








HGH
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
HGH: A Powerful Hormonal Tool With a Specific Medical Role — Not a Universal Youth Injection
HGH is not a "magic youth injection," but a genuine peptide hormone with a very specific medical role. In the clinical context, it has been studied most thoroughly in settings where there is a confirmed growth hormone deficiency in adults and children, as well as in certain officially recognized growth-related conditions. In the published data, it is precisely in these scenarios that HGH is associated with effects on growth, body composition, and certain functional parameters — not with some universal "upgrade" for just anyone.
Its loud reputation in anti-aging, weight loss, and muscle gain extends much further than the actual evidence base. That is exactly what makes HGH interesting — not as lifestyle hype, but as a powerful hormonal tool that works only in the right diagnosis and under proper supervision.
And yes, this is one of those cases where "powerful" does not mean "appropriate for everyone."
Human Growth Hormone (HGH / Somatropin): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Human growth hormone (HGH), in its pharmaceutical form called somatropin, is unlike most compounds in this article series: it is not experimental, it is not a research chemical, and it is not awaiting clinical validation. It is a fully characterised, FDA-approved, extensively regulated biologic with a decades-long track record in specific medical indications — primarily paediatric growth hormone deficiency (GHD), adult GHD, and several other well-defined conditions.
Understanding HGH requires holding three distinct frames simultaneously. In genuine GHD, it works: for children with documented GHD, somatropin produces 8–12 cm additional final adult height; for adults with documented GHD, it improves body composition, quality of life, bone mineral density, and metabolic parameters. In healthy adults, the body composition effects are real but the clinical significance is doubtful: HGH raises lean body mass by ~2 kg and reduces fat mass by a comparable amount — confirmed across multiple controlled trials — but it does not improve muscle strength, physical function, exercise capacity, or quality of life at meaningful clinical levels.[6] The longevity biology is counterintuitive and sobering: GH-resistant mice live dramatically longer; centenarians frequently have lower IGF-1 levels; human Laron syndrome (GH resistance) is associated with remarkably low rates of cancer and diabetes. These findings fundamentally challenge the premise that more GH equals longer, healthier life.[8]
| At a glance | |
|---|---|
| INN (pharmaceutical name) | Somatropin |
| Structure | Single-chain polypeptide, 191 amino acids, ~22 kDa; identical to endogenous pituitary GH; 2 disulfide bridges; no sugar residues |
| Production | Recombinant DNA technology (E. coli or mammalian cell culture, depending on formulation) |
| Key endogenous functions | Childhood growth; adult body composition; metabolism; IGF-1 stimulation |
| Primary signalling | GH receptor → JAK2 → STAT5b; also indirect via hepatic IGF-1 |
| Half-life | ~2–4 hours (subcutaneous injection) |
| FDA-approved indications | Paediatric GHD, adult GHD, Turner syndrome, Prader-Willi, SGA, CKD-related growth failure, SHOX deficiency, short bowel syndrome (Zorbtive), HIV/AIDS wasting (Serostim) |
| Key brands | Norditropin (Novo Nordisk), Humatrope (Eli Lilly), Genotropin (Pfizer), Omnitrope (Sandoz), Saizen, Zomacton, Skytrofa (once-weekly), Sogroya (once-weekly) |
| Anti-aging use | ⚠️ Explicitly illegal in US; no long-term efficacy evidence in healthy adults |
| WADA | ❌ Prohibited at all times (S2) |
Biology: The Growth Hormone Axis
Endogenous GH: pulsatile, nocturnal, complex
Growth hormone is a 191-amino acid, 22-kDa polypeptide synthesised and secreted by somatotroph cells in the lateral wings of the anterior pituitary gland. Its secretion is released in discrete pulses, typically 6–8 per day in young adults, with the largest pulse occurring 30–90 minutes after sleep onset during slow-wave sleep. Between pulses, circulating GH is essentially undetectable.
