermorelin has a substantive human evidence base: FDA-approved clinical trials demonstrating GH stimulation in GH-deficient children, with increased height velocity in 74% of treated children at 6 months; diagnostic use studies; adult studies showing increased GH and IGF-1 with acceptable short-term tolerability; and a multi-decade clinical use history before commercial discontinuation.[6][7]
What this does and does not tell us about Modified GRF(1-29)
The mechanistic inference is reasonable: Modified GRF(1-29) shares the same four amino acid substitutions as the core of CJC-1295, activates the same receptor, and produces GH pulses through the same pathway. It plausibly works as a GHRH agonist in humans. What no published trial establishes for Modified GRF(1-29) specifically: the magnitude of GH elevation per dose in humans; IGF-1 elevation pattern with the specific Modified GRF sequence; pharmacokinetic parameters (t½, Cmax, AUC) in humans; efficacy for any clinical endpoint; or safety under repeated dosing over months. The compound is used by large numbers of people based on pharmacological inference from closely related compounds — an honest gap in its own evidence base.
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) | ❌ Not approved; no approved product based on Modified GRF(1-29) sequence |
| Sermorelin (closely related) | Commercially discontinued 2008; not for safety; compoundable under appropriate frameworks [5] |
| Modified GRF(1-29) | No equivalent regulatory history; available from compounders but without sermorelin’s prior approval anchor |
| WADA | ❌ Prohibited — growth hormone secretagogue [12] |
Safety: Short-Acting Advantages and Remaining Unknowns
Advantages of the short half-life for safety
One genuinely favourable feature of Modified GRF(1-29) compared to CJC-1295 with DAC is pharmacokinetic reversibility: any adverse effect from a single injection will resolve within 30–60 minutes as the peptide clears. There is no “trapped” 6–8 day pharmacological stimulus that cannot be reversed. This makes dose titration simpler and adverse effect management more tractable.
Common adverse effects (class effects)
Modified GRF(1-29) produces the same class effects as other GHRH agonists: transient flushing or warmth after injection (NO-mediated vasodilation from acute GH pulse); water retention/oedema with repeated dosing at higher doses; headache; injection site reactions (erythema, pruritus, mild pain); and transient fatigue or somnolence, particularly if dosed at night. These effects are typically short-lived given the 30-minute half-life.
Longer-term safety unknowns
⚠️ The same concerns that apply to any compound that chronically elevates IGF-1 apply here: no long-term cancer surveillance data exists; no systematic monitoring of pituitary somatotroph proliferation in human users; no data on interactions with insulin sensitivity in individuals with metabolic risk; and no published safety data in women, many of whom use this compound through compounding clinics.
GHRH agonists require intact pituitary function
An important point often missed in wellness marketing: Modified GRF(1-29) and its combination with ipamorelin only work if the pituitary somatotroph population is functional. They stimulate GH release from existing somatotrophs — they cannot replace a non-functional pituitary. In individuals with true pituitary GH deficiency, they will not produce a meaningful response.[8]
Comparison with Related GHRH-Axis Compounds
| Compound | Mechanism | Half-life | Human evidence | FDA status |
|---|---|---|---|---|
| Modified GRF(1-29) | GHRH receptor agonist | ~30 min | ❌ None independent | ❌ Not approved |
| Sermorelin | GHRH receptor agonist | ~5–12 min | Multiple clinical trials | Discontinued 2008; not for safety |
| Tesamorelin (Egrifta) | GHRH analogue | ~26 min (daily SC) | Phase 3 completed | ✅ Approved (HIV lipodystrophy) |
| CJC-1295 with DAC | GHRH receptor agonist + albumin binding | ~6–8 days | 2 Phase 1/2 PK studies | ❌ Not approved; Phase 2 discontinued |
| Ipamorelin | Ghrelin receptor agonist | ~2 hours | Phase 2 (negative); limited other | ❌ Not approved |
| Recombinant hGH | Direct GH replacement | Dose-dependent | Extensive; 30+ years | ✅ Approved (multiple indications) |
Common Misconceptions
“CJC-1295 without DAC is just CJC-1295 with the DAC removed — same compound, shorter acting.”
It is not. The compound sold as “CJC-1295 without DAC” is Modified GRF(1-29), a 29-amino acid GHRH analogue descended from sermorelin. CJC-1295 with DAC was a 30-amino acid compound with a proprietary reactive group enabling albumin binding. They share the same four amino acid substitutions in the GHRH core but differ in length, structure, pharmacokinetics, and origin.[2]
“The human clinical data for CJC-1295 proves Modified GRF works.”
