






Sermorelin Acetate
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Sermorelin Acetate: A Short GHRH Peptide With a Long History and a Very Limited Modern Interpretation
Sermorelin acetate is a synthetic analog of GHRH(1-29)-NH2 — a short active fragment of growth hormone–releasing hormone, which in the research context was used as a way to observe how the pituitary responds to stimulation of its own GH–IGF-1 axis. In early clinical and physiological observations, it produced a rapid GH response when pituitary function was preserved, and in historical pediatric scenarios it was studied as part of a narrow endocrine model of growth.
The real interest here is not in "ready-made magic," but in a careful tool for those who care about the logic of regulation itself rather than loud promises. In the published data around sermorelin, what is especially compelling is its role as the minimal active sequence of GHRH — a small peptide with quite a large scientific idea behind it.
Why It Is Worth a Closer Look
If what interests you is not myths about anti-aging, but the research context of GH secretagogues, sermorelin is exactly the kind of case that invites a closer look. It does not shout, but rather calmly says: "let's figure out how this actually works."
Sermorelin Acetate: A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Sermorelin occupies an unusual position in the GH peptide landscape: it has more regulatory legitimacy than almost any other compound in the community performance and anti-aging market, and yet its evidence base for the applications people actually use it for — adult GH optimisation, body composition, anti-aging — is thin, old, and methodologically limited.
The regulatory legitimacy is real. Sermorelin received FDA approval in 1990 (diagnostic use) and 1997 (paediatric treatment).[1][2] When its manufacturer discontinued it in 2008, the FDA explicitly confirmed the withdrawal was not for safety or efficacy reasons — a statement that allows compounding pharmacies to continue preparing it legally.[4] No comparable statement covers most other peptides in this series. The mechanism is also physiologically coherent: as a GHRH receptor agonist, sermorelin stimulates the pituitary to release GH in a pulsatile, somatostatin-regulated manner that respects the body’s feedback architecture.
The evidence limitation is equally real. The adult data is primarily from small studies conducted in the 1990s, measuring intermediate endpoints (IGF-1, lean body mass, sleep quality) in modest sample sizes. No large randomised controlled trials have evaluated sermorelin for adult GHD, age-related GH decline, or body composition. Tesamorelin — a related GHRH analogue with modern Phase 3 trial data and an approved indication — is the pharmacologically more robust reference point in the GHRH class.
| At a glance | |
|---|---|
| Full name | Sermorelin acetate; also: GHRH(1-29), GRF 1-29 |
| Brand name | Geref (Geref Diagnostic, Geref Pediatric) — discontinued 2008 |
| Sequence | First 29 amino acids of human GHRH(1-44) |
| Molecular weight | ~3,357 Da |
| Mechanism | GHRH receptor (GHRHR) agonist → pituitary somatotroph GH secretion |
| Half-life | 11–12 minutes (SC or IV) |
| FDA approval history | Approved 1990 (diagnostic) and 1997 (paediatric GHD); voluntarily withdrawn 2008 (commercial reasons only) |
| FDA statement | ✅ “Not withdrawn for reasons of safety or effectiveness” (2013) |
| Current status | Compounded off-label by licensed pharmacies with valid prescription; not a controlled substance |
| WADA | ❌ Prohibited — S2 (Growth Hormone Secretagogues) |
The GH Axis: Context for Understanding Sermorelin
The hypothalamus secretes GHRH in pulses — classically during sleep, fasting, and in response to exercise and stress. GHRH travels via the hypophyseal portal system to the anterior pituitary, where it binds to GHRH receptors (GHRHR) on somatotroph cells, triggering cAMP → PKA activation → pulsatile GH secretion. The counter-regulatory hormone somatostatin (SRIF) inhibits GH release. The interplay between GHRH pulses and somatostatin withdrawal creates the characteristic pulsatile pattern of GH secretion: large pulses at night during deep sleep, smaller pulses during the day. GH acts on the liver and peripheral tissues to produce IGF-1, which feeds back negatively to suppress both GHRH and pituitary GH secretion.
GHRH secretion from the hypothalamus declines progressively with age — the primary driver of the age-related fall in GH levels. GH secretion peaks in adolescence and declines approximately 14% per decade thereafter. The pituitary somatotrophs themselves retain secretory capacity; they receive less GHRH stimulation. This distinguishes age-related GH decline (somatopause) from organic adult-onset GHD, where the pituitary or hypothalamus has structural damage. Sermorelin’s pharmacological rationale in aging rests on this distinction: because the pituitary retains functional capacity, providing exogenous GHRH-like stimulation can restore GH pulsatility and partially reverse the somatopause decline.
Structure: The Minimal Active Fragment
Human GHRH is a 44-amino acid peptide. Studies in the 1980s established that the N-terminal 29 amino acids (GHRH(1-29)) retain full biological activity at the GHRH receptor — the C-terminal residues contribute little to receptor binding or GH-secretory potency. Sermorelin is this N-terminal 29-amino acid fragment: Tyr-Ala-Asp-Ala-Ile-Phe-Thr-Asn-Ser-Tyr-Arg-Lys-Val-Leu-Gly-Gln-Leu-Ser-Ala-Arg-Lys-Leu-Leu-Gln-Asp-Ile-Met-Ser-Arg-NH&sub2;. The C-terminal amidation (–NH&sub2;) is required for full biological activity; the N-terminal tyrosine is essential for receptor binding.
