







HGH Fragment 176-191
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
HGH Fragment 176–191: An Interesting Research Fragment With a Strong Concept, but Not a Proven Human Fat-Loss Therapy
HGH Fragment 176–191, also known in its research history as AOD9604, is not full growth hormone but a short C-terminal fragment of it, which once attracted attention as a candidate for studying lipolysis and antilipogenesis.
In preclinical models and in studies of human adipose tissue ex vivo, it showed interesting metabolic signals — which is exactly why an almost legendary reputation grew around it as a "fat-loss peptide." And this is where the lab romance meets the clinical paperwork — a plot twist many peptides do not enjoy.
In the clinical context, the obesity program did not produce a statistically significant reduction in body weight, and development in that direction was discontinued. So this is not a story about a "secret working drug that was simply underestimated," but rather an example of how a beautiful biological idea does not have to turn into a convincing result in humans.
That is exactly why Fragment 176–191 is interesting first and foremost as a research peptide with a strong concept and a noticeable drug-development history.
Practical Takeaway
If what matters to you is not myths but real scientific context, this is exactly the kind of case where you should look not at the promises, but at what the substance actually showed in studies.
HGH Fragment 176-191: A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
HGH Fragment 176-191 is a synthetic peptide corresponding to amino acids 176 through 191 at the C-terminal end of human growth hormone — the portion of GH believed to be responsible for most of its lipolytic (fat-mobilising) activity. The theoretical premise is elegant: capture GH’s fat-burning benefits in a small, targetable fragment, without the complications (IGF-1 elevation, insulin resistance, growth promotion, cancer risk) that come with full-length GH.
Based on the most rigorous available evidence, the premise was partially right and the clinical outcome was insufficient. The animal evidence is real and published in peer-reviewed journals.[1][2] A 12-week randomised trial showed a meaningful signal. The pivotal 24-week trial (OPTIONS study, N=536) did not show statistically significant weight loss at the primary endpoint, and Metabolic Pharmaceuticals halted the development programme in 2007.
| At a glance | |
|---|---|
| Also known as | HGH Frag 176-191; GH Fragment 176-191; hGH (176-191) |
| Clinical development form | AOD9604 (Anti-Obesity Drug 9604) — N-terminal tyrosine substitution |
| Sequence (unmodified) | hGH residues 176–191: Ser-Leu-Leu-Arg-Ile-Val-Gln-Cys-Arg-Ser-Val-Glu-Gly-Ser-Cys-Gly-Phe |
| AOD9604 modification | Tyr replaces Phe at N-terminus; improves stability and oral bioavailability |
| CAS (unmodified fragment) | 66004-57-7 |
| Proposed primary mechanism | β-3 adrenergic receptor upregulation → lipolysis; independent of GH receptor and IGF-1 |
| FDA status | ❌ Not approved; PCAC December 2024 rejected for 503A compounding |
| WADA | ❌ Prohibited at all times (Growth Hormone Fragments category) |
| Development history | Phase 2B (OPTIONS, N=536) failed primary endpoint; programme terminated 2007 |
The Molecular Context: Why This Fragment?
Human growth hormone is a 191-amino acid, single-chain polypeptide. Structure-activity studies in the 1990s established that the C-terminal region, particularly residues 177–191, contains the primary sequence responsible for GH’s lipolytic activity, while the N-terminal and mid-chain regions are more important for GH receptor binding and IGF-1 stimulation. This suggested a pharmacological opportunity: synthesise just the fat-burning portion of GH to get selective lipolysis without the complications of full GH therapy — no IGF-1 elevation, no insulin resistance, no growth promotion, no cancer risk amplification.
Fragment 176-191 vs. AOD9604: an important distinction
The unmodified fragment corresponds exactly to hGH residues 176–191, with a native phenylalanine at the N-terminus. AOD9604 is the modified, clinically tested derivative: essentially hGH 177–191 with a tyrosine substituted at the N-terminus, improving stability against enzymatic degradation and enhancing oral bioavailability. In the commercial research peptide market, “HGH Fragment 176-191” and “AOD9604” are often used interchangeably — pharmacologically imprecise, though AOD9604’s human clinical data is the only meaningful human evidence available for this structural class.[6]
Chemistry
| Property | Unmodified HGH Frag 176-191 | AOD9604 |
|---|---|---|
| Length | 16 amino acids | 16 amino acids |
| N-terminal residue | Phenylalanine | Tyrosine (added for stability) |
| CAS | 66004-57-7 | N/A (modified derivative) |
| MW | ~1,815 Da | ~1,818 Da |
| Oral bioavailability | Poor | Substantially improved |
| Disulfide bridges | Yes (Cys-Cys) | Yes (Cys-Cys) |
| Stability in plasma | Short | Better than unmodified |
The internal Cys-Cys disulfide bridge is important for maintaining the peptide’s secondary structure and receptor-interaction geometry. Loss of this structure through oxidation would abolish activity.