The Teichman 2006 and Ionescu & Frohman 2006 studies were conducted using CJC-1295 with DAC — the 30-amino acid albumin-binding compound.[9][10] Their pharmacokinetic findings (6–8 day half-life; 2–10x GH elevation for 6+ days) describe the DAC version’s specific properties and cannot be directly applied to the no-DAC compound.
“Combining it with ipamorelin is well-studied and proven.”
The combination is widely used and the mechanistic rationale is sound. But no published randomised controlled trial has evaluated the combination’s efficacy for any clinical outcome. Practitioner reports and pharmacological logic are not the same as clinical trial evidence.
“It’s safer than sermorelin because it’s a newer, improved version.”
Sermorelin’s safety profile is actually better characterised than Modified GRF(1-29)’s, because sermorelin was FDA-approved and used clinically for years.[4] Modified GRF(1-29) is structurally similar and probably has a comparable safety profile — but it lacks sermorelin’s documented human exposure history.
Frequently Asked Questions
Is CJC-1295 without DAC the same as sermorelin?
No — but they are closely related. Both are 29-amino acid GHRH receptor agonists with very short half-lives and pulsatile GH release profiles. Modified GRF(1-29) has four amino acid substitutions relative to sermorelin that provide greater enzymatic stability and a slightly longer half-life (~30 min vs. ~5–12 min). They are different molecules but pharmacologically very similar.
Does it have its own human trials?
No published randomised controlled trial has specifically studied Modified GRF(1-29) as its primary compound. Human evidence is inferred from sermorelin and from CJC-1295 with DAC — not directly established.
Why is it called “CJC-1295 without DAC”?
The name was popularised in the research chemical and performance community to align it with the better-known CJC-1295 brand identity. It is not a name used by any pharmaceutical developer or regulatory authority. Modified GRF(1-29) or Mod-GRF is the more scientifically accurate designation.[1]
Can it be legally compounded in the US?
Unlike BPC-157 (Category 2 — cannot be compounded) and CJC-1295 with DAC (not added to 503A bulks list), Modified GRF(1-29) exists in a less explicitly regulated space. Sermorelin, its close relative, can be compounded under appropriate frameworks. The legal landscape for Modified GRF(1-29) specifically is less clearly defined.[11]
Is it better than sermorelin?
They are so pharmacologically similar that the question is difficult to answer definitively without head-to-head human trials. Modified GRF(1-29)’s DPP-4 resistance and slightly longer half-life represent marginal technical improvements. Sermorelin has a more established safety history and clearer regulatory status. Neither has strong evidence of clinical superiority over the other for adults.
Key Takeaways
- “CJC-1295 without DAC” is a marketing name for Modified GRF(1-29) — a stabilised GHRH analogue descended from sermorelin. It was not developed by ConjuChem and is not CJC-1295 with the DAC removed.[2]
- The compound has no independent published human clinical trials. Its evidence base is inferred from sermorelin (same receptor, similar structure, longer history) and from the CJC-1295 with DAC pharmacology studies (same four-substitution core, fundamentally different pharmacokinetics).
- The mechanism is legitimate and well-characterised. GHRH receptor agonism drives pulsatile GH release through the physiological pituitary pathway — the same as sermorelin and tesamorelin, just with slightly better enzymatic stability.
- The short half-life (~30 min) is a genuine safety advantage over CJC-1295 with DAC: adverse effects cannot persist for days, dose titration is practical, and normal somatostatin feedback fully resets between doses.
- The combination with ipamorelin has pharmacological logic but no clinical trial data. Dual GHRH + ghrelin receptor stimulation produces greater GH release than either alone in theory and in practice — but the combination has not been evaluated in rigorous human outcome trials.
- For anyone seeking GHRH-axis support for a genuine medical indication, tesamorelin remains the only FDA-approved option. For those using compounded GHRH analogues, sermorelin has the stronger regulatory history. Modified GRF(1-29) sits in a grey zone — pharmacologically plausible, structurally close to approved compounds, but without its own independent human evidence base.