Pulsatility is regulated by GHRH from hypothalamic arcuate neurons (stimulates release), somatostatin from hypothalamic periventricular neurons (inhibits release), ghrelin from the stomach fundus (stimulates release), and IGF-1 (negative feedback on both hypothalamus and pituitary). After puberty, GH secretion declines exponentially — approximately 14% per decade. By age 60, endogenous GH production may be 10-fold lower than during puberty. This age-related decline is termed somatopause.[1]
Signal transduction: GH receptor → JAK-STAT
Somatropin binds to dimeric GH receptors on target tissue cells. GH binding causes receptor dimerisation, activating JAK2 kinase, which phosphorylates STAT5b, which translocates to the nucleus and activates GH-responsive genes — principally IGF-1 in the liver, but also multiple genes involved in glucose metabolism, lipid oxidation, and protein synthesis. Some pharmacodynamic effects are primarily mediated by IGF-I produced in the liver (e.g., skeletal growth, protein synthesis), while others are primarily a direct consequence of somatropin (e.g., lipolysis).[2]
IGF-1: the critical mediator
Most of GH’s anabolic effects are mediated indirectly through IGF-1, produced primarily by the liver under GH stimulation. IGF-1 promotes chondrocyte proliferation (bone growth at growth plates), protein synthesis in muscle, and cell proliferation broadly — which has dual implications for anabolism and cancer risk. IGF-1 is used clinically as the primary proxy measure for GH axis activity, since single-point GH measurements are unreliable due to pulsatility. IGF-1 levels peak in puberty and decline with age, mirroring the somatopause GH decline.
Direct GH effects (IGF-1 independent)
GH directly stimulates adipocyte triglyceride breakdown (lipolysis) — the primary explanation for fat loss in GHD adults on replacement therapy. It also has anti-insulin effects: supraphysiological GH raises blood glucose and impairs insulin sensitivity. Sodium and water retention explains the oedema frequently seen in the first weeks of GH therapy.
History: From Cadaveric Extraction to Recombinant Technology
The cadaveric era (1958–1985) and its tragedy
Before recombinant technology, human growth hormone was extracted from pituitary glands of human cadavers. In 1985, this era ended abruptly when it was confirmed that cadaveric hGH preparations were contaminated with prions causing Creutzfeldt-Jakob disease (CJD) — a fatal neurodegenerative condition. Over 200 recipients worldwide eventually developed iatrogenic CJD, with cases continuing to emerge decades after the last contaminated treatment due to the extreme incubation periods of prion diseases. This represents one of the most tragic chapters in pharmaceutical medicine.
Genentech pioneered recombinant human growth hormone for human therapy, which was approved by the FDA in 1985. The recombinant product (somatropin) has the identical 191-amino acid sequence as the 22-kDa isoform of endogenous GH. No prion transmission has occurred with any recombinant preparation.
The Rudman 1990 NEJM study and the anti-aging industry
One study created an entire industry. In 1990, Daniel Rudman and colleagues published in the New England Journal of Medicine a study of 12 men over age 60 treated with GH for six months: 4.7 kg increase in lean body mass, 3.5 kg decrease in adipose mass, and increase in lumbar spine density, at approximately twice the dose used in adult GHD.[3] This incited a proliferation of “anti-aging” clinics and lay publications extolling HGH as a reversal of ageing.
FDA-Approved Indications
Paediatric indications
| Indication | Key features |
|---|---|
| Paediatric GHD | Most established; stimulation tests required; two peak GH values <10 ng/mL; treatment continues until epiphyseal fusion |
| Turner syndrome | Chromosomal condition (45,X); GH approved for height augmentation |
| Prader-Willi syndrome | Genetic obesity syndrome; GH improves body composition and function |
| Chronic kidney disease (CKD) | Uraemia impairs GH signalling; replacement improves growth |
| Small for gestational age (SGA) without catch-up | Catch-up growth failure by age 2; approved since 2001 |
| SHOX deficiency | Haploinsufficiency of short stature homeobox gene |
| Idiopathic short stature | Height SDS ≤ −2.25 without underlying etiology; first pure height-based indication (2003) |
| Noonan syndrome | Genetic syndrome; GH modestly improves final height |
Adult indications
| Indication | Key features |
|---|---|
| Adult GHD | Documented GHD from pituitary/hypothalamic pathology; GH stimulation test required; improves body composition, bone density, quality of life |
| HIV/AIDS wasting (Serostim) | Approved for serious weight loss and muscle wasting; doses higher than GHD replacement |
| Short bowel syndrome (Zorbtive) | 4-week treatment to improve intestinal absorption during specialised nutritional support |
Long-acting formulations (once-weekly)
Sogroya (somapacitan, Novo Nordisk): Weekly injection using reversible albumin-binding fatty acid derivative; approved for adults (2021) and extended to paediatrics. Skytrofa (lonapegsomatropin, Ascendis Pharma): Weekly injection using TransCon linker prodrug; approved for paediatric GHD (2021) and extended to adult GHD on July 28, 2025. Approval was supported by data from the foresiGHt trial — a Phase 3, multicenter, randomised, placebo-controlled double-blind study involving 259 adults with GHD, in which IGF-1 SDS levels normalised in the Skytrofa group compared to persistent deficiency in the placebo group.[12]
Clinical Evidence: GHD vs. Healthy Adults
In documented GHD: strong and established
Adult GHD following pituitary/hypothalamic disease produces a well-characterised clinical syndrome: increased visceral fat, decreased lean mass, reduced bone density, impaired quality of life, dyslipidaemia, and increased cardiovascular risk. GH replacement therapy produces reduction in visceral adipose tissue, increase in lean body mass, improvement in bone mineral density, normalisation of lipid profile (LDL reduction), quality of life improvement, and some evidence of reduced cardiovascular risk markers. These benefits are well-supported by multiple RCTs and are the basis for the FDA approvals.[2]
In healthy older adults: body composition without function
The picture changes fundamentally when GH is given to endocrinologically normal adults with age-related (not pathological) GH decline. Controlled studies show GH supplementation in older men increases lean mass by ~2 kg with similar reductions in fat mass.[5] There is little evidence that GH treatment improves muscle strength and performance (e.g., walking speed or ability to climb stairs) or quality of life.