Pharmacokinetics
After subcutaneous administration, peak concentrations are reached in 5–20 minutes, with sermorelin rapidly cleared from the circulation. The half-life is 11–12 minutes after either intravenous or subcutaneous administration. This very short half-life means sermorelin needs to be timed to coincide with the natural GHRH pulse — typically a bedtime injection, when the first major nocturnal GH pulse occurs. The brief stimulation mirrors natural pulsatility — brief GHRH receptor activation → GH pulse → somatostatin feedback → GH pulse subsides — unlike rhGH injection, which produces a sustained plateau of GH exposure.
Compared to tesamorelin (the related FDA-approved GHRH analogue): tesamorelin has a modified N-terminal trans-3-hexenoic acid group that increases its half-life to approximately 26 minutes and confers greater plasma stability, contributing to more potent and reproducible clinical effects.[9]
Mechanism of Action
Sermorelin binds to GHRHR on anterior pituitary somatotrophs, coupling to Gαs → adenylyl cyclase → cAMP → PKA → voltage-gated calcium channel activation → GH vesicle exocytosis. Sermorelin specifically stimulates GH secretion from the pituitary gland without any significant change in prolactin, LH, FSH, insulin, cortisol, glucose, or glucagon.[5]
The somatostatin regulation advantage
Sermorelin’s effects are regulated by negative feedback through somatostatin, making it very difficult to achieve supraphysiological GH levels — unlike exogenous rhGH, where the GH level is determined entirely by the dose administered. This self-limiting mechanism means sermorelin promotes GH release in bursts that mirror natural hormone rhythms rather than the constant levels produced by rhGH injections, and avoids tachyphylaxis by maintaining physiological pulsatility.[5]
Pituitary reserve
Sermorelin is claimed to stimulate pituitary gene transcription of GH messenger RNA, increasing pituitary reserve and thereby preserving more of the growth hormone neuroendocrine axis. In contrast, chronic high-dose rhGH suppresses endogenous GH production through negative feedback, potentially reducing pituitary reserve over time. The clinical significance of this distinction in adults has not been formally validated in controlled trials.
Key difference from GHRPs
Sermorelin acts on GHRHR — the same receptor as endogenous GHRH. Growth hormone-releasing peptides (GHRPs) such as ipamorelin, GHRP-2, and GHRP-6 act on the ghrelin receptor (GHS-R1a) — a completely different mechanism. The two classes are synergistic: GHRH (via sermorelin) sets the stage for GH release, while GHRPs amplify the pulse via ghrelin receptor activation. Combined GHRH + GHRP produces greater GH release than either alone — GHRP-2 led to a 47-fold increase in pulsatile GH secretion, GHRH alone to a 20-fold increase, and the combination to a 54-fold increase compared to controls.[11]
Regulatory History
The FDA approved sermorelin injection 0.05 mg/amp in December 1990 for diagnostic evaluation of pituitary GH secretory capacity (NDA 19-863).[1] In September 1997, NDA 20-443 approved Geref for the treatment of idiopathic GHD in children with growth failure — the first GHRH analogue approved for therapeutic use in paediatric GHD.[2] EMD Serono notified the FDA on December 2, 2008 of their intention to stop manufacturing Geref; the withdrawal was for commercial reasons.[3] In 2013, the FDA specifically confirmed under §314.161 that Geref was not withdrawn for safety or effectiveness reasons — a legally significant determination that permits compounding pharmacies to continue preparing sermorelin under 503A provisions.[4]
Evidence: What Do We Actually Know?
Paediatric GHD (the established evidence)
The clinical trials supporting the 1997 FDA approval established that sermorelin significantly increases GH secretion in GH-deficient children, improves growth velocity, and is well-tolerated with injection site reactions as the primary adverse event. This evidence is solid within its indication but is not directly extrapolatable to adult use — paediatric GHD is a different clinical entity from age-related somatopause.
Adult GHD and somatopause (limited evidence)
The adult evidence is primarily from small studies conducted in the 1990s. Corpas et al. (1992–1993) demonstrated that short-term subcutaneous sermorelin injections in healthy elderly men reversed age-related decreases in GH and IGF-1 — confirming that the aged pituitary does respond to GHRH stimulation. A small single-blind RCT by Vitiello et al. (1997) in elderly male and female subjects given nightly subcutaneous sermorelin for 16 weeks reported increased skin thickness, significant increases in lean body mass in males (mean +1.26 kg), and improvements in libido and wellbeing. Positive effects on sleep quality and cognitive markers were also reported in separate Vitiello studies, consistent with the known role of GH/IGF-1 in slow-wave sleep regulation.[6]
The most-cited adult rationale paper (Walker, Clinical Interventions in Aging, 2006) is a review, not primary trial data.[5] The aggregate adult picture: sermorelin raises GH and IGF-1 in older adults, produces modest improvements in lean mass and some quality-of-life metrics, and is well-tolerated. The studies are too small, too short, and too old to support contemporary regulatory approval for adult indications.
