
CJC-1295 (No DAC) + Ipamorelin
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
CJC-1295 (No DAC) + Ipamorelin: An Interesting Endocrine Hypothesis With Early Signals and an Honest Evidence Gap
CJC-1295 (No DAC) / Ipamorelin is a popular GH-axis stack in which one peptide belongs to the class of GHRH analogues and the other to growth hormone secretagogues. That is precisely why interest in the pairing rests on a biologically intelligible premise: two different signaling routes converging on the same endocrine axis. In the research context, ipamorelin does have early human PK/PD data showing a dose-dependent GH response, whereas discussion of the combination itself tends to revolve far more around theoretical mechanistic complementarity than around a strong direct clinical evidence base.
The key nuance is this: CJC-1295 No DAC must not be conflated with the with-DAC version. The FDA explicitly emphasizes that these are different active moieties, which means the headline numbers attached to the DAC form should not be casually "relocated" into this duo as though they came with complimentary baggage. In preclinical and review-based discussions, the pairing looks scientifically plausible, but for the actual outcomes people usually seek it for, the evidence is described as limited.
Put simply, this is not the story of a "proven stack." It is the story of an interesting endocrine hypothesis, some early signals for the individual components, and a rather noticeable gap between marketing confidence and data quality. If you are interested in peptides not for their forum mythology but for the exact point where mechanism ends and evidence begins, this duo is well worth a closer look.
CJC-1295 (No DAC) + Ipamorelin: A Scientific Review of the Most Widely Prescribed Peptide Combination
Based on peer-reviewed literature and regulatory documents — see References. Last updated: April 2026.
The Short Version
“CJC-1295 / Ipamorelin” is the most widely prescribed peptide combination in the US and many other markets. It is routinely offered by anti-ageing, men’s health, longevity, and functional medicine clinics — often as the default entry point to “peptide therapy.” Online, it is presented with a confident clinical voice: accelerated fat loss, improved body composition, better sleep, faster recovery, increased muscle mass, enhanced energy. The marketing frequently implies that the evidence base is mature and the practice is well-established.
The pharmacological rationale for this combination is genuinely sound. CJC-1295 without DAC (properly called Modified GRF 1-29) and ipamorelin are two growth hormone-releasing agents that work through different receptors — one via the GHRH receptor, one via the ghrelin receptor — and their simultaneous use produces a greater GH pulse than either alone. The mechanistic logic is solid. Ipamorelin’s selectivity profile — stimulating GH without elevating cortisol or prolactin — is a genuine advancement over older GH-releasing peptides.
| At a glance — combination | |
|---|---|
| Component 1 | Modified GRF(1-29) / CJC-1295 no DAC — GHRH receptor agonist |
| Component 2 | Ipamorelin — ghrelin receptor (GHS-R1a) agonist |
| Combination mechanism | Dual-receptor GH axis stimulation |
| Published combination RCT data | ❌ None |
| FDA status — Modified GRF(1-29) | ❌ Not approved; not added to 503A bulks list |
| FDA status — ipamorelin | ❌ Not approved; PCAC voted against 503A inclusion Oct 2024; ipamorelin acetate now Category 2 |
| WADA status | ❌ Both prohibited (growth hormone secretagogues) |
Part 1 — Ipamorelin: The Better-Known Half
Origins and Discovery
Ipamorelin was developed by Novo Nordisk in the late 1990s as part of a systematic programme to find growth hormone-releasing peptides (GHRPs) with superior selectivity profiles. Earlier GHRPs — GHRP-6 and GHRP-2 — stimulated GH effectively but also elevated cortisol and ACTH, triggering a stress hormone response alongside the desired GH pulse. Ipamorelin did not release ACTH or cortisol in levels significantly different from those observed following GHRH stimulation, and this lack of effect was evident even at doses more than 200-fold higher than the ED50 for GH release.[1] This selectivity was the defining discovery. Ipamorelin was — and remains — the first GHRP-receptor agonist whose GH selectivity is genuinely comparable to GHRH itself.