The Blackman et al. JAMA 2002 trial (N=57+61 women) — the most rigorous placebo-controlled trial of GH + sex steroids in healthy older adults — confirmed the body composition changes but found no improvement in peak oxygen uptake, muscle strength, or cognitive function.[6] Side effects were common: fluid retention (reported in 11–100% across studies), carpal tunnel syndrome, joint pain, and mild glucose intolerance. The pattern is consistent across the literature: a person using HGH off-label may look somewhat leaner — without meaningfully performing better, living longer, or functioning better in daily activities.
The Longevity Paradox: GH/IGF-1 and Lifespan
Animal evidence: less GH = longer life
In laboratory mice, genetic GH deficiency or resistance leads to a remarkable extension of longevity accompanied by signs of delayed and/or slower aging, leading to the counterintuitive conclusion that the actions of GH normally released by the pituitary somehow limit life expectancy and likely accelerate the biological process of aging.[9] Ames dwarf mice (GH deficient) live 35–65% longer than wild-type; Snell dwarf mice show similar lifespan extension; GH receptor knockout mice (“Laron mice”) live significantly longer and are resistant to cancer; GH-overexpressing transgenic mice are short-lived with accelerated aging phenotypes.
Human evidence: Laron syndrome and centenarians
Individuals with Laron syndrome (GH receptor mutations, severe GH resistance) have strikingly low rates of cancer and diabetes. The Ecuadorian cohort studied by Guevara-Aguirre showed near-zero cancer rates over decades of follow-up. Studies have found that many centenarians have mutations that keep their IGF-1 levels naturally below average. In one study following 184 men and women in their mid-90s for up to 11 years, every 1-nanogram per millilitre decrease in IGF-1 translated into about one more week of life.[11] In humans, more subtle variations in GH and IGF-1 signalling are associated with reduced old-age mortality, particularly in women, and with improved chances of attaining extremes of lifespan.[9]
What this means for anti-ageing HGH use
The longevity biology does not establish that HGH administration causes premature death in healthy middle-aged adults. What the data does establish is that the premise driving anti-ageing HGH use — that the age-related decline in GH/IGF-1 is a disease process to be corrected — is almost certainly wrong. The decline in GH with age may be adaptive rather than pathological. Restoring youthful GH/IGF-1 levels in ageing adults may carry real risk of accelerating the very processes (cell proliferation, metabolic dysregulation) that the natural decline was partially protecting against.
Safety
Well-established adverse effects
| Effect | Frequency | Clinical significance |
|---|---|---|
| Fluid retention / oedema | 11–100% (dose-dependent) | Usually mild; can worsen hypertension |
| Joint and muscle pain | Common | Limits dose escalation |
| Carpal tunnel syndrome | Common | Median nerve compression from fluid retention |
| Glucose intolerance / insulin resistance | Common | ⚠️ Can precipitate diabetes in predisposed individuals |
| Gynecomastia | 7–14% | From aromatisation of elevated androgens |
| Intracranial hypertension (pseudotumour cerebri) | Rare | Headache, visual disturbance; reversible with dose reduction |
| Slipped capital femoral epiphysis | Paediatric | Limp, hip/knee pain; evaluate promptly |
| Scoliosis progression | Paediatric | Monitor growing patients |
Cancer risk
⚠️ This is the most serious unresolved question in GH pharmacology. IGF-1 promotes cell proliferation through anti-apoptotic and mitogenic effects. HGH is contraindicated in active malignancy. An increased risk of a second neoplasm has been reported in childhood cancer survivors treated with radiation to the brain/head who developed subsequent GHD and were treated with somatropin.[2] For healthy adults using HGH off-label, the long-term cancer risk has not been definitively quantified, but given the longevity biology implicating IGF-1 in cancer promotion, this risk is a genuine concern — not theoretical.
