
ACTH 1-39
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
ACTH 1–39: The Full-Length Corticotropin With a Multilayered Research Profile
ACTH 1–39 is the full 39-amino-acid form of corticotropin, one of the most extensively studied signaling peptides in endocrine biology. In a research context, it is valued for its dual profile: through MC2R, it triggered a steroidogenic response, while through other melanocortin receptors it demonstrated distinct immunomodulatory and anti-inflammatory effects.
In published observations and clinical scenarios, it has been studied especially actively in connection with the HPA axis, neuroimmune mechanisms, and inflammatory processes — in other words, this is not "just another peptide," but a genuinely multilayered model for studying several systems at once.
A further point of interest is that full-length ACTH 1–39 is biologically broader than the shortened ACTH 1–24: it has a more complete receptor profile and supports a different research rationale. If you need a peptide that, within a research framework, brings together endocrine signaling, the melanocortin system, and the neuroimmune context, ACTH 1–39 looks like a very substantial candidate.
ACTH 1-39 (Adrenocorticotropic Hormone / Corticotropin): A Scientific Review
Based on peer-reviewed literature and pharmacopoeial documentation — see References. Last updated: April 2026.
The Short Version
Adrenocorticotropic hormone (ACTH) is a 39-amino acid peptide hormone secreted by the anterior pituitary gland that governs cortisol production from the adrenal cortex — making it the master regulator of the human stress response and the central player in the hypothalamic-pituitary-adrenal (HPA) axis. The designation “ACTH 1-39” specifies the full-length natural molecule, distinguishing it from the clinically widely used synthetic fragment ACTH 1-24 (cosyntropin/tetracosactide), which retains full adrenal-stimulating activity and is the standard for the ACTH stimulation diagnostic test.
ACTH’s contemporary relevance in this series has three dimensions: it is a foundational peptide hormone for understanding adrenal and HPA axis physiology; it has approved pharmaceutical applications with a specific and instructive risk-benefit profile; and it has a documented history of use as a doping agent in professional cycling, where it was used for glucocorticoid-driven euphoria, reduced perceived exertion, and energy substrate mobilisation.
| At a glance | |
|---|---|
| Full name | Adrenocorticotropic hormone (ACTH); corticotropin |
| Length / MW | 39 amino acids; ~4,541 Da |
| Gene | POMC (proopiomelanocortin); chromosome 2p23.3 |
| Secretion site | Anterior pituitary corticotroph cells |
| Primary receptor | MC2R (melanocortin-2 receptor) — almost exclusively expressed in adrenal cortex |
| Primary biological action | Stimulates cortisol (and androgen) synthesis and secretion from adrenal cortex |
| Plasma half-life | 10–30 minutes |
| Normal plasma levels | 7.2–63.3 pg/mL (7:00–10:00 AM peak) |
| Pharmaceutical forms | H.P. Acthar Gel (porcine-derived ACTH 1-39); cosyntropin (synthetic ACTH 1-24) |
| WADA | ❌ Prohibited S2 (peptide hormone) |
Origins: The POMC Precursor
ACTH does not exist as a discrete molecule until it is cleaved from a larger precursor protein. The POMC (proopiomelanocortin) gene encodes one of the most remarkable precursor proteins in human biology: a single precursor processed differently in different tissues generates an entire family of biologically distinct hormones and neuropeptides.[13]
In anterior pituitary corticotroph cells: POMC → (PC1/3 cleavage) → ACTH (1-39) + β-lipotropin (β-LPH), which is further processed → β-endorphin (the endogenous opioid) + γ-lipotropin. In hypothalamus and skin (different processing by PC2): ACTH → α-MSH (the first 13 amino acids of ACTH, N-acetylated) + CLIP (ACTH 18-39).
This tissue-specific processing explains the characteristic hyperpigmentation of Addison’s disease: when cortisol is chronically low, feedback fails and ACTH rises dramatically → elevated ACTH is cleaved in skin to α-MSH → activates MC1R (the melanocortin-1/“tanning” receptor) → melanin production, particularly in sun-exposed areas, skin folds, and mucosal membranes.