Mechanism of Action
What is established
The most thoroughly characterised mechanism involves the β-3 adrenergic receptor (β3-AR) pathway in adipocytes. Both hGH and AOD9604 can reduce body weight and body fat in obese mice following chronic administration, correlating with increases in the level of expression of β3-AR RNA — the major lipolytic receptor found in fat cells. Importantly, both compounds are capable of increasing the repressed levels of β3-AR RNA in obese mice to levels comparable with those in lean mice.[2] The β3-AR is a G-protein coupled receptor expressed in adipose tissue; in obese subjects, β3-AR expression is downregulated, contributing to impaired fat mobilisation.
What is not established
AOD9604 does not compete for the hGH receptor and does not induce cell proliferation, unlike full-length hGH. However, no specific high-affinity receptor for AOD9604 has been identified. The identity of the primary receptor remains unresolved. β3-AR upregulation appears to be a downstream secondary effect, as AOD9604 can acutely increase fat oxidation even in β3-AR knockout mice. Additional proposed mechanisms include inhibition of lipogenesis, increased mitochondrial fat oxidation, and a β3-AR-independent acute lipolytic pathway. Interaction with the melanocortin-4 receptor (MC4R) has been suggested in some sources but remains unconfirmed in the primary literature.[1]
Key properties compared to full-length GH
| Property | Full-length HGH | HGH Fragment 176-191/AOD9604 |
|---|---|---|
| GH receptor binding | Yes — primary mechanism | ❌ No |
| IGF-1 stimulation | Yes — major effect | ❌ No |
| Insulin resistance | Yes — dose-dependent | ✅ No — confirmed across 6 clinical trials |
| Cell proliferation | Yes — IGF-1 mediated | ❌ No |
| Lipolysis | Yes | Yes (though insufficient in pivotal trial) |
| Cancer risk concern | Significant | Theoretically reduced (no IGF-1/GHR) |
Clinical Development History: From Promise to Failure
Phase 1 and Phase 2A: safety and dose ranging
Phase 1 (METAOD001) administered single doses from 25 to 400 µg/kg IV to 15 healthy adult males. Compared against rhGH as a positive control, AOD9604 did not elevate GH or IGF-1. Safety was established. Phase 2A studies (METAOD002, METAOD003) tested IV and oral single doses in obese males, confirming the absence of GH-like hormonal effects and establishing oral dosing feasibility.[3]
Phase 2A/B (METAOD004): 12-week oral trial — the positive signal
This was the study that generated clinical excitement. In a 12-week randomised clinical trial, subjects receiving AOD9604 (1 mg/day) lost an average of 2.6 kg compared to 0.8 kg in the placebo group. The 1.8 kg additional weight loss over placebo was statistically significant. The compound showed no effect on glucose, insulin, or IGF-1 levels.
Phase 2B (METAOD006 / OPTIONS study): the pivotal failure
The definitive trial: 536 obese adults, 24 weeks, doses of 0, 0.25, 0.5, and 1 mg/day oral AOD9604. The pivotal trial enrolled a larger cohort and failed to replicate statistically significant weight loss, which led Metabolic Pharmaceuticals to halt the formal drug development programme in 2007.[4][5] Possible contributing factors include the modest absolute effect size (even the positive trial showed only 1.8 kg additional loss — modest compared to GLP-1 agonists now achieving 15–25% body weight reduction), an unusual inverse dose-response in the 12-week trial, and inherently variable oral peptide bioavailability.
GRAS designation: what it does and does not mean
After the development programme ended, AOD9604 received Generally Recognised as Safe (GRAS) designation for use as a food ingredient — not as a drug. GRAS for food means the substance is considered safe for oral consumption in food products at specified levels. It explicitly does not constitute FDA approval as a drug and does not validate therapeutic efficacy claims. Some marketing implies FDA sanction from this GRAS designation — this is misleading.
PCAC December 2024: compounding rejected
The Pharmacy Compounding Advisory Committee reviewed AOD9604 for inclusion on the 503A bulks list. The committee declined to add it. The clinical evidence base — including the failed pivotal trial — was a central consideration.[7]
Safety across clinical trials
Across six trials involving approximately 900 participants, glucose levels, insulin levels, and markers of insulin sensitivity remained unchanged from baseline. No serious adverse events were attributed to the compound and no antibody formation against the peptide was observed.[3] The safety data is the most credible human data from the development programme. The compound’s problem is not safety but efficacy.
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) — drug | ❌ Not approved; PCAC December 2024 rejected for 503A compounding [7] |
| FDA (USA) — food | GRAS designation for food ingredient use (not a drug approval) |
| WADA | ❌ Prohibited at all times — classified under “Growth Hormone Fragments” in S2 [8] |
| TGA (Australia) | Not registered as a therapeutic good |
| EMA (Europe) | Not approved |
The Unmodified Fragment 176-191: Where Is the Human Evidence?
⚠️ The unmodified HGH Fragment 176-191 has never been tested in a human clinical trial. All human clinical data — the 12-week positive signal, the 24-week pivotal failure, the safety database of 900 participants — comes from AOD9604, the tyrosine-modified derivative. Extrapolating AOD9604 clinical data to the unmodified fragment requires unvalidated assumptions about oral bioavailability (AOD9604 was specifically designed for oral delivery; the unmodified fragment has inferior oral bioavailability), receptor binding characteristics, and pharmacokinetics in humans. No published controlled trial of the unmodified fragment 176-191 in humans exists in any form.