The critical illness mortality signal
⚠️ Among the most significant HGH safety findings was the discovery that high-dose rhGH given to critically ill ICU patients increased mortality — a finding so robust it led to early termination of multiple trials. This is why the Van den Berghe GHRP-2 work explored secretagogues as a potentially safer alternative. The mechanism involved impaired wound healing, exacerbated insulin resistance, and altered immune function in the catabolic environment of critical illness.
Legal Framework
⚠️ The legal status of HGH in the United States is unusually explicit. Under the Human Growth Hormone Restrictions Act (1990, amended), it is a federal criminal offence (felony) to distribute or possess human GH for any purpose other than an FDA-approved indication with a valid prescription. This law specifically names “anti-aging” and “body building” as explicitly prohibited uses. Off-label prescribing by physicians is legally distinct — a physician can prescribe HGH off-label — but doing so for anti-ageing or body composition purposes exposes the prescriber to DEA scrutiny and professional licence risk.[13]
Comparison: HGH vs. GH Secretagogues
| Feature | Exogenous HGH | GHRP-2 / Ipamorelin / CJC-1295 (secretagogues) |
|---|---|---|
| Mechanism | Direct GH replacement; bypasses all feedback | Stimulates pituitary to release endogenous GH; feedback intact |
| Pulsatility | Eliminated — sustained elevation | Preserved pulsatility |
| Somatostatin feedback | Bypassed | Active — limits response amplitude |
| IGF-1 elevation | More pronounced and sustained | More modest, physiologically constrained |
| ICU mortality signal | ⚠️ Increased in critically ill | Not observed (likely feedback-limited) |
| FDA status | ✅ Approved (specific indications) | ❌ Not approved (research compounds) |
| Anti-ageing legal status | ⚠️ Explicitly illegal (felony) | Not approved; prohibited for anti-ageing |
| WADA | ❌ Prohibited | ❌ Prohibited |
Common Misconceptions
“The Rudman study proves HGH reverses ageing.”
The Rudman study demonstrated body composition changes over 6 months in 12 men with a non-blinded design at twice the GHD dose. The author himself repudiated its use as evidence for anti-ageing.[3] Subsequent blinded RCTs confirmed body composition changes but found no functional improvement.[6]
“Since GH declines with age, replacing it is natural and beneficial.”
The somatopause parallel to menopause breaks down under examination. Menopausal oestrogen decline causes documented pathological consequences from loss of an ongoing protective signal. GH decline in ageing may be a regulatory adaptation rather than pathology — the longevity biology strongly suggests that some GH decline with age is protective.[9]
“I just need to raise my IGF-1 to youthful levels.”
Youthful IGF-1 levels are associated with growth during a period of life designed for growth. In post-growth adults, particularly the elderly, elevated IGF-1 is associated with cancer risk. The centenarian and Laron syndrome data collectively suggest that lower-than-average IGF-1 in post-reproductive life may be associated with greater longevity, not lesser.[11]
“Peptide secretagogues are a legal alternative to HGH.”
Secretagogues (ipamorelin, CJC-1295, etc.) are not FDA-approved, are prohibited by WADA, and have never been approved for anti-ageing use either. They occupy different legal territory from HGH (not felony possession in the same statutory sense) but are not a regulated alternative — they are research compounds with their own evidence limitations.
Frequently Asked Questions
Can a physician legally prescribe HGH for body composition or anti-ageing?
Off-label prescribing is legal for physicians, but prescribing HGH for anti-ageing or body building is explicitly prohibited by federal law and creates serious DEA and professional licensing exposure.[13]
What does documented adult GHD look like, and how is it diagnosed?
Adult GHD typically results from pituitary/hypothalamic disease (tumour, surgery, radiation, or head trauma). Diagnosis requires a GH stimulation test showing a peak GH below 3–5 µg/L (thresholds vary by assay and clinical context). Low IGF-1 alone is not sufficient for diagnosis in adults.
Does the once-weekly formulation work as well as daily?
The Phase 3 data for Skytrofa (lonapegsomatropin) and Sogroya (somapacitan) show comparable IGF-1 normalisation and body composition effects to daily somatropin in both paediatric and adult GHD. The weekly format substantially reduces injection burden and appears to improve adherence.[12]
What is the Endocrine Society’s position?
The Endocrine Society maintains that growth hormone therapy offers benefits in body composition, exercise capacity, skeletal integrity, and quality-of-life measures, and is most likely to benefit those patients who have more severe HGH deficiency. The Society does not endorse HGH for healthy adults or for anti-ageing.