Structure and Functional Domains
Human ACTH 1-39 sequence: Ser-Tyr-Ser-Met-Glu-His-Phe-Arg-Trp-Gly-Lys-Pro-Val-Gly-Lys-Lys-Arg-Arg-Pro-Val-Lys-Val-Tyr-Pro-Asn-Gly-Ala-Glu-Asp-Glu-Ser-Ala-Glu-Ala-Phe-Pro-Leu-Glu-Phe
Residues 1–13: The biological activity core; when N-terminally acetylated forms α-MSH and binds all melanocortin receptors. Residues 1–24: Retains full adrenal-stimulating activity of the complete molecule — the basis for cosyntropin. Residues 15–18 (Lys-Lys-Arg-Arg): The basic tetrapeptide cluster; removal of these four basic residues completely inactivates ACTH. Residues 25–39: Do not contribute to receptor activation but significantly extend plasma half-life by protecting the active N-terminal region from proteolysis. The biological activity of the ACTH molecule depends on its first 24 amino-terminal amino acids while fragments of less than 20 amino acids are completely inactive.[1]
ACTH is highly conserved in mammals — only amino acids 31 and 33 vary between higher mammals and primates. This conservation explains why porcine-derived ACTH (H.P. Acthar Gel) is pharmacologically active in humans.
The HPA Axis: ACTH in Context
ACTH is the second messenger in a three-tier neuroendocrine cascade. Level 1 (Hypothalamus): In response to stress, the paraventricular nucleus releases CRH (41 AA) into the hypothalamic-pituitary portal circulation; vasopressin (AVP) acts synergistically. CRH is also released in a circadian pattern, driving the morning ACTH and cortisol peak. Level 2 (Anterior pituitary): CRH binds CRH-R1 on corticotroph cells → Gs → cAMP → PKA → POMC transcription + stored ACTH secretion. ACTH pulses in a circadian rhythm: peak at 6–8 AM, nadir around midnight. Level 3 (Adrenal cortex): ACTH binds MC2R → Gs → cAMP → PKA → steroidogenesis (see below). Cortisol enters systemic circulation within minutes.[2]
Negative feedback: Cortisol feeds back at both pituitary (suppresses ACTH secretion and POMC transcription) and hypothalamus (suppresses CRH secretion) in a fast/slow dual loop: fast feedback (minutes) directly inhibits CRH and ACTH secretory responses; slow feedback (hours to days) reduces POMC gene transcription and CRH mRNA expression. This feedback loop is the basis of dexamethasone suppression testing and explains HPA axis suppression after prolonged glucocorticoid therapy.
Mechanism: How ACTH Stimulates Steroidogenesis
Acute effects (minutes)
ACTH acts by binding to MC2R cell surface receptors on adrenocortical cells, triggering conformational changes that stimulate adenylyl cyclase → increased intracellular cAMP → PKA activation. PKA rapidly: activates hormone-sensitive lipase (HSL) to release cholesterol from stored cholesteryl esters; activates SR-B1 to enhance LDL-cholesterol uptake from plasma; induces StAR protein (steroidogenic acute regulatory protein — the rate-limiting step for steroidogenesis, physically transferring cholesterol from the outer to the inner mitochondrial membrane); and activates P450scc (CYP11A1) on the inner mitochondrial membrane to convert cholesterol → pregnenolone, the committed step in steroidogenesis.[4]
Chronic effects (hours to days)
With sustained ACTH stimulation: upregulation of all steroidogenic enzyme gene expression (CYP11A1, CYP17A1, CYP21A2, CYP11B1, HSD3B2); adrenocortical hypertrophy and hyperplasia (explaining bilateral adrenal hyperplasia in ACTH-dependent Cushing’s disease); and increased VLDL and LDL receptor expression for long-term cholesterol substrate availability.