What Is Established and What Is Not
| ✅ Established | ❌ Not established |
|---|---|
| AOD9604 does not bind GH receptor (confirmed in vitro) [1] | Identity of the primary receptor for AOD9604/fragment 176-191 |
| AOD9604 does not elevate IGF-1 in humans (6 trials, N=893) [3] | Long-term safety of injectable unmodified fragment 176-191 |
| AOD9604 reduces body weight in obese mice [1] | Clinically meaningful fat loss in humans at 24 weeks (failed) [4] |
| 1.8 kg additional weight loss at 12 weeks in one trial | Whether this 12-week signal is reproducible in larger/longer trials |
| GRAS status for food ingredient | Any drug-like therapeutic efficacy |
| Unmodified fragment 176-191 causes lipolysis in cell cultures | Any human pharmacokinetic or efficacy data for the unmodified fragment |
Common Misconceptions
“HGH Fragment 176-191 is FDA-approved.”
It is not. The GRAS designation applies to AOD9604 as a food ingredient — not to HGH Fragment 176-191, and not to AOD9604 as a drug. No therapeutic approval exists in any form.
“The research proves it works for fat loss.”
⚠️ The 12-week trial showed a modest, statistically significant effect. The 24-week pivotal trial in 536 patients did not replicate it.[5] By the standard applied in pharmaceutical development — and that should be applied to self-administered compounds — a failed pivotal trial is a negative result.
“AOD9604 is the same as HGH Fragment 176-191.”
Structurally similar but not identical. AOD9604 has a tyrosine substitution at the N-terminus. Human clinical data applies only to AOD9604.
“Because it doesn’t raise IGF-1, it’s safe for cancer patients.”
The absence of IGF-1 elevation is a genuine differentiating safety feature compared to full HGH. However, this does not establish safety in cancer patients. The compound is not approved for any condition, and the fragments’ effects on tumour cell behaviour have not been studied.
Frequently Asked Questions
Why is this compound still widely used despite the failed trial?
Several factors: the compound entered the research peptide market before the pivotal trial results were publicly prominent; the GRAS designation created an impression of regulatory endorsement; the injectable SC form may have better bioavailability than the oral form tested clinically; and short-term body composition effects in some users are attributed to the peptide when caloric deficit and exercise are simultaneously applied.
Is injectable HGH Fragment 176-191 more effective than the oral form that failed?
The clinical trials used oral AOD9604. Many current users inject the unmodified fragment subcutaneously. Whether SC injection achieves plasma levels that oral dosing did not is pharmacologically plausible but unknown — no pharmacokinetic comparison has been published. This remains speculation.
Key Takeaways
- HGH Fragment 176-191 and AOD9604 are related but distinct compounds. All published human clinical data — good and bad — applies to AOD9604 (the tyrosine-modified form). The unmodified fragment 176-191 has never been formally tested in humans.
- The drug development rationale was scientifically sound — isolating the lipolytic portion of GH to achieve fat-burning without GH receptor activation, IGF-1 elevation, or insulin resistance. The animal evidence was consistent and the early human signal was real.[1][2]
- ⚠️ The pivotal trial failed. 536 subjects, 24 weeks, three dose levels — no statistically significant weight loss. This is the definitive human evidence statement. A 12-week positive signal that does not replicate in a larger, longer trial is an insufficient evidence base.[4]
- ⚠️ The PCAC’s December 2024 rejection for 503A compounding reflects this evidence gap. The committee’s standard — demonstrated safety and clinical plausibility — was not met for therapeutic compounding.[7]
- WADA prohibits it under growth hormone fragments — appropriate given the parent molecule’s doping potential and the fragment’s designed metabolic activity.[8]
- The safety profile across human trials is genuinely good — no serious adverse events, no IGF-1 elevation, no insulin resistance across 900+ participants.[3] A safe drug that doesn’t work in its pivotal trial is still a failed drug.
References
Preclinical Evidence
- Heffernan M, et al. Increase of fat oxidation and weight loss in obese mice caused by chronic treatment with human growth hormone or a modified C-terminal fragment. Endocrinology. 2001;142(12). PMID: 11713213
- Heffernan M, et al. The effects of human GH and its lipolytic fragment (AOD9604) on lipid metabolism following chronic treatment in obese mice and beta(3)-AR knock-out mice. Endocrinology. 2001. PMID: 11673763
Human Clinical Safety Data
- Stier H, et al. Safety and Tolerability of the Hexadecapeptide AOD9604 in Humans. Journal of Endocrinology and Metabolism. 2013;3(1–2):7–15.