References
Structural and Mechanistic Background
- Wikipedia. Modified GRF (1-29). en.wikipedia.org/wiki/Modified_GRF_(1-29)
- Wikipedia. CJC-1295 — Nomenclature section on false equivalence with Modified GRF(1-29). en.wikipedia.org/wiki/CJC-1295
- Jetté L, et al. Human growth hormone-releasing factor (hGRF)1-29-albumin bioconjugates activate the GRF receptor on the anterior pituitary in rats: identification of CJC-1295 as a long-lasting GRF analog. Endocrinology. 2005;146(7):3052–3058. PMID: 15817669
Sermorelin Evidence Base (Closely Related)
- FDA approval history: Sermorelin acetate (Geref), NDA 020443. Approved 1997; commercial discontinuation 2008.
- FDA Federal Register. Determination that GEREF (sermorelin acetate) was not withdrawn from sale for reasons of safety or effectiveness. Federal Register. March 4, 2013.
- Corpas E, Harman SM, Piñeyro MA, et al. Growth hormone (GH)-releasing hormone-(1-29) twice daily reverses the decreased GH and insulin-like growth factor-I levels in old men. Journal of Clinical Endocrinology & Metabolism. 1992;75(2):530–535. PMID: 1379256
- Walker RF. Sermorelin: a better approach to management of adult-onset growth hormone insufficiency? Clinical Interventions in Aging. 2006;1(4):307–308. PMC2699646
- Ishida J, Saitoh M, et al. Growth hormone secretagogues: history, mechanism of action, and clinical development. JCSM Rapid Communications. 2020. doi: 10.1002/rco2.9
CJC-1295 with DAC Human Studies (for context)