The steroidogenic cascade from ACTH to cortisol
Cholesterol → (CYP11A1) → Pregnenolone → (CYP17A1) → 17-OH-Pregnenolone → (HSD3B2) → 17-OH-Progesterone → (CYP21A2) → 11-Deoxycortisol → (CYP11B1) → Cortisol. In the zona reticularis, the same ACTH signal drives adrenal androgen synthesis: DHEA and androstenedione.
MC2R: The ACTH Receptor
The melanocortin-2 receptor (MC2R) is unique among the five melanocortin receptors in its extraordinary selectivity for ACTH — it binds only ACTH, not α-MSH, β-MSH, or any other melanocortin. The ACTH receptor (MC2R) is expressed almost exclusively in the cortex of the adrenal glands, where it regulates synthesis and release of glucocorticoids in response to pituitary ACTH. ACTH also has long-term effects on adrenal cell growth and differentiation. This near-exclusive adrenal expression explains why ACTH’s primary direct physiological action is steroidogenesis.
Disease States: When the HPA Axis Fails
Addison’s Disease (Primary Adrenal Insufficiency)
Destruction or dysfunction of the adrenal cortex → inadequate cortisol. Most commonly autoimmune (90% in Western countries); also TB, metastatic cancer, bilateral adrenal haemorrhage. ACTH levels: very high (feedback failure). Hallmarks: fatigue, weight loss, hypotension, hypoglycaemia, hyponatraemia, hyperkalaemia, and hyperpigmentation (excess ACTH → α-MSH → MC1R activation → melanin production). Definitive diagnosis: cosyntropin stimulation test. Treatment: lifelong hydrocortisone (± fludrocortisone); sick-day rules for stress dosing are essential to prevent adrenal crisis.
Cushing’s Disease (ACTH-Dependent Cushing’s Syndrome)
Pituitary ACTH-secreting adenoma (corticotropinoma) → chronic hypercortisolism. ACTH elevated or inappropriately normal despite cortisol excess (the tumour escapes normal feedback suppression). Hallmarks: central obesity, moon face, buffalo hump, purple striae, muscle wasting, hypertension, hyperglycaemia, osteoporosis, easy bruising, immunosuppression, psychiatric disturbance. Distinction from adrenal Cushing’s (ACTH-independent): in adrenal adenoma/carcinoma, autonomous cortisol production suppresses ACTH to very low levels. In pituitary Cushing’s, ACTH is inappropriately elevated. Ectopic ACTH syndrome: non-pituitary tumours (small cell lung cancer, carcinoid, medullary thyroid cancer, thymoma) secrete ACTH autonomously → very high ACTH → severe hypercortisolism that may not suppress even with high-dose dexamethasone.
Secondary Adrenal Insufficiency
Pituitary or hypothalamic failure → inadequate ACTH secretion → adrenal cortex atrophies. Most common cause: iatrogenic — chronic exogenous glucocorticoid therapy suppresses CRH → ACTH → adrenal atrophy. Abrupt discontinuation → adrenal crisis. ACTH levels: low or inappropriately normal. Key distinction from Addison’s: no hyperpigmentation (ACTH not elevated); aldosterone production usually preserved (regulated primarily by renin-angiotensin, not ACTH) — no hyperkalaemia.