Clinical Trial History and Pivotal Failure
- BioSpace (2006). Metabolic Pharmaceuticals’s Obesity Trial Update: First 100 Subjects Complete The Phase 2B Trial Of AOD9604. biospace.com
- Kos K, et al. Obesity Pharmacotherapy: Current Perspectives and Future Directions. PMC3584306
- AOD9604. Wikipedia. en.wikipedia.org/wiki/AOD9604
Regulatory
- PCAC (Pharmacy Compounding Advisory Committee). December 2024 meeting — AOD9604 not added to 503A bulks list. fda.gov
- WADA. Prohibited List — S2 (Growth Hormone and related fragments). wada-ama.org
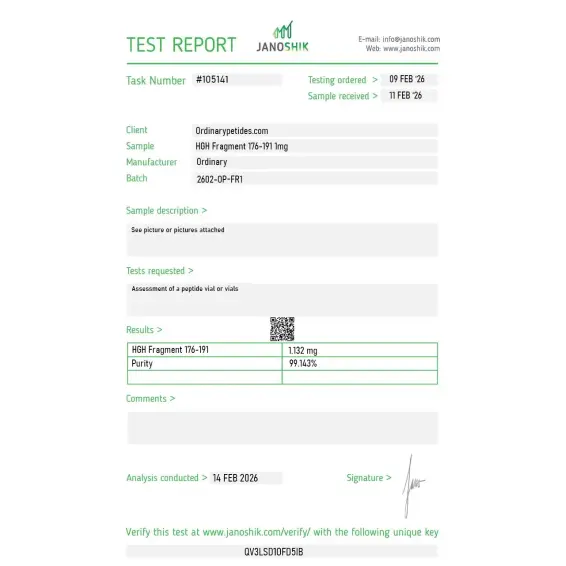
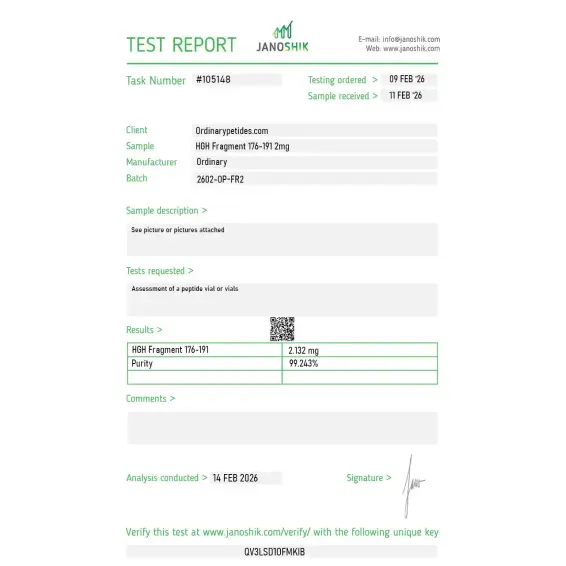
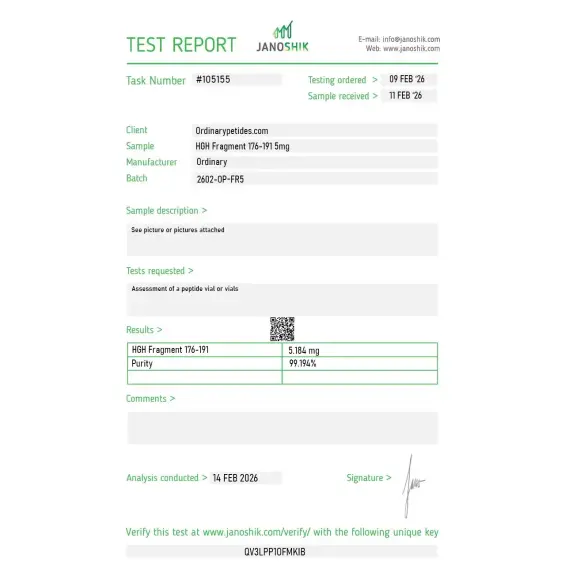
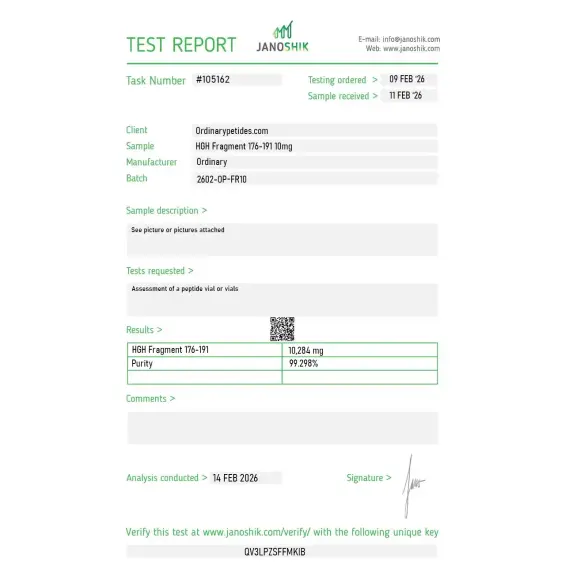
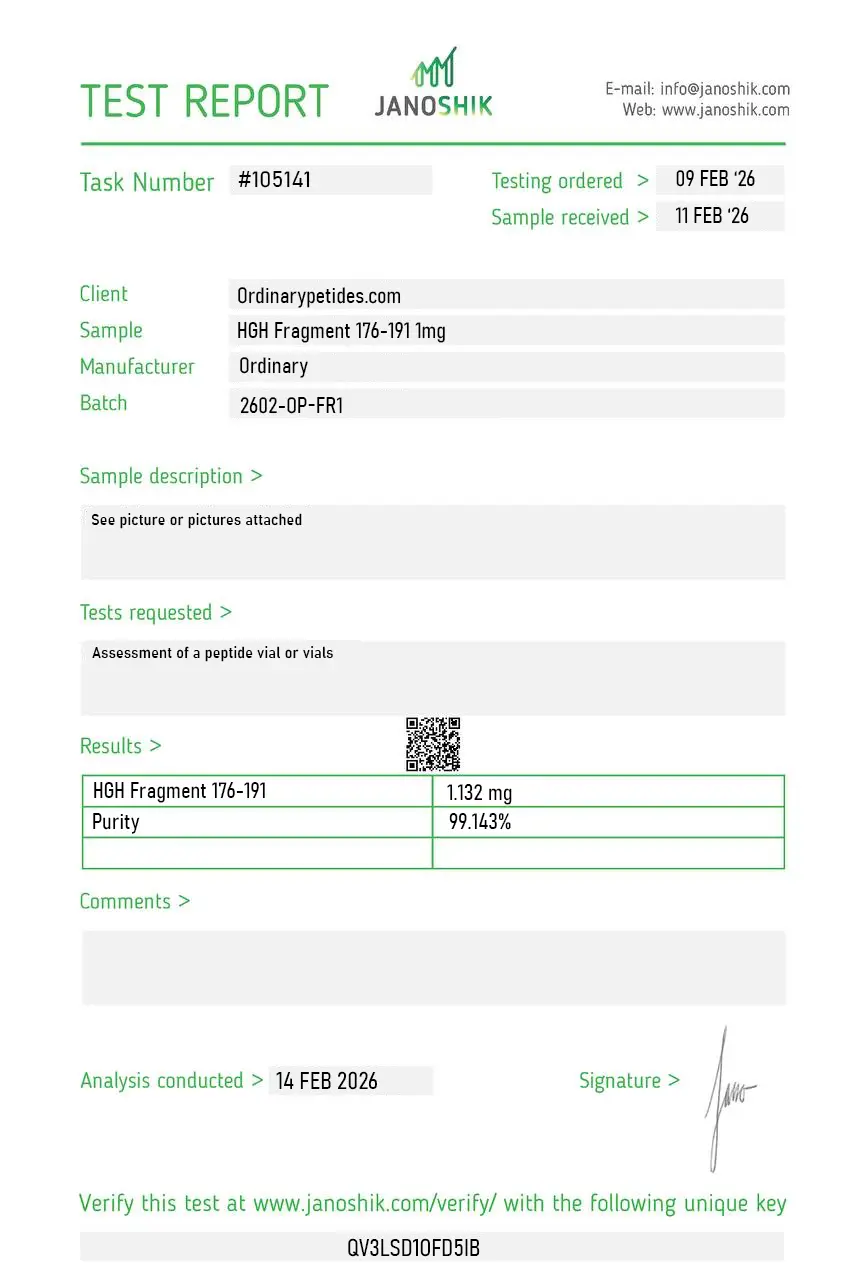