- Teichman SL, Neale A, Lawrence B, et al. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. Journal of Clinical Endocrinology & Metabolism. 2006;91(3):799–805. PMID: 16352683
- Ionescu M, Frohman LA. Pulsatile secretion of growth hormone (GH) persists during continuous stimulation by CJC-1295, a long-acting GH-releasing hormone analog. Journal of Clinical Endocrinology & Metabolism. 2006;91(12). PMID: 17018654
Regulatory Documents
- FDA PCAC Briefing Document: Ipamorelin; CJC-1295; sermorelin combinations. December 2024. fda.gov
- WADA. Prohibited List — Growth Hormone Secretagogues. wada-ama.org
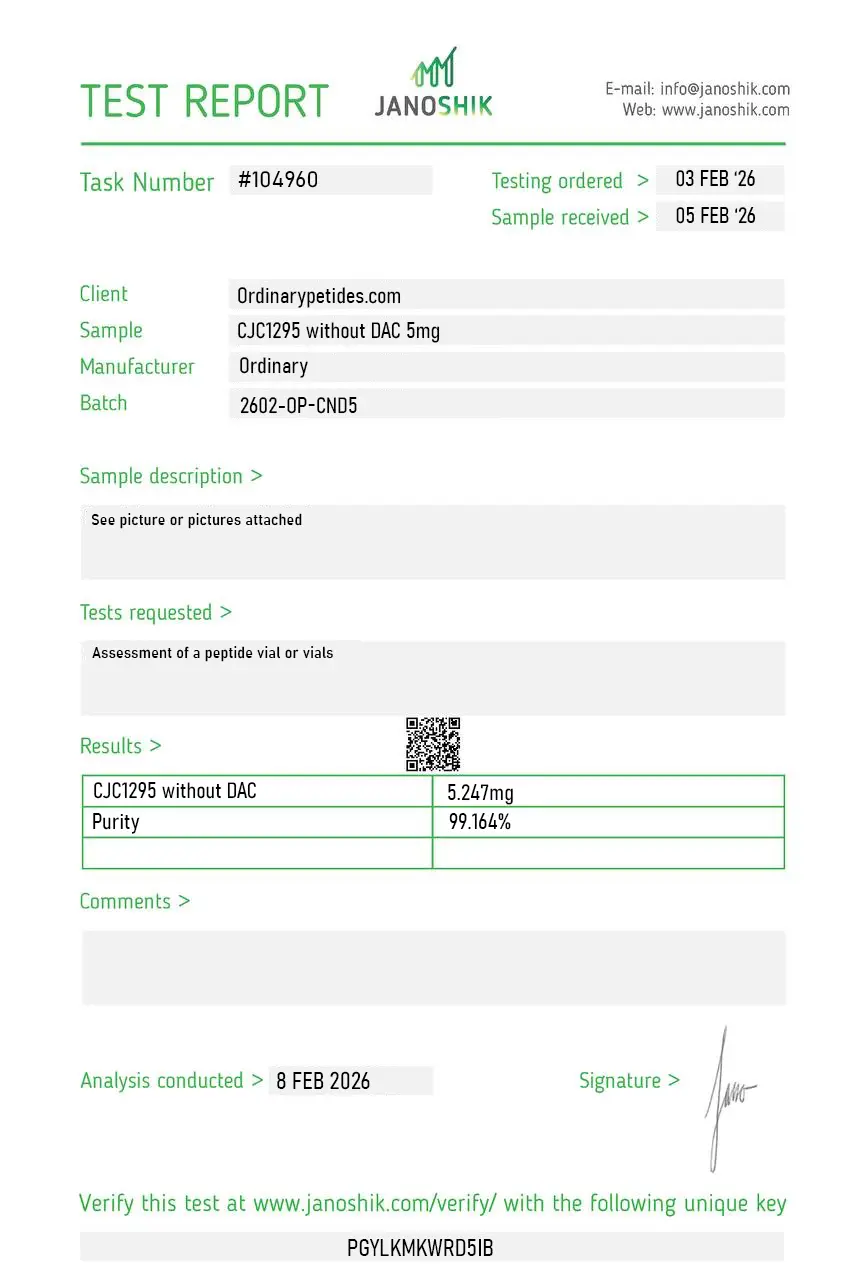
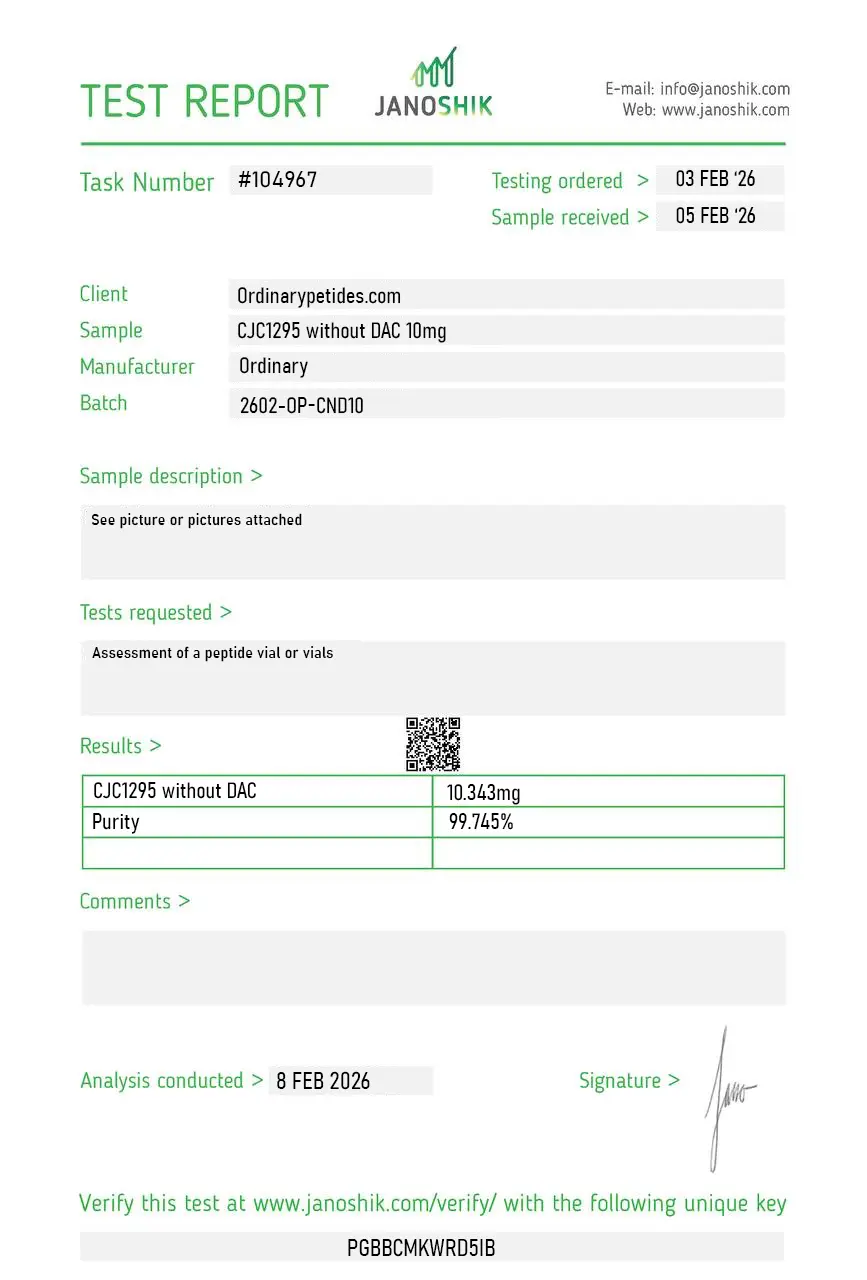
Certificate of Analysis
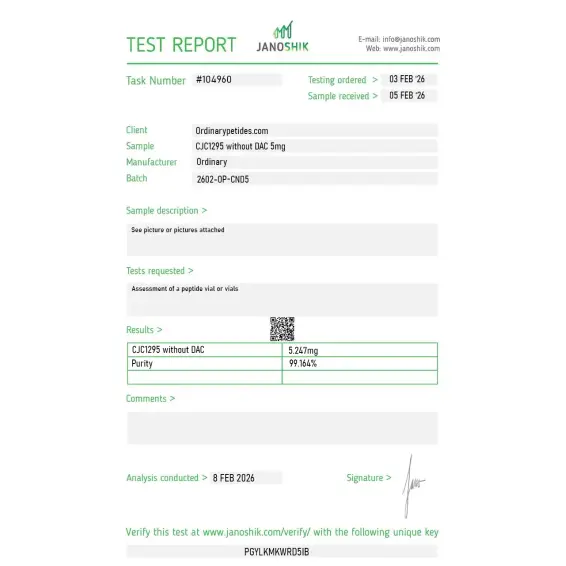
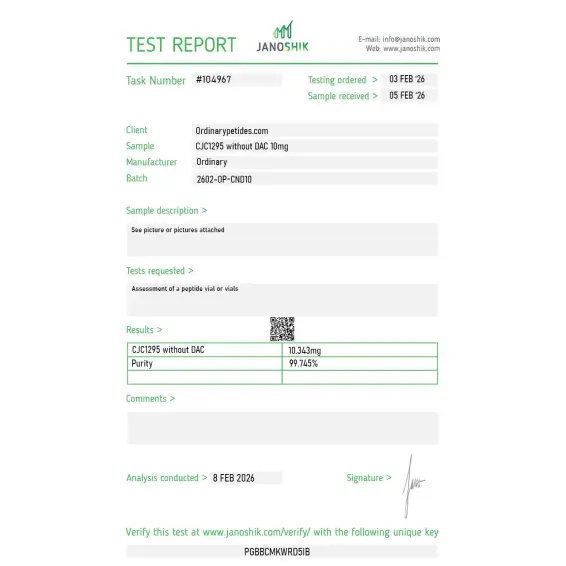
Independent test reports are available for CJC-1295 without DAC 2mg, 5mg, and 10mg batches. These reports provide batch-level documentation and analytical verification information for research reference.

Based on 3 reviews
5.0
We anchor the pulsatile end of a GHRH-receptor desensitization study with it — comparing brief repeated No-DAC pulses against sustained DAC exposure to map how the receptor downregulates under each regime. The No-DAC's rapid clearance is precisely what lets us deliver discrete pulses rather than a continuous signal. Sourcing both forms with matched documentation keeps the only variable the exposure kinetics, and the material held its rapid-clearance profile across our pulses.