Structure
Ipamorelin is a pentapeptide: five amino acids in the sequence Aib-His-D-2-Nal-D-Phe-Lys-NH&sub2;, where Aib is α-aminoisobutyric acid. It was derived from GHRP-1 through systematic modification, with structural features designed to improve metabolic stability and receptor selectivity.
| Property | Value |
|---|---|
| Structure | Aib-His-D-2-Nal-D-Phe-Lys-NH&sub2; (5 amino acids) |
| Molecular weight | ~711 Da |
| Receptor target | GHS-R1a (ghrelin receptor) |
| Half-life (estimated) | ~2 hours |
| GH release pattern | Pulsatile burst peaking ~40 min post-dose |
| Cortisol/ACTH effect | ✅ None at any studied dose |
| Prolactin effect | ✅ None |
| Developer | Novo Nordisk (Denmark) |
Mechanism of Action
Ipamorelin binds to and activates the growth hormone secretagogue receptor type 1a (GHS-R1a) — the ghrelin receptor — on somatotroph cells in the anterior pituitary. This receptor is distinct from the GHRH receptor activated by Modified GRF(1-29). The GHS-R1a is a Gq-protein-coupled receptor that increases intracellular calcium through the phospholipase C / IP&sub3; pathway — different from the Gs/cAMP pathway activated by GHRH receptor agonism. This mechanistic distinction is the pharmacological basis for the combination’s greater-than-additive effect on GH release.[3]
The Phase 2 Clinical Trial: The Most Important Human Evidence
Helsinn Therapeutics sponsored a Phase 2 randomised controlled trial of intravenous ipamorelin for postoperative ileus (POI) — the paralysis of bowel motility that frequently complicates abdominal surgery. One hundred seventeen patients were enrolled. Median time to first tolerated meal was 25.3 hours in the ipamorelin group and 32.6 hours in the placebo group (p = 0.15). Ipamorelin was well tolerated, but there were no significant differences in key efficacy analyses.[2]
Human Evidence Summary for Ipamorelin
| Study | Design | N | Finding |
|---|---|---|---|
| Raun et al. 1998 [1] | Preclinical (rats, swine) | Animals | Dose-dependent GH release; no ACTH/cortisol elevation; selectivity profile established |
| Phase 1 PK/PD | Healthy subjects | Small | GH peak at ~40 min; rapid decline; clean hormonal profile |
| Beck et al. 2014 [2] | Phase 2 RCT, POI | 117 patients | Well-tolerated; ❌ failed to meet primary endpoint (p=0.15) |
Part 2 — Modified GRF(1-29): Revisiting the Foundation
A comprehensive treatment of Modified GRF(1-29) appears in the dedicated article in this series. For the combination article, the key points are that Modified GRF(1-29) is a 29-amino acid GHRH receptor agonist with the same four stability-enhancing substitutions as CJC-1295 with DAC, but without the albumin-binding DAC group. It has a half-life of ~30 minutes, produces pulsatile GH release with somatostatin feedback preserved, and has no independent published human trials — its pharmacological inference is borrowed from sermorelin and CJC-1295 with DAC literature. It acts through the GHRH receptor (Gs-cAMP pathway), which is distinct from ipamorelin’s GHS-R1a (Gq-calcium pathway).[5][6]
Part 3 — The Combination: Mechanism, Rationale, and Evidence
Why the Combination Makes Pharmacological Sense
The GHRH receptor pathway and the ghrelin receptor pathway converge on the same pituitary somatotroph cells but use different second-messenger systems. Simultaneous stimulation through both pathways produces greater GH release than either pathway alone — a well-established principle in GH secretion biology.