Comparison: Tesamorelin evidence (the modern benchmark)
Tesamorelin — a GHRH(1-44) analogue with a trans-3-hexenoic acid N-terminal modification — has undergone rigorous Phase 3 trials and received FDA approval in 2010 for HIV-associated lipodystrophy (Egrifta). Its visceral fat reduction evidence (15–20% VAT reduction at 26 weeks vs. placebo, in trials of approximately 400 patients per arm) is the most robust GHRH class data available for adult body composition endpoints. Sermorelin has no equivalent Phase 3 body composition trials. The two compounds share a mechanism (GHRHR agonism) but tesamorelin is pharmacologically more potent and has far stronger clinical evidence for the body composition endpoints that are the primary claimed benefit of both compounds in adult practice.[9]
Clinical Evidence Summary
| Endpoint | Population | Key evidence | Quality |
|---|---|---|---|
| GH stimulation (diagnostic) | Paediatric GHD | Multiple studies; FDA approval basis [1] | Strong for indication |
| Growth velocity improvement | Paediatric GHD | Clinical trial basis for 1997 approval [2] | Moderate-strong |
| IGF-1 elevation in elderly | Healthy elderly adults | Small RCTs, 1992–1997 | Weak-moderate |
| Lean body mass increase | Elderly males | Small RCT (N<50), 16 weeks | Weak |
| Sleep quality improvement | Elderly adults | Small observational/RCT data | Weak |
| Fat mass reduction | Adults | No adequately powered RCT | No data |
| Cardiovascular endpoints | Any population | No data | No data |
How Sermorelin Differs from Exogenous rhGH
| Feature | Sermorelin | Recombinant human GH (rhGH) |
|---|---|---|
| What is administered | GHRH analogue (stimulates pituitary) | GH itself (bypasses pituitary) |
| GH release pattern | Pulsatile (physiological) | Non-pulsatile sustained plateau |
| Somatostatin regulation | ✅ Preserved; limits supraphysiological GH | Bypassed; dose determines GH level |
| Supraphysiological GH risk | Very low (somatostatin feedback) | Real at higher doses |
| Pituitary reserve | Maintained or enhanced | May suppress with long-term use |
| Legal restrictions (US) | Not a controlled substance | Controlled; restricted to GHD, wasting states |
| Evidence base for adults | Limited small studies | Extensive; large trials for GHD indication |
| WADA prohibited | ❌ Yes (S2) | ❌ Yes (S2) |
Safety Profile
Sermorelin’s safety in paediatric GHD treatment over years of clinical use established a favourable profile: the most common adverse events are injection site reactions (redness, swelling, pain) — mild and transient. Flushing, headache, and nausea are occasionally reported. No significant effects on prolactin, LH, FSH, insulin, cortisol, or glucose at therapeutic doses have been documented.
⚠️ Cancer concern: Because GH and IGF-1 are mitogenic, all GH-related therapies carry a theoretical concern about acceleration of pre-existing occult malignancies. Sermorelin is contraindicated in patients with active or suspected malignancy. Long-term IGF-1 monitoring is recommended to ensure levels remain within age-appropriate normal ranges. Sermorelin, by working through somatostatin feedback, is much less likely than high-dose rhGH to produce supraphysiological IGF-1 levels — one of its primary safety advantages over direct GH administration.
Long-term safety data for sermorelin in adults is genuinely limited. The existing trials are short (weeks to months), small, and not designed to detect low-frequency adverse events. No large pharmacovigilance database exists for sermorelin comparable to the SAGhE study for rhGH.
Common Misconceptions
“Sermorelin is FDA-approved and therefore proven safe and effective for anti-aging.”
Sermorelin’s FDA approval was for paediatric GHD only — it was never approved for adult GHD or anti-aging. The FDA-approved product (Geref) no longer exists. Current compounded sermorelin is not FDA-approved. The FDA’s statement that withdrawal was not for safety reasons permits legal compounding but does not constitute approval for adult indications.
“Because sermorelin works through the body’s own pituitary, it has no risks.”
Working through the pituitary’s natural GH-secretion machinery modulates risk but does not eliminate it. Cancer risk, injection-related risks, and the risk of elevating IGF-1 beyond age-appropriate levels remain. “Natural mechanism” is not synonymous with “risk-free.”
“Sermorelin won’t show on drug tests.”
⚠️ Sermorelin is prohibited by WADA under S2 and is detectable by mass spectrometric methods used in anti-doping programmes. Assuming it is undetectable because it stimulates endogenous GH rather than supplying exogenous GH is incorrect — the peptide itself is detectable in urine and blood.
Frequently Asked Questions
How does sermorelin relate to CJC-1295?
CJC-1295 (Mod GRF 1-29) is a modified version of sermorelin with amino acid substitutions at positions 2, 8, 15, and 27 designed to increase proteolytic stability, producing a longer effective action than sermorelin (hours versus minutes). CJC-1295 with DAC binds to albumin and has a half-life measured in days. CJC-1295 is a distinct peptide from sermorelin without FDA approval history; it is covered separately in this series.
Why is tesamorelin preferred by many clinicians over sermorelin?
Tesamorelin is FDA-approved (Egrifta), has Phase 3 trial data for visceral fat reduction, is manufactured under pharmaceutical quality controls, and has a longer half-life producing more reproducible plasma exposure. For body composition goals in adults, tesamorelin’s clinical data is substantially stronger.[9] Sermorelin’s advantages are lower cost through compounding and a longer clinical history from paediatric use.