What earned the order is the listing keeping the No-DAC clearly separate from both the DAC version and base sermorelin — three GHRH-receptor agonists with half-lives spanning two orders of magnitude, and a vendor that doesn't blur them is one I trust for kinetic work. For receptor-pathway studies where the exposure profile is the experimental variable, that labeling precision was the deciding factor. Consistent across two orders.
The short half-life is the whole reason we use the No-DAC form — without the albumin-binding linker it clears in about thirty minutes, which gives the pulsatile GHRH-receptor activation profile that matches physiologic GHRH pulsing far better than the week-long DAC version's tonic exposure. For studying receptor behavior under pulsatile rather than continuous stimulation, the No-DAC is the correct tool, and the material reproduced that brief-activation profile in our somatotroph timecourse.
No. It is not FDA-approved for therapeutic use and is supplied strictly for laboratory research purposes.
The No DAC version produces short, pulse-like activity, while DAC variants create extended elevation. The preferred option depends on the intended research objective.
In experimental models, CJC-1295 (No DAC) has been shown to stimulate growth hormone release via activation of pituitary GHRH receptors.
Yes. It is a synthetic peptide analogue of GHRH.
It means the absence of the Drug Affinity Complex that gives the DAC version its albumin-binding prolongation of action.
No. CJC-1295-related substances are not currently FDA-approved therapies.