Pathway 1 — Modified GRF(1-29): Binds GHRHR → Gs → cAMP ↑ → PKA activation → GH secretion
Pathway 2 — Ipamorelin: Binds GHS-R1a → Gq → PLC → IP&sub3; → intracellular Ca²+ ↑ → GH secretion
The calcium signal from ipamorelin synergises with the cAMP/PKA signal from Modified GRF, producing a supra-additive GH pulse. The specific claim that the combination produces 3–5× more GH than ipamorelin alone is reproduced across many clinical and educational sources — but derives from practitioner experience and extrapolation rather than published human pharmacokinetic data on the specific combination.[3]
Typical Dosing Protocol (as used clinically)
| Component | Typical dose | Frequency |
|---|---|---|
| Mod-GRF(1-29) | 100–200 µg | Co-administered with ipamorelin |
| Ipamorelin | 100–200 µg | 1–3× daily SC injection |
| Combined product | Often co-formulated in single vial | Once or twice daily (typically bedtime) |
| Cycle | 3–6 months, then off-cycle period | Physician-dependent |
What the Combination Is Claimed to Produce
| Claimed benefit | Pharmacological basis | Evidence quality |
|---|---|---|
| Increased GH pulse amplitude | Dual-receptor additive/synergistic GH release | Mechanistically solid; ❌ no combination RCT |
| Elevated IGF-1 over time | Downstream hepatic IGF-1 from cumulative GH pulses | Inferred from GH axis biology; ❌ no combination RCT |
| Fat loss / body composition | GH promotes lipolysis, fatty acid oxidation | Class effect (GH-axis); ❌ no combination-specific trial |
| Muscle mass | GH/IGF-1 promote protein synthesis | Class effect; ❌ no combination-specific trial |
| Improved sleep quality | GH axis / ghrelin receptors in hypothalamic sleep centres | Plausible; ❌ no combination RCT |
| Faster injury / surgical recovery | IGF-1-mediated tissue repair | Indirect evidence from GH literature; ❌ no combination RCT |
The Human Evidence Gap: Why This Matters
The wellness industry around this combination is large and growing — practitioners are prescribing it to healthy adults seeking anti-ageing benefits, athletes seeking performance enhancement, and patients seeking body composition changes. The argument commonly made is that the safety profile of the components is acceptable and the mechanism is sound, so waiting for RCT data would deny patients a beneficial intervention. This reasoning deserves honest evaluation.
The case for proceeding before RCTs: The GH axis is well-studied; the benefits of restored GH in GH-deficient adults are documented with recombinant GH; sermorelin (same mechanism as Modified GRF) has decades of clinical use with an acceptable safety history; and ipamorelin’s selectivity makes it safer than earlier GHRPs.
The case for caution: ⚠️ Most healthy adults being prescribed this combination do not have diagnosed GH deficiency — they have age-related GH decline, which is normal physiology, and the indication for treating it is not established. The magnitude of GH/IGF-1 elevation from the combination in healthy adults has not been quantified in controlled studies. Chronically elevated IGF-1 carries a theoretical but unquantified cancer risk. “The mechanism is sound” is not the same as “the intervention works for the stated purpose.”
The Regulatory Timeline for Ipamorelin: A Critical Recent History
| Date | Event |
|---|---|
| September 2023 | ⚠️ FDA placed ipamorelin on Category 2 of the 503A interim bulks list — “cannot be compounded” |
| Late 2023 – 2024 | Lawsuit filed (Evexias et al.) challenging FDA’s classification process |
| September 2024 | Settlement reached; FDA agreed to submit ipamorelin for formal PCAC review; ipamorelin acetate temporarily removed from Category 2 |
| October 29, 2024 | PCAC meeting: committee reviewed ipamorelin for 503A bulks list inclusion [8] |
| October 2024 | ❌ PCAC voted against adding ipamorelin to the 503A bulks list [9] |
| Post-October 2024 | ⚠️ Ipamorelin acetate placed back on Category 2 — cannot be legally compounded under 503A |
| April 2026 (current) | Ipamorelin acetate: Category 2; CJC-1295: not added to 503A bulks list; both widely sold as research chemicals |
Safety: Component-by-Component and Combination Considerations
Modified GRF(1-29) safety
Closely related to sermorelin, which has a multi-decade compounding and clinical use history with an acceptable short-term safety profile. Short half-life means effects resolve quickly. Common adverse effects: flushing, headache, injection site reactions, transient water retention. Long-term oncological safety not formally evaluated.
Ipamorelin safety
The Beck et al. (2014) RCT found ipamorelin well-tolerated in 117 surgical patients, with AE rates comparable to placebo (87.5% vs. 94.8% in a surgical population).[2] The key safety advantage over older GHRPs is confirmed: no cortisol/ACTH elevation even at >200× the GH-releasing ED50; no prolactin elevation. Long-term safety profile in healthy adults used chronically for GH optimisation: not formally studied.