What is somatopause and how does it relate to sermorelin?
Somatopause is the age-related decline in GH secretion driven by hypothalamic GHRH decline. Because the pituitary retains functional capacity in healthy aging, GHRH stimulation with sermorelin can partially restore GH pulsatility — different from organic GHD where the pituitary or hypothalamus has structural damage. Sermorelin’s theoretical utility is greatest in somatopause, where the pituitary is ready to respond but receives insufficient stimulation. However, the evidence that this restoration produces clinically meaningful health benefits in otherwise healthy adults has not been established in large trials.
Key Takeaways
- ✅ Sermorelin has more regulatory legitimacy than almost any other compound in the community GH peptide market. It was FDA-approved for paediatric GHD from 1997 to 2008. The FDA explicitly confirmed the withdrawal was not for safety or efficacy reasons — a history that distinguishes sermorelin from compounds that have never been through regulatory review.[4]
- ⚠️ The evidence for adult use is weak. Small studies from the 1990s show GH and IGF-1 elevation in older adults with some modest body composition improvements. No Phase 3 trials have been conducted for adult GHD, somatopause, anti-aging, or body composition. The physiological rationale is coherent, but rationale is not evidence.
- ✅ The somatostatin-feedback physiological advantage over rhGH is real. Sermorelin’s self-limiting regulatory mechanism genuinely distinguishes it from exogenous GH in terms of supraphysiological exposure risk. The pharmacology is sound, though clinical superiority in adults has not been formally established.
- Tesamorelin is the pharmacologically superior GHRH analogue with better evidence. FDA-approved, Phase 3 trial data, pharmaceutical manufacturing — tesamorelin (Egrifta) is the better-evidenced option. Sermorelin’s advantage is lower cost and accessibility via compounding.[9]
- ⚠️ WADA prohibition is absolute. Sermorelin is prohibited in-competition and out-of-competition under S2. The peptide itself is detectable by mass spectrometry.
- Compounded sermorelin quality is not guaranteed. Compounding pharmacies produce sermorelin without FDA oversight of safety, efficacy, or quality. Working with reputable, licensed facilities and insisting on certificates of analysis is the minimum standard.
References
FDA Regulatory History
- FDA approval NDA 19-863: sermorelin acetate injection 0.05 mg/amp. December 1990. (Diagnostic use)
- FDA approval NDA 20-443: Geref (sermorelin acetate injection) 0.5 and 1.0 mg/vial. September 26, 1997.
- FDA Federal Register notice: Geref (sermorelin acetate) NDAs 19-863 and 20-443 withdrawn. May 19, 2009; effective June 18, 2009.
- FDA determination under §314.161: “Geref (sermorelin acetate) was not withdrawn for reasons of safety or effectiveness.” Published 2013.
Key Science
- Walker RF. Sermorelin: a better approach to management of adult-onset growth hormone insufficiency? Clinical Interventions in Aging. 2006;1(4):307–308. PMC2699646
- Corpas E, Harman SM, Blackman MR. Human growth hormone and human aging. Endocrine Reviews. 1993;14(1):20–39.
- Sigalos JT, Pastuszak AW. Beyond the androgen receptor: the role of growth hormone secretagogues in the modern management of body composition in hypogonadal males. World Journal of Urology. 2020. PMC7108996
- Ishida J, et al. Growth hormone secretagogues: history, mechanism of action, and clinical development. JCSM Rapid Communications. 2020. doi: 10.1002/rco2.9
Comparison: Tesamorelin
- Falutz J, Allas S, Blot K, et al. Metabolic effects of a growth hormone–releasing factor in patients with HIV. New England Journal of Medicine. 2007;357(23):2359–2370.
- FDA NDA 022505: tesamorelin acetate (Egrifta) approval documents. 2010.