Pharmaceutical Forms and FDA-Approved Indications
H.P. Acthar Gel (corticotropin repository injection)
Porcine pituitary-derived full 39-amino acid ACTH in a glycerol slow-release base. First approved 1952. Current manufacturer: Mallinckrodt ARD Inc. Price: raised from ~$40/vial to ~$28,000/vial circa 2013 — one of the most notorious pharmaceutical price-gouging cases in US history. FDA-approved indications include: infantile spasms (West syndrome); MS acute exacerbations; rheumatic disorders (RA, psoriatic arthritis, AS); collagen diseases (SLE, systemic dermatomyositis); severe dermatological conditions; allergic conditions; ophthalmic conditions; symptomatic sarcoidosis; and nephrotic syndrome.[5]
Cosyntropin (Cortrosyn / tetracosactide / Synacthen)
Synthetic ACTH 1-24. Cosyntropin is created by isolating the first 24 amino acids from the 39-amino acid ACTH peptide. The only FDA-labelled indication for cosyntropin in the US is diagnostic testing of adrenal function. A depot formulation (Synacthen Depot, zinc phosphate suspension) is not approved by the FDA and is available only through a compassionate-use programme; it is approved in the UK and Europe for therapeutic use in MS relapses, infantile spasms, rheumatic and collagen diseases, skin diseases, IBD, and nephrotic syndrome.[6]
The ACTH Stimulation Test (Cosyntropin Stimulation Test)
The gold standard for diagnosing primary adrenal insufficiency. Standard dose: 250 μg cosyntropin IV or IM at 9:00 AM. Measurement: Serum cortisol at 0, 30, and 60 minutes. Normal response: Peak cortisol ≥550 nmol/L (20 μg/dL) at 30 or 60 minutes. A subnormal response confirms adrenal insufficiency; high ACTH indicates primary (Addison’s); low ACTH indicates secondary (pituitary/hypothalamic) or iatrogenic. The low-dose test (1 μg) is more sensitive for partial adrenal insufficiency and secondary adrenal insufficiency (where the adrenal gland may respond to the supra-maximal 250 μg dose but would fail at physiological concentrations). The depot test (1 mg depot tetracosactide IM) distinguishes primary from secondary: in Addison’s, no cortisol rise at 6 hours; in secondary adrenal insufficiency, cortisol continues rising over 6–24 hours as the reversibly atrophied adrenal gland responds to sustained stimulation.
Key Therapeutic Application: Infantile Spasms (West Syndrome)
West syndrome — a triad of infantile spasms, hypsarrhythmia (chaotic high-amplitude EEG), and developmental regression — is among the most devastating infantile epilepsies, with onset typically at 3–12 months of age. ACTH has been used for infantile spasms since the 1950s. The mechanism is thought to involve CRH suppression in the developing brain (where CRH acts as a proconvulsant), direct CNS effects of ACTH fragments on melanocortin receptors, and cortisol-mediated modulation of GABAergic neurotransmission and neuroinflammation.
Secondary adrenal insufficiency risk: Three days after completion of ACTH therapy for West syndrome, basal cortisol, peak cortisol, and peak ACTH levels are all low. HPA axis recovery takes approximately as long as the treatment course. Stress-dose steroids and monitoring are required during this recovery period.[9]
ACTH as a Doping Agent
As of 2007, it was widely reported that tetracosactide had been used as an illegal performance-enhancing drug by professional cyclists, administered to increase the secretion of glucocorticoids by adrenal glands. The physiological rationale: supraphysiological cortisol produces euphoria, reduced perceived exertion, and a sense of well-being; cortisol has potent anti-inflammatory and analgesic effects allowing competition through pain and injury; cortisol-driven gluconeogenesis and lipolysis mobilise energy substrates during sustained effort; and cortisol upregulates adrenergic receptor expression, increasing epinephrine sensitivity. ACTH (as tetracosactide) was preferred over direct glucocorticoid injections in some doping contexts because producing endogenous cortisol rather than exogenous synthetic glucocorticoids made detection harder. ACTH was implicated in the 1998 Tour de France Festina affair and subsequently added to the WADA Prohibited List under S2, where it remains today. Detection is challenging given ACTH’s short half-life (10–30 minutes) and natural presence in plasma; anti-doping laboratories rely on indirect markers, diurnal cortisol profile abnormalities, and longitudinal athlete passport data alongside direct ACTH mass spectrometry.[11][12]
Comparison: ACTH 1-39 vs. Cosyntropin (ACTH 1-24)
| Feature | ACTH 1-39 (corticotropin) | ACTH 1-24 (cosyntropin/tetracosactide) |
|---|---|---|
| Length | 39 amino acids | 24 amino acids |
| Source | Porcine pituitary (H.P. Acthar Gel) | Synthetic |
| Plasma half-life | 15–30 minutes | 10–15 minutes |
| Adrenal-stimulating potency | Full agonist (reference) | Equal (per molar dose) |
| Immunogenicity | Higher (porcine origin) | Lower (shorter, fully synthetic) |
| US FDA therapeutic approval | ✅ Yes (H.P. Acthar Gel, multiple indications) | Diagnostic only |
| Cost per vial (US) | ~$28,000 (H.P. Acthar Gel) | ~$15–25 (cosyntropin diagnostic vial) |
Safety Profile
The adverse effects of ACTH therapy are essentially the adverse effects of supraphysiological glucocorticoid exposure, because ACTH stimulates adrenal cortisol production far above physiological levels during therapeutic use. Cushingoid features (prolonged use): moon face, central weight gain, striae, skin thinning, easy bruising, buffalo hump, hirsutism, osteoporosis. Metabolic: hyperglycaemia/steroid-induced diabetes; hyperlipidaemia. Immunological: increased infection susceptibility; reactivation of latent TB or herpes simplex; live vaccine contraindication. Cardiovascular: hypertension; sodium and water retention, oedema. Psychiatric: mood disturbance, insomnia, anxiety, acute steroid psychosis at high doses.