Key Takeaways
- Somatropin is a well-characterised, FDA-approved drug with real efficacy in documented GHD. In the right population — children or adults with pathological GH deficiency from pituitary disease — it works, with meaningful clinical outcomes including height restoration, body composition normalisation, and quality of life improvement.
- In healthy adults, HGH produces body composition changes without functional benefit. Controlled studies consistently show +2 kg lean mass and −2 kg fat mass in healthy older adults. No study has shown improved muscle strength, physical function, or exercise capacity in endocrinologically normal adults.[6]
- ⚠️ The Rudman 1990 NEJM study was never evidence for anti-ageing use — its author said so explicitly, repeatedly. The 2003 NEJM editorial explicitly condemned the anti-ageing industry’s citation of Rudman’s work.[4]
- The longevity biology is counterintuitive and important. GH-resistant organisms live longer; human GH resistance syndromes protect from cancer; centenarians have low IGF-1. This fundamentally undermines the premise that more GH equals longer, healthier life.[8]–[10]
- ⚠️ Anti-ageing and body-building use of HGH is explicitly illegal under US federal law — a felony for distributors, and legally problematic for physicians who prescribe it for these purposes.
- The new once-weekly formulations (Skytrofa, Sogroya) represent genuine clinical advance for the GHD population — reducing injection burden while maintaining efficacy — but do not change the risk-benefit calculation for off-label use in healthy adults.[12]
References
Biology and Physiology
- Growth hormone. Wikipedia. en.wikipedia.org/wiki/Growth_hormone
- Norditropin (somatropin) prescribing information. Novo Nordisk. FDA, 2017/2025.
Anti-Ageing Evidence and Critique
- Rudman D, Feller AG, Nagraj HS, et al. Effects of human growth hormone in men over 60 years old. New England Journal of Medicine. 1990;323:1–6.
- Vance ML. Can Growth Hormone Prevent Aging? New England Journal of Medicine. 2003 (editorial).
- Papadakis MA, et al. Growth hormone replacement in healthy older men improves body composition but not functional ability. Annals of Internal Medicine. 1996;124(8):708–716.
- Blackman MR, et al. Growth hormone and sex steroid administration in healthy aged women and men: a randomized controlled trial. JAMA. 2002;288(18):2282–2292.
- Growth hormone and aging: a clinical review. Frontiers in Aging. 2025. PMC12009952
Longevity Biology
- Bartke A, et al. Growth hormone and aging: A challenging controversy. PMC. 2009. PMC2682398
- Bartke A. Growth hormone and aging: Updated review. PMC. 2019. PMC6305861
- Bartke A. GH and ageing: pitfalls and new insights. PMC. 2017. PMC5424628
- Milman S, et al. Studies from Albert Einstein College of Medicine / Nir Barzilai laboratory on IGF-1 and longevity in nonagenarians.
Regulatory
- Skytrofa (lonapegsomatropin) adult GHD approval. FDA, July 28, 2025. NCT05171855 (foresiGHt trial).
- Mayo Clinic. Human Growth Hormone (HGH): Does it slow aging? Updated 2024. mayoclinic.org
- FDA Import Alert 57-04. Detention of unapproved human growth hormone.