GH Secretagogue Context
- Cook DM, et al. The safety and efficacy of growth hormone secretagogues. Current Drug Safety. 2007. PMC5632578
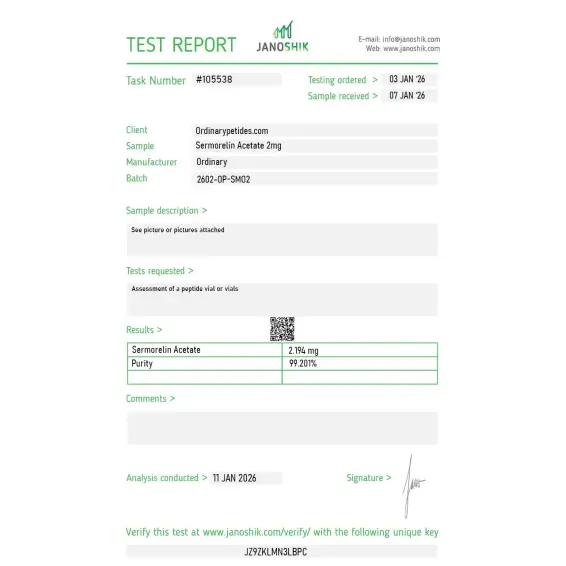
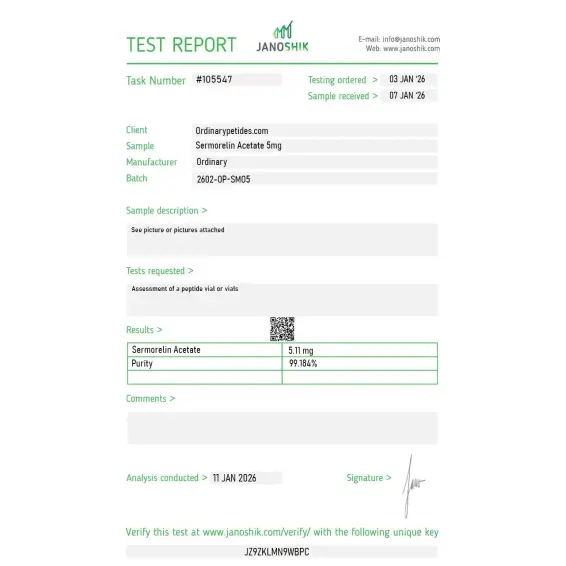
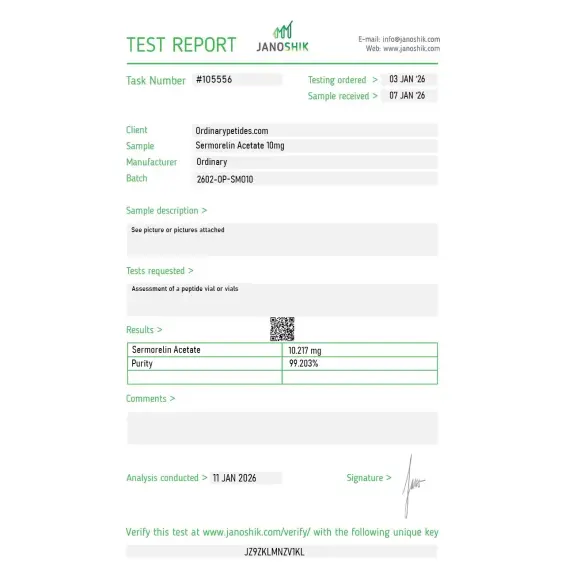
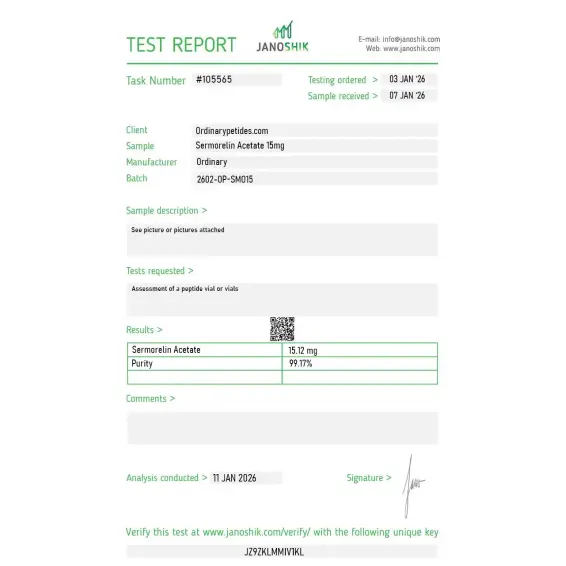
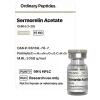
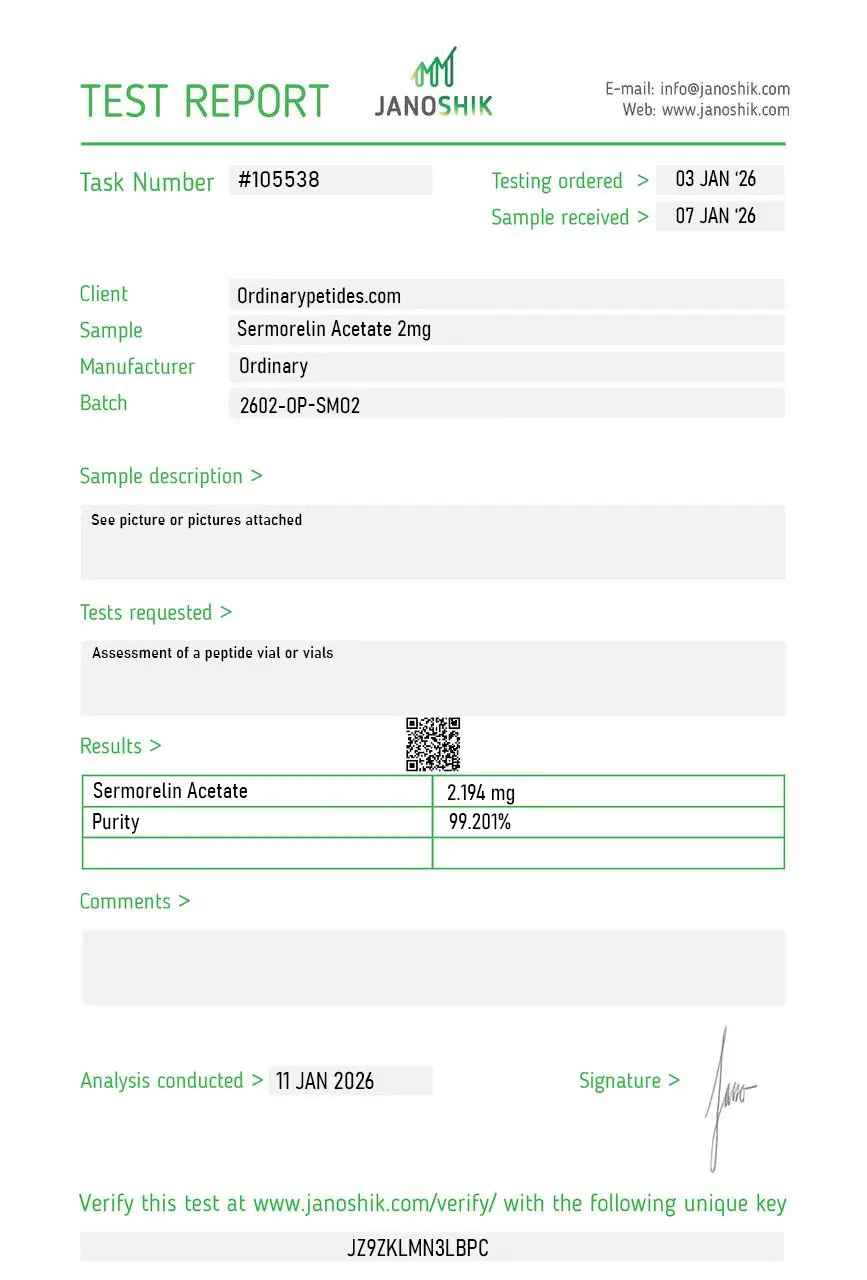
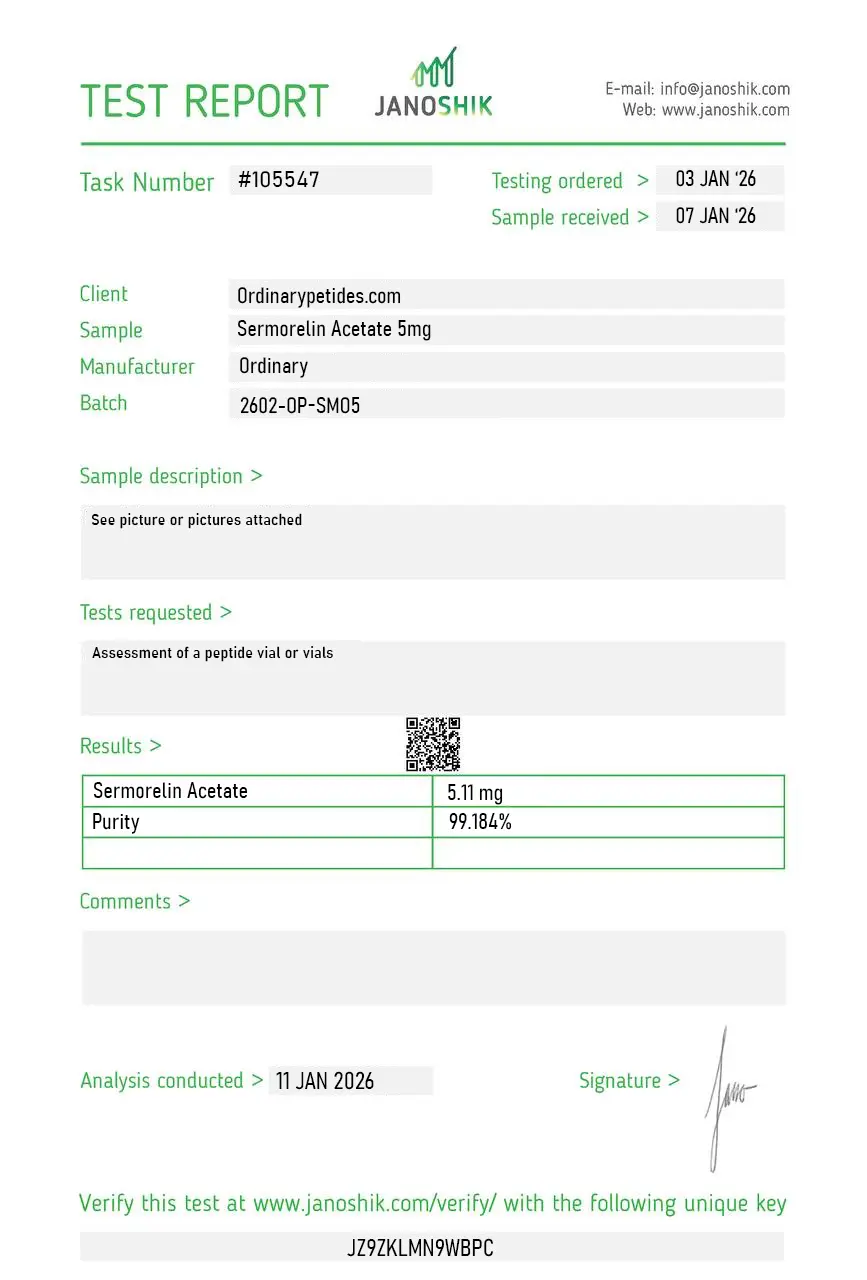
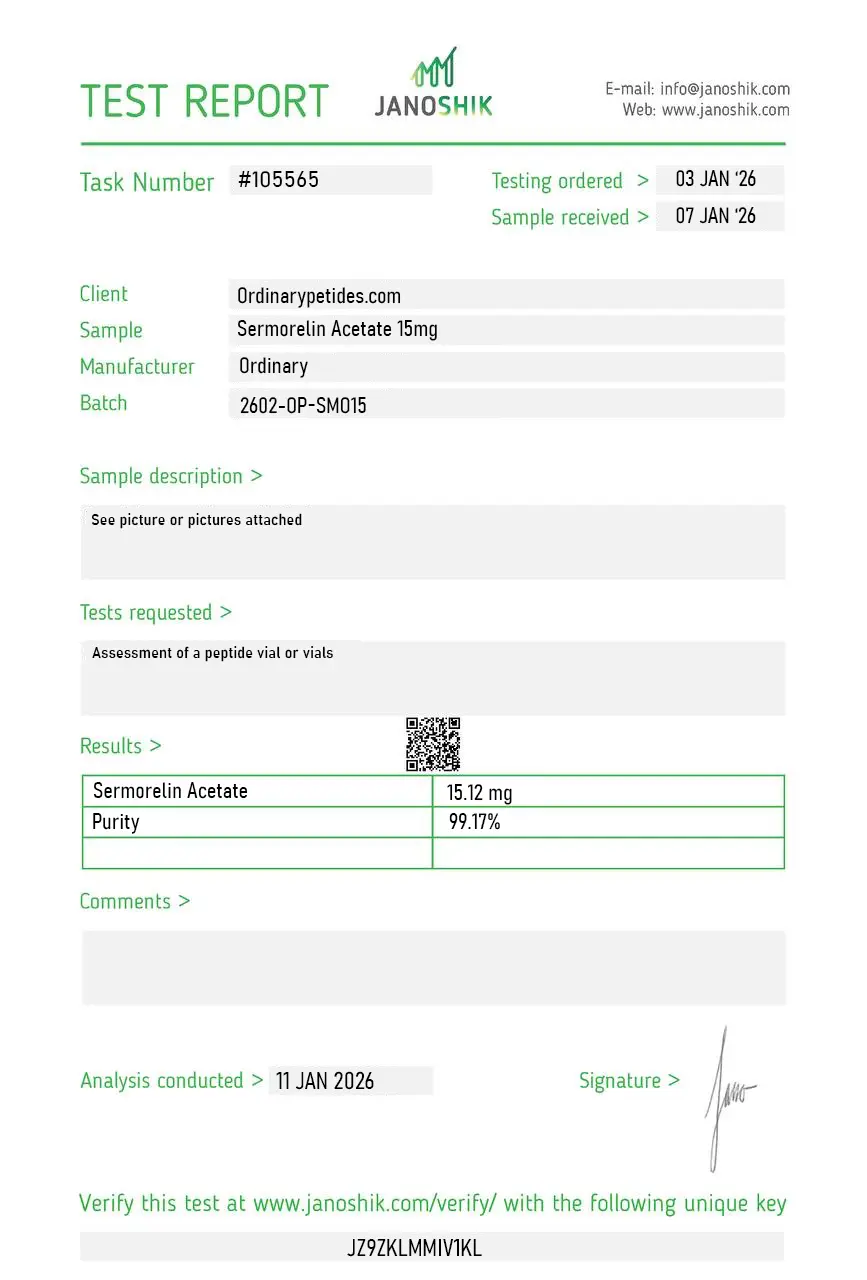
Certificate of Analysis
Independent test reports are available for Sermorelin Acetate 2mg, 5mg, 10mg, and 15mg. These reports provide batch-level documentation and analytical verification information for research reference.
Based on 2 reviews
5.0
Ordered the acetate form specifically because the prior batch elsewhere came as a TFA salt that left us with anomalously high background