For the No DAC form, the open and reliable human evidence base is limited. The best-known early GH/IGF-1 data belong to the long-acting CJC-1295 context and cannot be automatically transferred to No DAC.
By the absence of DAC modification and therefore by having different pharmacology. FDA explicitly states that the forms are not interchangeable.
No. CJC-1295 is prohibited by WADA as a GHRH analogue.
CJC-1295 without DAC — also called Modified GRF(1-29), Mod GRF 1-29, or sometimes incorrectly sold as "CJC-1295" without specification — is a synthetic analog of the first 29 amino acids of naturally occurring growth hormone-releasing hormone (GHRH). It was created by modifying four amino acid positions in the native GHRH(1-29) sequence to improve stability and resistance to enzymatic breakdown while retaining full biological activity at GHRH receptors. It does not contain the Drug Affinity Complex that defines the DAC version — meaning it does not bind albumin and clears from the body rapidly. It is not FDA-approved and cannot be legally compounded in the United States.
The critical difference is half-life and release pattern. CJC-1295 without DAC has a half-life of approximately 30 minutes — after injection it produces a sharp, concentrated pulse of growth hormone from the pituitary and is then rapidly cleared. CJC-1295 with DAC has a half-life of 6 to 8 days due to albumin binding, producing a sustained but non-physiological elevation of GH and IGF-1. The No DAC version closely mimics the body's natural pulsatile GHRH secretion pattern. This pulsatile rhythm is considered physiologically important because GH receptors — like most receptors — are susceptible to desensitization under conditions of sustained, non-pulsatile stimulation. Maintaining the pulse-and-rest pattern preserves receptor sensitivity and endocrine feedback integrity over time.
It binds to GHRH receptors on somatotrope cells in the anterior pituitary, triggering a brief but potent surge of growth hormone release into circulation. The GH pulse then stimulates hepatic IGF-1 production. Because the peptide clears within 30 minutes, the GH elevation is time-limited — rising sharply and then returning toward baseline — mimicking what the hypothalamus naturally does during sleep or exercise-induced GH release. When combined with a GH-releasing peptide such as Ipamorelin, which activates the separate ghrelin receptor pathway, the dual signal produces a significantly larger GH pulse than either compound alone — analogous to how the body naturally uses both GHRH and ghrelin-like signals to coordinate GH secretion.
Because it works through the same downstream GH-IGF-1 axis, the reported benefits are largely identical to those of the DAC version — improved body composition through increased lean mass and reduced fat, faster recovery from exercise and injury, improved deep sleep quality and duration, increased energy, anti-aging effects on skin and connective tissue, and enhanced bone density support over time. The distinction is in how these benefits are achieved — through physiologically timed pulses rather than sustained elevation — which some physicians and researchers argue produces a more favorable long-term hormonal profile with less risk of receptor downregulation, insulin resistance, and IGF-1 overexposure.
Because of its short half-life, CJC-1295 without DAC requires more frequent dosing than the DAC version — typically administered once to three times daily. It is given by subcutaneous injection and must be timed carefully for maximum effect. It is most effective when injected on an empty stomach — ideally 2 hours after eating and at least 30 minutes before the next meal — because elevated insulin from food blunts GH secretion. Bedtime administration is particularly popular because it amplifies the natural GH surge that occurs during slow-wave sleep. Typical research doses range from 100 to 300 mcg per injection. It is most commonly stacked with Ipamorelin in clinical and wellness protocols.
Side effects are generally mild and short-lived given the rapid clearance. Commonly reported effects include temporary flushing immediately after injection, mild water retention, tingling or numbness in the extremities, headache, and increased appetite. Injection site reactions are also reported. A key practical advantage over the DAC version is that if side effects occur they resolve within hours rather than persisting for days. This also makes dose adjustment much more straightforward — if a dose is too high or causes unwanted effects, the next injection can simply be reduced or skipped. The same theoretical long-term concerns about sustained IGF-1 elevation apply if the compound is used continuously at high frequency over extended periods.
The same contraindications apply as for the DAC version. People with active cancer or a history of cancer should avoid it due to IGF-1's role in cell growth promotion. Those with diabetes, insulin resistance, or pituitary disorders should not use it without physician guidance. Pregnant or breastfeeding women should not use it. Athletes subject to anti-doping testing should be aware it is detectable and prohibited under WADA. As it is not FDA-approved and cannot be legally compounded in the United States, any product obtained outside a clinical setting carries unverified purity and potency risks.