Combination safety concerns
⚠️ Additive IGF-1 elevation: Both pathways converge on GH release, and cumulative daily GH stimulation over months produces sustained IGF-1 elevation. The theoretical cancer risk from chronic IGF-1 elevation applies here. Product quality variability: Given the regulatory turbulence around both compounds, quality and sterility of compounded products is highly variable. A combination that involves daily subcutaneous self-injection amplifies the consequences of any sterility failure. Insulin resistance: GH counter-regulation of insulin is a real metabolic effect. Chronic twice-daily GH stimulation in individuals with pre-existing insulin resistance warrants monitoring of fasting glucose. Pituitary requirement: Neither compound works in complete GH deficiency — they require a functional pituitary somatotroph population to produce any effect.
Comparison with the GH-Axis Landscape
| Option | Mechanism | Human evidence | Regulatory status |
|---|---|---|---|
| Mod-GRF + Ipamorelin | GHRH-R + GHS-R1a | ❌ No combination RCT; PK/PD only for components | ❌ Not approved; ipamorelin acetate Category 2 |
| Sermorelin alone | GHRH-R | Multiple clinical trials; FDA-approved 1997; discontinued 2008 | Compoundable (prior approval pathway) |
| Tesamorelin (Egrifta) | GHRH-R | Phase 3 completed | ✅ FDA-approved for HIV lipodystrophy |
| Recombinant hGH | Direct GH replacement | Extensive; 30+ years | ✅ FDA-approved (multiple indications) |
| Ipamorelin alone | GHS-R1a | Phase 2 POI (failed); PK/PD | ❌ Not approved; acetate Category 2 |
| MK-677 (ibutamoren) | Oral GHS-R1a agonist | Multiple trials incl. elderly; Phase 2 data | ❌ Not approved; PCAC voted against |
Common Misconceptions
“The combination is well-studied — doctors prescribe it all the time.”
Widespread clinical use does not constitute controlled evidence. The combination’s clinical adoption has outrun its evidence base. Without controlled trials, placebo effects, natural improvement, and concurrent lifestyle interventions cannot be disentangled from any observed benefits.
“It just restores your GH to youthful levels — that must be safe.”
Age-related GH decline is normal physiology, not a disease. The assumption that restoring GH to youthful levels produces benefits without risks is not supported by controlled evidence in otherwise healthy ageing adults. The recombinant GH literature in healthy elderly adults shows modest body composition effects alongside real adverse effects (fluid retention, carpal tunnel, insulin resistance).
“Ipamorelin is so selective it has no side effects.”
Selectivity for GH over cortisol/prolactin is a real advantage — but it is selectivity within the GH-axis pharmacological profile. The downstream effects of elevated GH and IGF-1 (insulin resistance, fluid retention, theoretical cancer risk) are class effects that apply regardless of how the GH was stimulated.
“Since both compounds were removed from Category 2 after the lawsuit, they’re now approved for compounding.”
The lawsuit settlement led to the FDA submitting the compounds for proper PCAC review — not to their approval. The PCAC subsequently voted against adding ipamorelin to the 503A bulks list.[9] Ipamorelin acetate is now back on Category 2. The compounds went through the proper review process and failed to gain compounding approval on their merits.
Frequently Asked Questions
Can the combination currently be legally compounded in the US?
Ipamorelin acetate was voted against by PCAC in October 2024 and placed back on Category 2 — meaning it cannot be legally compounded under the 503A framework.[8][9] CJC-1295 / Modified GRF was not added to the 503A bulks list in December 2024. The combination’s legal compounding pathway is not established under current FDA regulations.
Is the combination banned in sport?
Yes. Both ipamorelin and Modified GRF(1-29) / sermorelin analogues are classified as growth hormone secretagogues by WADA and are prohibited at all times in competitive sport.[12]
Is sermorelin + ipamorelin different from Modified GRF + ipamorelin?