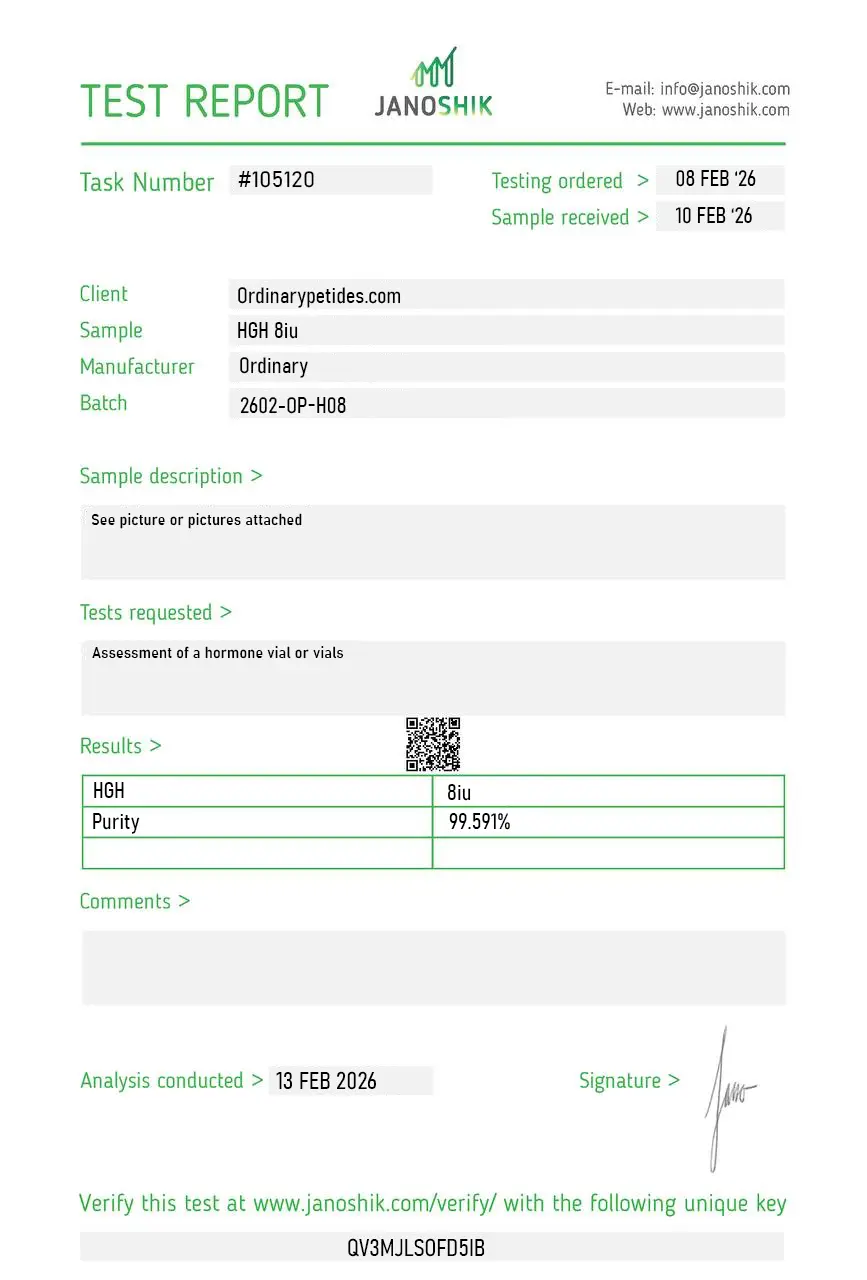
Certificate of Analysis
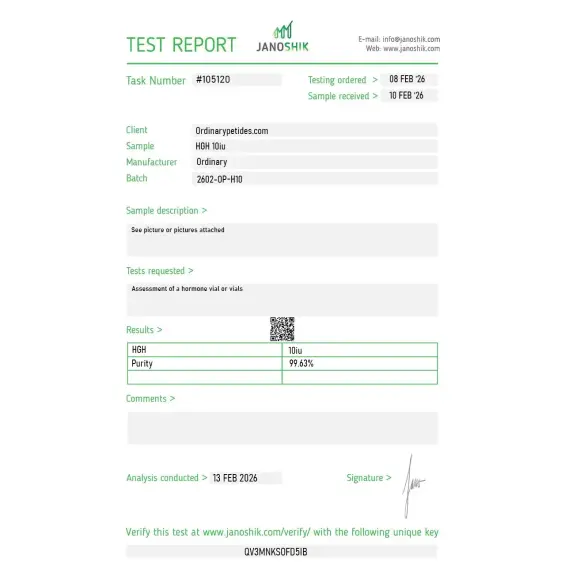
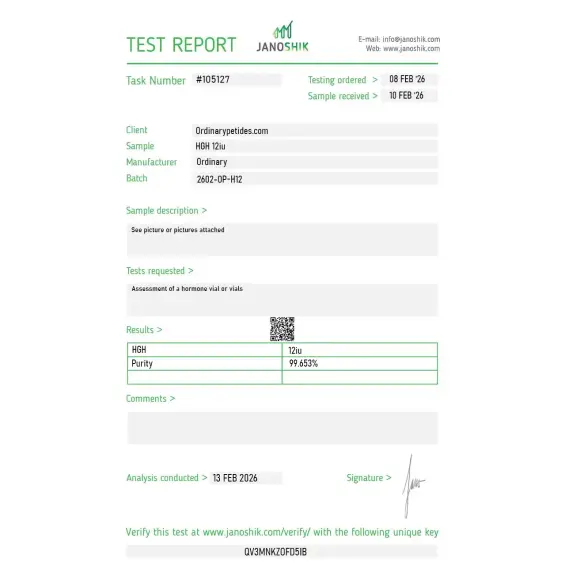
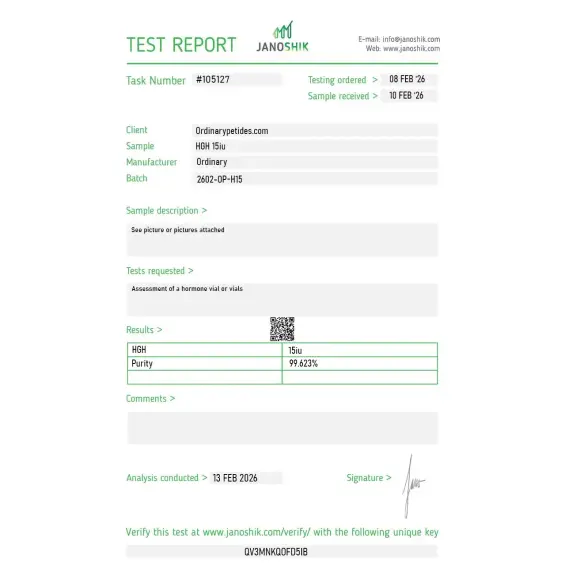
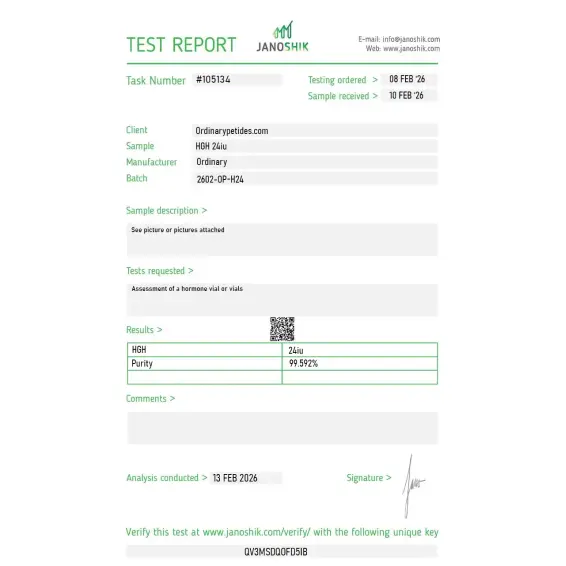
Independent test reports are available for HGH 6 IU, 8 IU, 10 IU, 12 IU, 15 IU, and 24 IU batches. These reports provide batch-level documentation and analytical verification information for research reference.




In everyday clinical use, medicinal HGH usually refers to somatropin, which is recombinant human growth hormone.
Yes. HGH is a peptide hormone.
In adults, it is best established for adult growth hormone deficiency. In children, it is used for growth hormone deficiency and some other clearly approved growth-related conditions.
In people with true growth hormone deficiency, it can improve body composition. But that does not make it a proven or appropriate weight-loss treatment for healthy people without deficiency.
No. Based on current medical guidance and regulatory standards, HGH is not considered a standard or approved anti-aging treatment.
No. WADA prohibits HGH in sport.
Human Growth Hormone (HGH), also called somatotropin, is a 191-amino acid single-chain polypeptide produced and secreted by somatotrope cells in the anterior pituitary gland. It is the largest and most complex compound in this series — substantially bigger than any peptide covered so far. It is released in pulses throughout