in our peptide bioactivity readouts — TFA at residual levels has its own cellular effects that masquerade as compound effects. Switching to a properly acetate-exchanged sermorelin cleaned that up. The salt form question is invisible until it isn't, and this material was the exchange we needed.
The honest pricing on this is part of why I keep ordering — sermorelin is one of the older compounds in this category and the pricing reflects that maturity, where newer or scarcer GHRH analogs carry premium markups that aren't always justified by superior characterization. Sermorelin gets you authentic native GHRH(1-29) at a price point that makes routine receptor work affordable. The material has been consistent batch-over-batch within the working window we've used it.
No. It is an analog of GHRH(1-29)-NH2 that stimulates the release of endogenous GH from the pituitary.
Yes. Historically, the FDA approved Geref Diagnostic and Geref Pediatric, both based on sermorelin acetate. These products were later withdrawn and are no longer manufactured or sold.
Based on the available data, there are no grounds to consider it a modern standard treatment for adult conditions related to age-related decline, wellness, or "rejuvenation.
Historically yes, but only in a limited subgroup of pediatric idiopathic GHD, and that history is not equal to a current broad standard of therapy.
Somatropin is GH itself, while sermorelin is a stimulator of its endogenous release. If the pituitary does not respond, sermorelin will not work the way somatropin does.
There is no convincing modern clinical base for such a claim. There are only limited studies in the GHRH-analog direction and physiological signals.