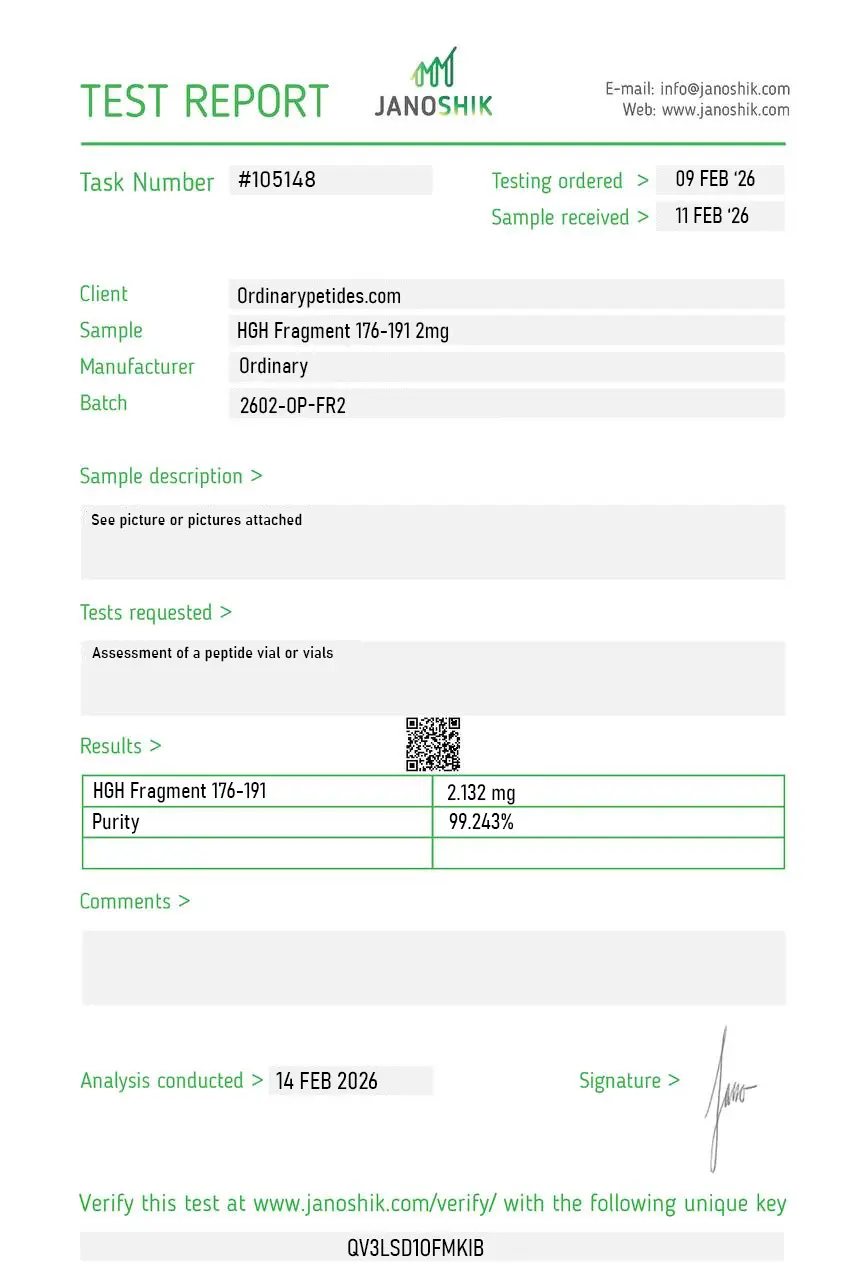
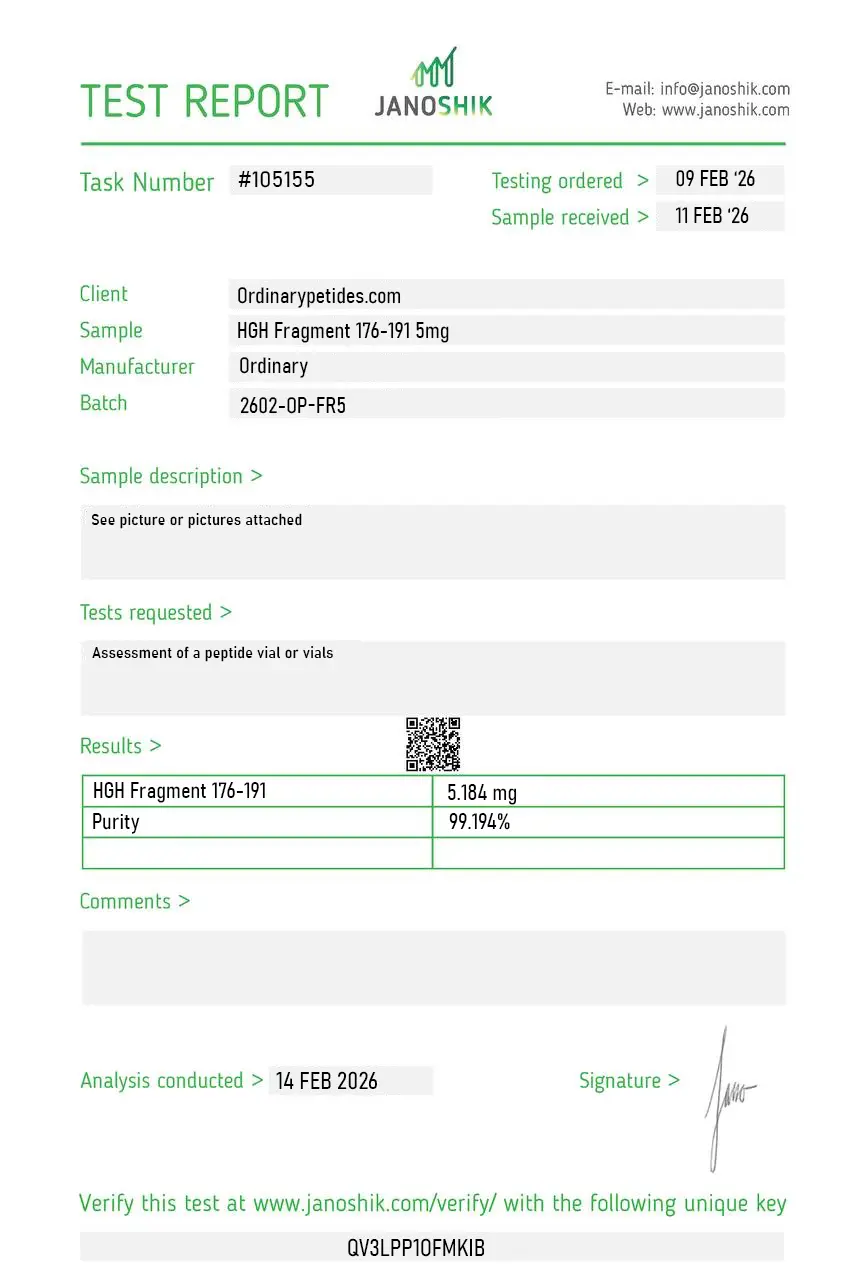
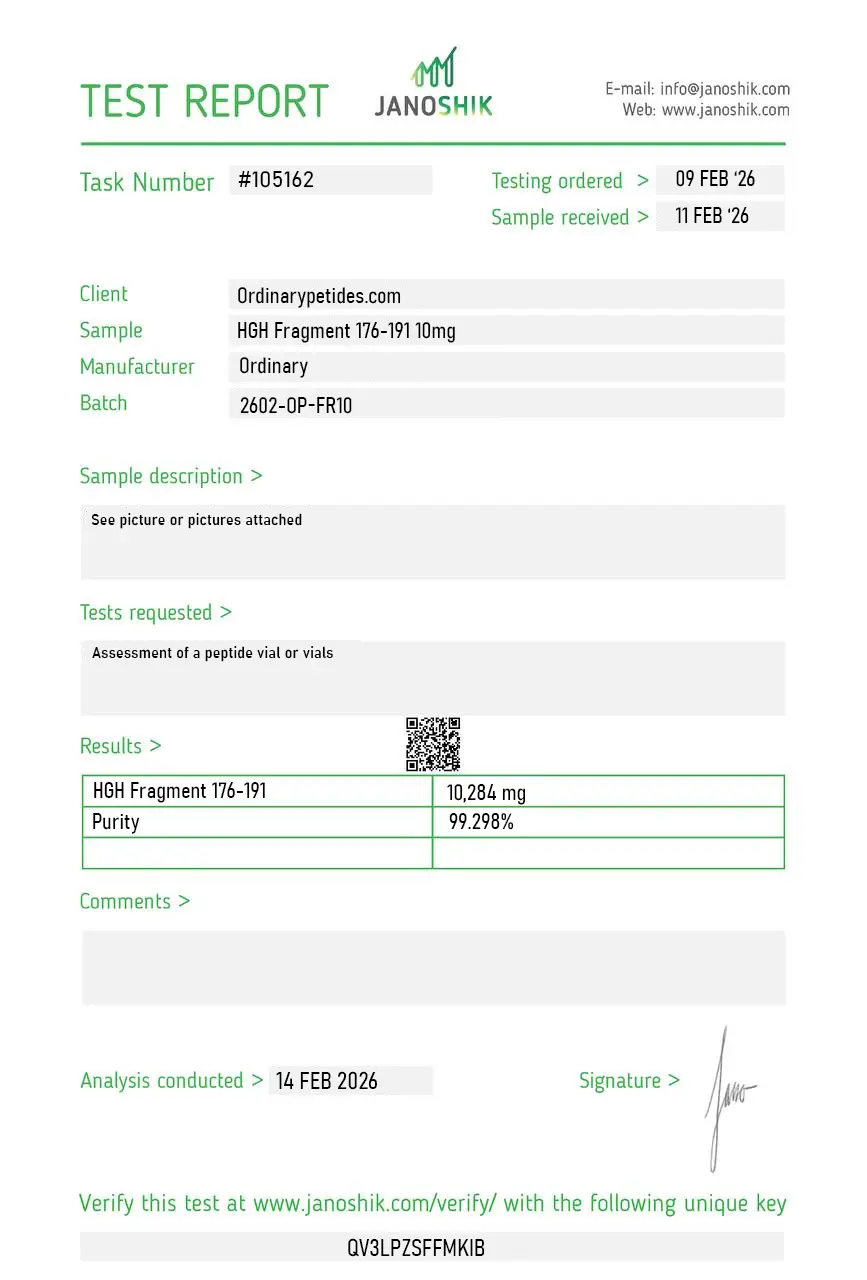
Certificate of Analysis
Independent test reports are available for HGH Fragment 176-191 standard, 2mg, 5mg, and 10mg batches. These reports provide batch-level documentation and analytical verification information for research reference.
Based on 1 reviews
5.0
The depot-selective lipolysis question is what we actually probe — published animal data suggests the fragment shows differential activity across abdominal versus visceral versus subcutaneous adipose depots, which is a more nuanced research question than "does it stimulate lipolysis." For mapping depot-specific responsiveness in primary adipocyte preparations from different anatomical sources, the fragment is a useful tool because the selectivity itself is the experimental object. The material gave reproducible differential responses across our depot-matched cultures.
Not exactly. They are very closely related, but they are not strictly identical in drug-development documents. AOD9604/LAT8881 is described as a modified form, while in commercial use the names are often treated as if they were the same.
No. It is not whole HGH or somatropin. It is a short fragment from the C-terminal region of human growth hormone.
Yes. It has been studied in both preclinical research and human clinical development programs, especially in obesity.
No. The available clinical evidence does not convincingly show meaningful weight loss in humans. The most important open clinical documents indicate that statistically significant weight-loss results were not demonstrated in obesity trials.
No. It is not FDA-approved for weight loss. Regulatory sources have also taken a cautious position on AOD9604 in the compounding context.
Because it has a very strong marketing narrative: a growth hormone fragment associated with fat loss, promoted as a way to support "cutting" without the full effects of HGH. That idea is highly marketable, even though the clinical evidence is much less impressive.
The key point is that HGH Fragment 176–191 is an interesting research peptide, but not a proven or recognized standard treatment for obesity or fat loss.