Pharmacologically very similar — sermorelin and Modified GRF(1-29) activate the same GHRH receptor and produce the same type of pulsatile GH stimulation. Modified GRF is marginally more stable (4 amino acid substitutions). Sermorelin has the stronger regulatory history (prior FDA approval). The combination rationale is identical for both pairings.
Are there any ongoing trials of this combination?
No registered Phase 2 or Phase 3 trial of the Mod-GRF / ipamorelin combination for any patient-relevant endpoint appears in major clinical trial databases as of April 2026.
Key Takeaways
- The combination has a sound pharmacological basis. Dual-receptor GH axis stimulation — GHRH receptor (Modified GRF) and ghrelin receptor (ipamorelin) — is a legitimate mechanistic approach with additive or synergistic effects on GH pulse amplitude. The selectivity of ipamorelin (no cortisol/ACTH elevation) is a genuine advantage over earlier GHRPs.[1]
- ⚠️ No published controlled trial has evaluated this combination for any patient-relevant endpoint. The efficacy claims around fat loss, muscle mass, body composition, sleep, and recovery are mechanistic extrapolations and practitioner reports — not established clinical findings.
- ⚠️ The regulatory situation for ipamorelin deteriorated in late 2024. PCAC voted against 503A inclusion in October 2024. Ipamorelin acetate is now on Category 2 — cannot be legally compounded under the standard 503A framework.[9]
- The evidence hierarchy within the GH-axis space makes the combination look thin. Sermorelin (same mechanism as Modified GRF) has prior FDA approval and decades of clinical use. Tesamorelin has Phase 3 data. Recombinant GH has 30+ years of data. The combination being widely prescribed has less formal evidence than any of them.
- ⚠️ Product quality is a practical safety concern. The regulatory turbulence around these compounds has affected the supply chain for compounded products. Sterility, purity, and actual peptide content of unregulated research chemical products cannot be assumed.
- The widespread use of this combination reflects a genuine unmet need — declining GH axis function in ageing adults is real and affects quality of life. The honest answer is that the intervention may well produce benefits, but the evidence standard required to recommend it with confidence has not yet been met.
References
Ipamorelin Primary Literature
- Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. European Journal of Endocrinology. 1998;139(5):552–561. PMID: 9849822
- Beck DE, Sweeney WB, McCarter MD; Ipamorelin 201 Study Group. Prospective, randomized, controlled, proof-of-concept study of the Ghrelin mimetic ipamorelin for the management of postoperative ileus in bowel resection patients. International Journal of Colorectal Disease. 2014;29(12):1527–1534. PMID: 25331030
Mechanisms and GH Secretagogue Class Reviews
- Ishida J, Saitoh M, et al. Growth hormone secretagogues: history, mechanism of action, and clinical development. JCSM Rapid Communications. 2020. doi: 10.1002/rco2.9
- Venkova K, et al. Efficacy of ipamorelin, a novel ghrelin mimetic, in a rodent model of postoperative ileus. Journal of Pharmacology and Experimental Therapeutics. 2009;329(3):1110–1116. PMC4863553
Modified GRF(1-29) and CJC-1295 DAC Background
- Teichman SL, et al. Prolonged stimulation of GH and IGF-I by CJC-1295, a long-acting analog of GHRH, in healthy adults. Journal of Clinical Endocrinology & Metabolism. 2006;91(3):799–805. PMID: 16352683
- Ionescu M, Frohman LA. Pulsatile GH secretion persists during continuous stimulation by CJC-1295. JCEM. 2006;91(12). PMID: 17018654
- Wikipedia. Modified GRF (1-29). en.wikipedia.org/wiki/Modified_GRF_(1-29)
Regulatory Documents
- FDA PCAC Briefing Document: Ipamorelin-related bulk drug substances. October 29, 2024. fda.gov