the day, predominantly during deep slow-wave sleep, and is regulated by the interplay of hypothalamic GHRH (which stimulates release) and somatostatin (which inhibits it) — the same axis that CJC-1295, Ipamorelin, GHRP-2, and GHRP-6 work upstream of. Pharmaceutical recombinant HGH (rhGH) has been produced since 1985 when it replaced pituitary-derived HGH, which was withdrawn after cases of Creutzfeldt-Jakob disease transmission. Multiple FDA-approved rhGH products exist including Genotropin, Humatrope, Norditropin, Nutropin, Omnitrope, Saizen, Serostim, and Zomacton.
HGH exerts its effects through two pathways. Direct effects occur when HGH binds to GH receptors on target cells — in adipose tissue it directly stimulates lipolysis, breaking down triglycerides and mobilizing free fatty acids. Indirect effects — responsible for most of HGH's anabolic and growth-promoting actions — occur through IGF-1. HGH stimulates the liver and other tissues to produce IGF-1, which then mediates growth and repair of virtually every tissue in the body: stimulating protein synthesis in muscle, chondrocyte proliferation in bone, collagen synthesis in connective tissue, and organ growth. IGF-1 also exerts negative feedback on both HGH and GHRH, regulating the axis. The full-length molecule also influences glucose metabolism — opposing insulin's action and elevating blood glucose, which underlies HGH's diabetogenic potential at supraphysiological doses.