Sermorelin acetate is a synthetic 29-amino acid peptide corresponding to the first 29 amino acids of the naturally occurring 44-amino acid growth hormone-releasing hormone (GHRH). It is the shortest fully functional fragment of GHRH that retains complete biological activity at GHRH receptors — stimulating the pituitary gland to produce and release growth hormone through the same physiological pathway as endogenous GHRH. It was developed initially as a diagnostic tool for assessing GH deficiency and was FDA-approved under the brand name Geref for both diagnostic use and therapeutic treatment of idiopathic GH deficiency in children. It is one of the most established GH secretagogues in this entire series — having been in clinical use and studied in humans far longer than CJC-1295, Ipamorelin, or any of the GHRPs. The pharmaceutical-grade Geref product was voluntarily withdrawn from the US market in 2008 for commercial reasons, not safety concerns, but compounded sermorelin has remained widely available through licensed compounding pharmacies and its regulatory status differs significantly from Category 2 peptides like CJC-1295.
Sermorelin binds to and activates GHRH receptors on somatotrope cells in the anterior pituitary gland — the same receptor that CJC-1295, Mod GRF 1-29, and Tesamorelin act upon. This binding triggers adenylyl cyclase activation, cAMP elevation, and ultimately the synthesis and pulsatile release of growth hormone from stored GH pools. Because sermorelin works upstream — stimulating the body's own pituitary to produce GH — it preserves the natural feedback loops of the hypothalamic-pituitary axis. The pituitary's somatostatin-mediated feedback mechanism remains intact, meaning the body can still regulate and limit GH output. This distinguishes it fundamentally from direct exogenous HGH administration, which bypasses these feedback mechanisms entirely and suppresses endogenous GH production. Sermorelin's shorter half-life of approximately 10 to 20 minutes produces a more physiological GH pulse pattern compared to the longer-acting CJC-1295 DAC.
Sermorelin's original FDA approval was for diagnosis and treatment of GH deficiency in children — a well-established pediatric indication. Beyond this, it has been studied and used clinically in adults for GH deficiency, age-related GH decline, body composition improvement, sleep quality enhancement, and general wellness optimization. Published human trials document significant increases in GH and IGF-1 levels after sermorelin administration, improved sleep architecture through enhanced slow-wave sleep, improvements in lean body mass and reductions in fat mass in GH-deficient adults, and generally favorable tolerability over extended use periods. The evidence base for sermorelin in healthy adults for optimization purposes — as opposed to diagnosed GH deficiency — is less robust than its pediatric deficiency indication but substantially better than most research peptides in this series.
Sermorelin is given by subcutaneous injection, typically once daily at bedtime — the bedtime timing capitalizes on the natural nocturnal GH surge during deep sleep and maximizes the additive effect of sermorelin on this physiological rhythm. Standard therapeutic doses range from 0.2 mg to 0.3 mg per injection, though some protocols use divided twice-daily dosing. Like all GHRH analogs it should be administered on an empty stomach as food-induced insulin elevation blunts GH release. It is commonly combined with a GHRP such as Ipamorelin — producing dual-pathway GH stimulation through GHRH receptor and ghrelin receptor activation simultaneously — though Ipamorelin itself cannot be legally compounded in the United States. Sermorelin is supplied as lyophilized powder reconstituted with sterile diluent. Unlike CJC-1295, Ipamorelin, and most other GH peptides in this series, sermorelin can be legally compounded by licensed US compounding pharmacies as it is not designated Category 2.
Sermorelin has one of the most favorable and well-characterized safety profiles of any GH-axis peptide, consistent with its long clinical history. The most commonly reported side effects are mild injection site reactions including redness, swelling, and brief discomfort — particularly relevant given its daily injection schedule. Flushing, headache, and dizziness are reported in some users. Mild water retention and joint discomfort are documented at higher doses, consistent with elevated IGF-1 effects seen across the GH-secretagogue class. Notably it does not produce the cortisol, prolactin, or ACTH elevations associated with GHRPs like GHRP-2 and GHRP-6, and does not meaningfully stimulate appetite. The same long-term theoretical concerns applicable to sustained GH and IGF-1 elevation — insulin resistance, potential effects on cell growth — apply, but sermorelin's pituitary-regulated ceiling on GH output provides an inherent safety advantage over direct HGH administration.
This is one of sermorelin's most important practical distinguishing features in the US market. The original pharmaceutical product Geref was voluntarily withdrawn for commercial rather than safety reasons. Sermorelin is not on the FDA's Category 2 bulk drug substances list — the list that prohibits compounding of BPC-157, CJC-1295, Ipamorelin, and many other peptides in this series. It can therefore be legally compounded by licensed US compounding pharmacies and prescribed by physicians for appropriate indications. This makes it one of the few GH-axis peptides genuinely accessible through legitimate US medical channels rather than only through gray-market research vendors. It is banned by WADA under the Peptide Hormones, Growth Factors, and Related Substances category.
People with active cancer or a history of cancer should not use it given IGF-1's established mitogenic role. Those with pituitary tumors or hypothalamic disorders should be evaluated carefully as sermorelin requires intact pituitary function to produce its effect. People with diabetes or significant insulin resistance should be monitored as GH elevation can worsen glucose metabolism. Pregnant or breastfeeding women should not use it. Children using it for therapeutic GH deficiency should have bone age monitoring as in any GH-stimulating therapy to avoid premature epiphyseal closure. Competitive athletes are prohibited from use under WADA.