HGH Fragment 176-191 is a synthetic peptide corresponding to amino acids 176 through 191 of the 191-amino acid human growth hormone molecule — specifically the C-terminal region of the HGH sequence. It is also known as AOD9604 (Anti-Obesity Drug 9604), with AOD9604 being the pharmaceutical development name given to the stabilized version that adds a tyrosine residue at the N-terminus to improve stability (making it technically a 16-amino acid fragment spanning residues 177 to 191 with a tyrosine addition, often written as Tyr-hGH177-191). In common use the names HGH Fragment 176-191 and AOD9604 are used interchangeably in the research and wellness community, though there is a minor structural distinction — Fragment 176-191 refers to the raw sequence without modification while AOD9604 refers to the N-terminally modified pharmaceutical-grade version. Both refer to the same fundamental C-terminal lipolytic domain of HGH.
This fragment retains the portion of HGH responsible for fat metabolism while entirely lacking the portions responsible for growth promotion, IGF-1 stimulation, insulin resistance, and the anabolic effects of full HGH. Full HGH binds to the GH receptor and drives both its fat-metabolizing effects and its growth and anabolic effects through IGF-1. Fragment 176-191 does not bind the classical GH receptor — it does not stimulate IGF-1 production, does not promote tissue or organ growth, and does not cause insulin resistance or glucose intolerance. Instead it acts on adipocyte receptors linked to adenylate cyclase, increasing intracellular cAMP, activating protein kinase A, and stimulating hormone-sensitive lipase and adipose triglyceride lipase — directly breaking down stored triglycerides into free fatty acids. It simultaneously downregulates lipogenic enzymes reducing new fat storage. This targeted lipolytic mechanism without the systemic hormonal effects of full HGH is its defining characteristic.
Animal research produced impressive results. In obese mice chronic administration produced approximately 50% greater fat loss compared to controls with no diabetogenic effects. In obese rats the fragment specifically reduced abdominal and visceral fat while preserving lean body mass. Metabolic studies showed enhanced fatty acid oxidation and energy expenditure. In clinical development the compound completed six randomized, double-blind, placebo-controlled human trials involving over 900 participants — an unusually extensive human safety database for a research peptide. Safety results were consistently clean across all trials with no IGF-1 elevation, no glucose intolerance, no anti-peptide antibodies, and no genotoxicity detected. However the largest Phase IIb efficacy trial with 500 obese adults incorporating a structured diet and exercise regimen failed to demonstrate statistically significant weight loss versus placebo, leading Metabolic Pharmaceuticals to permanently terminate the obesity drug development program in 2007.
The preclinical signal was genuine and the mechanism is biologically sound. The failure was in clinical translation — a pattern common in obesity pharmacology where animal results rarely replicate faithfully in humans at the scale needed for regulatory approval. The compound does appear to have lipolytic activity, but the magnitude of this effect in the context of diet and lifestyle interventions in humans is insufficient to produce meaningful weight loss as a standalone therapy. It may offer modest additive benefit to a well-structured fat loss protocol, but claims of dramatic targeted fat loss are not supported by the clinical trial record. The FDA's 2023 Category 2 designation — reflecting insufficient evidence that the compound would be safe when used in compounded preparations — aligns with the overall picture of a compound with an interesting mechanism but unproven clinical utility.
It is given by subcutaneous injection, typically in doses of 250 to 500 mcg once or twice daily, with some protocols using injection near target fat areas though localized effects have not been reliably demonstrated in human studies. It is supplied as lyophilized powder reconstituted with bacteriostatic water. Some oral formulations exist — animal studies confirmed oral bioavailability, which is unusual for a peptide, and Phase II oral trials were conducted. Oral bioavailability is lower than injectable but demonstrable. It is commonly stacked with CJC-1295, Ipamorelin, or other GH secretagogues in performance and wellness protocols under the premise that combining upstream GH stimulation with a targeted lipolytic fragment maximizes body composition benefits, though no clinical evidence exists for this combination approach.
Fragment 176-191 / AOD9604 has the most favorable documented safety profile of any compound in this series — confirmed across six controlled human trials with over 900 participants. No serious adverse events were reported. No IGF-1 elevation, no glucose impairment, no insulin resistance, no antibody formation, no genotoxicity, and a side effect profile indistinguishable from placebo across all trials. Mild injection site reactions including redness and local discomfort are the most commonly reported effects in practice. The absence of IGF-1 stimulation means it does not carry the cancer promotion concern associated with full HGH or IGF-1 LR3, distinguishing it from most other compounds in the GH axis category.
Not FDA-approved for any therapeutic indication. The clinical development program was terminated in 2007 due to lack of efficacy rather than safety concerns. The FDA designated it a Category 2 bulk drug substance in 2023, meaning it cannot be legally compounded in the United States by pharmaceutical compounding pharmacies. It is banned by WADA under its prohibited list. Despite the regulatory status it remains widely available through research peptide vendors and some international wellness clinics. In Australia it is classified as a prescription-only substance by the TGA. Health Canada lists it as an unauthorized substance.
Competitive athletes subject to WADA anti-doping testing must avoid it as it is detectable and prohibited. Pregnant or breastfeeding women should not use it given the absence of safety data in these populations. People with active cancer should exercise caution despite the absence of IGF-1 stimulation — the angiogenic properties documented in some preclinical research remain a theoretical concern. People seeking it as a primary weight loss intervention should understand the clinical trial record does not support meaningful standalone fat loss efficacy. Anyone obtaining it through US compounding pharmacies after 2023 is receiving a product outside the legal framework — quality and purity cannot be assumed.