HGH has more approved indications than almost any compound in this series. In children it is approved for growth hormone deficiency, Turner syndrome, Prader-Willi syndrome, chronic renal insufficiency, children born small for gestational age who fail to catch up, Noonan syndrome, short stature homeobox gene deficiency, and idiopathic short stature. In adults it is approved for growth hormone deficiency resulting from pituitary disease, hypothalamic disease, surgery, radiation, or trauma. Serostim specifically is approved for AIDS-related wasting and cachexia. Zorbtive is approved for short bowel syndrome. These are legitimate, physician-supervised indications with well-established dosing protocols and regulatory oversight.
Off-label use of HGH in healthy adults for anti-aging, body composition improvement, and athletic performance enhancement is widespread but controversial and in most contexts illegal without a valid prescription. Reported off-label effects at supraphysiological doses include increased lean muscle mass, accelerated fat loss particularly visceral fat, improved recovery from exercise and injury, improved skin quality and collagen density, enhanced deep sleep, and increased bone density. The clinical evidence for these effects in healthy adults — as opposed to GH-deficient patients — is considerably weaker than commonly claimed. A comprehensive 2007 Annals of Internal Medicine meta-analysis found that GH in healthy older adults increased lean body mass and decreased fat mass but produced no improvements in strength, exercise capacity, or bone density, while causing significant adverse effects. HGH is explicitly prohibited by WADA under all circumstances and listed as a controlled substance in many jurisdictions.
This is one of the most important practical distinctions in this entire series. Exogenous HGH administration bypasses the entire HPG axis — it suppresses endogenous GH production through negative feedback via IGF-1, can cause receptor downregulation over time, and eliminates the natural pulsatile rhythm of GH secretion. At supraphysiological doses it produces a sustained, non-physiological GH elevation that drives the side effect profile below. GH secretagogues like CJC-1295 and Ipamorelin work upstream — stimulating the body's own pituitary to produce GH in natural pulses, preserving feedback loops and pituitary sensitivity. The tradeoff is that secretagogues cannot exceed the ceiling of what the pituitary can produce, while exogenous HGH is limited only by the dose injected. For this reason secretagogues are generally considered safer and more physiologically appropriate for optimization purposes, while exogenous HGH is reserved for confirmed GH deficiency in clinical settings.
Pharmaceutical HGH is administered by subcutaneous injection using prefilled pens or vials. Approved therapeutic doses for adult GHD are typically 0.2 to 0.6 mg daily, titrated based on IGF-1 levels and clinical response. Off-label optimization doses range from 1 to 3 IU daily in wellness contexts. Performance enhancement doses are considerably higher — often 4 to 8 IU or more daily — and carry substantially greater risk. It has a short half-life of approximately 20 to 30 minutes after injection but produces prolonged downstream effects through IGF-1, which has a half-life of 12 to 15 hours. Timing relative to meals matters — insulin elevation from food blunts GH action.
At therapeutic doses in GH-deficient patients side effects are manageable and well-characterized. The most common are fluid retention, joint pain and swelling, carpal tunnel syndrome, and injection site reactions. At supraphysiological or long-term use doses, more serious effects emerge. Insulin resistance and diabetes are well-documented — HGH directly opposes insulin signaling and chronic elevation significantly impairs glucose metabolism. Acromegaly — characterized by enlargement of hands, feet, facial features, and organs including the heart and liver — is the endpoint of chronic HGH excess, driven by sustained IGF-1 elevation. Cardiomegaly and cardiomyopathy are serious cardiac risks. Gynecomastia can develop through increased aromatization. Elevated IGF-1 at supraphysiological levels is associated with increased cancer risk — IGF-1 is a potent mitogen and its role in promoting cell proliferation has been extensively documented in multiple cancer types including breast, prostate, and colorectal. Headaches, nerve compression syndromes, and peripheral edema are also common at higher doses.
Anyone with active malignancy or a history of cancer should not use HGH outside of strictly controlled oncology contexts — the IGF-1 elevation it produces is a significant cancer promotion concern. People with diabetes or insulin resistance face worsening glucose control. Those with active proliferative diabetic retinopathy should not use it. Children with closed epiphyseal plates should not use GH therapy for growth indications. People with Prader-Willi syndrome who are severely obese or have sleep apnea face increased risk of sudden death on GH therapy. Competitive athletes face career-ending consequences from WADA detection — HGH is detectable for several days using the isoform differential assay. Obtaining HGH without a valid prescription is illegal in the United States and most other countries. Anyone considering HGH therapy for anti-aging or optimization purposes should understand the evidence base does not support the dramatic claims commonly made, while the risk profile — particularly for cancer and diabetes — is real and dose-dependent.