- PCAC Meeting Minutes. October 29, 2024 — vote against ipamorelin for 503A bulks list. fda.gov
- Alliance for Pharmacy Compounding (A4PC). PCAC votes against four nominated bulk drug substances (ipamorelin among them). October/November 2024. a4pc.org
- Lexology / Reed Smith. FDA removes certain peptide bulk drug substances from Category 2 and sets PCAC review dates. October 1, 2024. Lexology
- WADA. Prohibited List — S2 Growth Hormone Secretagogues. wada-ama.org
Certificate of Analysis
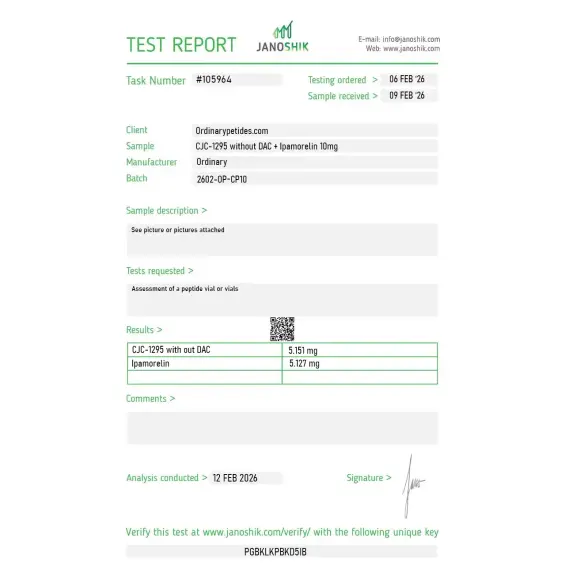
An independent test report is available for CJC-1295 without DAC / Ipamorelin. This report provides batch-level documentation and analytical verification information for research reference.

We chose the No-DAC pairing specifically because both components are short-acting — Mod GRF clearing in roughly half an hour, Ipamorelin similarly brief — which gives a pulsatile co-stimulation profile rather than the tonic exposure you'd get pairing Ipamorelin with the DAC version. That pulsatility matters for our protocol, and the listing was clear it was the No-DAC component. Sourcing the deliberately-pulsatile combination from one vial kept the design intent intact, and the material held both activities across the timecourse.
For a two-peptide formulation the documentation has to resolve the components and this one only half did — separate purity for each was there, but no chromatogram demonstrating the two peaks actually co-exist at the stated ratio in the same vial rather than being two numbers from two separate analyses stapled together. The blend performed in our somatotroph assays, but ratio integrity in the actual co-formulated vial is the thing I most want documented for any mixture. Four stars until the resolved-trace is standard.
The dual-receptor rationale is the actual research interest — Mod GRF hits the GHRH receptor while Ipamorelin hits the ghrelin receptor, two separate pathways converging on the somatotroph, and the co-formulation lets us study that convergence at a fixed ratio rather than reconstructing it from two stocks. For mapping whether the two receptor inputs sum or potentiate at the cell level, the pre-mixed form removes our own pipetting as a confound. Both receptor arms activated consistently in our parallel readouts.
No. These peptides are not FDA-approved medications and are supplied strictly for research purposes.
The No DAC version is shorter acting and supports pulse-based research designs, whereas DAC variants produce prolonged elevation. Choice depends on study objectives.
In research contexts, it is studied for controlled stimulation of growth hormone pathways without prolonged systemic exposure.
In experimental settings, CJC-1295 has been shown to stimulate growth hormone release via pituitary activation, particularly when combined with a GHRP such as Ipamorelin.
It is an unofficial combination of two GH-axis secretagogues: a GHRH analogue and a ghrelin receptor agonist. It is usually marketed as a stack for stimulating endogenous GH.
A strong human evidence base specifically for the duo is not clearly visible. There are data on the individual components, but not convincing clinical evidence on the combination itself.
It lacks the drug affinity complex. FDA explicitly states that DAC and non-DAC forms are not interchangeable.
Yes. There is an early human PK/PD study in healthy volunteers and a clinical program in postoperative ileus. But that is not the same thing as proven benefit for body composition or anti-aging.
No. At the current level of evidence, that would be too strong a claim.
No. Both CJC-1295 and ipamorelin are prohibited by WADA.
The key point is this: the duet has a plausible mechanism, but not a comparably strong clinical evidence base to justify the confidence with which it is marketed.
Ipamorelin is a synthetic pentapeptide — five amino acids — and a selective growth hormone secretagogue (GHS). It belongs to a class of compounds called growth hormone-releasing peptides (GHRPs) and mimics ghrelin, the "hunger hormone," by binding to the ghrelin receptor (also called the GHS-R1a receptor) in the pituitary and hypothalamus. It was developed specifically to stimulate GH release with high selectivity — meaning it does not significantly stimulate cortisol, prolactin, acetylcholine, or aldosterone, unlike earlier GHRPs such as GHRP-2 and GHRP-6. This selectivity makes it one of the cleanest and best-tolerated GH-releasing peptides available.
The two peptides activate GH release through completely different and complementary receptor pathways. CJC-1295 No DAC activates GHRH receptors on pituitary somatotropes — it is the accelerator that primes GH production and releases the accumulated stored GH. Ipamorelin activates ghrelin receptors — it is the trigger that actually fires the release mechanism. In normal physiology, the body uses both pathways simultaneously to generate each GH pulse. When both receptors are activated at the same time with exogenous peptides, the resulting GH pulse is significantly larger — typically 2 to 10 times greater — than what either compound produces alone. This is genuine synergy, not simple addition, because the two signals converge on the same final output through independent upstream mechanisms. The short half-lives of both compounds — approximately 30 minutes each — mean the GH pulse is sharp, physiological in its timing, and clears quickly without desensitizing the system.
Both peptides are injected simultaneously — typically in the same syringe drawn from separate vials — once, twice, or three times daily depending on the protocol. The injection triggers a coordinated dual-pathway GH pulse within minutes. The GH enters circulation, travels to the liver, and stimulates IGF-1 production. Because both peptides clear rapidly, the pulse-and-rest rhythm is preserved — GH rises sharply and then returns toward baseline before the next injection. This pattern closely mimics the natural GH secretion rhythm, particularly the large pulse that occurs during slow-wave sleep.
Reported and researched benefits include improved body composition through increased lean muscle mass and accelerated fat loss particularly visceral fat, significantly improved deep sleep quality and duration — users frequently report this as one of the first and most noticeable effects — faster recovery from exercise, injury, and surgery, increased energy and vitality, improved skin quality and elasticity through collagen stimulation, enhanced bone density support, and general anti-aging effects associated with optimized GH and IGF-1 levels. The combination is also used by some physicians as a more physiologically appropriate alternative to direct HGH injections, as it stimulates endogenous production rather than suppressing the body's own output.
Both peptides are given by subcutaneous injection simultaneously. Standard protocols use 100 to 300 mcg of each peptide per injection, once to three times daily. Timing is important — injections should be on an empty stomach ideally 2 hours after eating and at least 30 minutes before the next meal, as insulin blunts GH secretion. Bedtime injection is particularly recommended to amplify the natural GH surge during sleep. Both compounds are supplied as lyophilized powders reconstituted with bacteriostatic water and can be drawn into the same syringe for a single injection. Cycling is generally recommended — common protocols use 5 days on and 2 days off, or longer cycles of 3 to 6 months followed by a break.
The combination is considered one of the most well-tolerated in the peptide GH-secretagogue space. Ipamorelin's high selectivity means it does not cause the increased hunger, cortisol elevation, or prolactin rises seen with older GHRPs. Commonly reported side effects for the combination include mild water retention, temporary flushing immediately after injection, tingling or numbness in the hands or feet particularly at night, mild headache, and injection site redness. Increased appetite can occur at higher doses. Because both peptides clear within 30 minutes, any side effects are short-lived and resolve quickly. The risk of receptor desensitization is lower than with the DAC version of CJC-1295 due to the preserved pulsatile pattern.
The same contraindications as individual GH secretagogues apply to the stack. People with active cancer or a history of cancer should not use it — elevated IGF-1 is an established promoter of cell growth and its role in cancer biology is well documented. Those with diabetes or significant insulin resistance should exercise caution as GH elevation can worsen glucose control. People with pituitary disorders, acromegaly, or suspected pituitary tumors should avoid it. Pregnant or breastfeeding women should not use it. Competitive athletes subject to WADA testing should note that both peptides are prohibited and detectable. Neither peptide is FDA-approved and neither can be legally compounded in the United States, meaning any product obtained outside a clinical setting carries unverified purity risks.