⚠️ HPA axis suppression (critical): Secondary adrenal insufficiency on dose reduction or cessation; duration of suppression correlates with duration of therapy; tapering protocol required; stress-dose steroid coverage during illness. Contraindications: Primary adrenocortical insufficiency (adrenal gland cannot respond); Cushing’s syndrome (already hypercortisolaemic); active systemic infection; acute psychosis; osteoporosis (relative); sensitivity to porcine proteins (H.P. Acthar Gel).
Common Misconceptions
“ACTH is a steroid.”
ACTH is a peptide hormone — a chain of 39 amino acids. It is not a steroid. The steroids (cortisol, DHEA) are what ACTH causes the adrenal gland to produce. This distinction matters clinically: ACTH exerts its effects by stimulating endogenous steroid synthesis.
“ACTH 1-39 and cosyntropin are different drugs.”
Pharmacologically, cosyntropin (ACTH 1-24) has identical adrenal-stimulating activity to ACTH 1-39. The differences are regulatory (H.P. Acthar Gel has broader US therapeutic approval), immunogenicity (cosyntropin is less immunogenic being shorter and synthetic), and cost.
“ACTH is safe because it just makes your body produce its own hormones.”
Endogenous cortisol at supraphysiological levels — however produced — has the same adverse effects as exogenous corticosteroids. Cushing’s syndrome, the pathological consequence of cortisol excess, is associated with fractures, infections, cardiovascular disease, and psychiatric disorders regardless of whether the cortisol is exogenous or endogenously overproduced.
Key Takeaways
- ACTH 1-39 is the endogenous master regulator of adrenal cortisol production and the central executive hormone of the HPA axis stress response. Its biology is fundamental to understanding the human response to stress, immune regulation, metabolism, and cardiovascular homeostasis.[1]
- The first 24 amino acids (cosyntropin/tetracosactide) contain all biological activity required for MC2R binding and full adrenal steroidogenesis. The C-terminal 25–39 residues contribute primarily to metabolic stability.
- ✅ ACTH has genuine and important FDA-approved therapeutic applications. Infantile spasms (West syndrome) is the most clinically critical — 80–84% cessation rate, a first-line treatment alongside prednisolone and vigabatrin. The price of H.P. Acthar Gel (~$28,000/vial) represents a serious access barrier without proportional pharmacological justification over cosyntropin.[8]
- ⚠️ The safety risks of ACTH therapy are substantial and identical in nature to supraphysiological glucocorticoid therapy — Cushingoid features, osteoporosis, immunosuppression, HPA axis suppression, and psychiatric effects with prolonged use. HPA axis recovery after ACTH therapy is predictable but requires monitoring and stress-dose steroid coverage during the recovery period.
- ⚠️ ACTH is WADA-prohibited at all times (S2) and has been documented as a doping agent in professional cycling. Its performance-enhancing appeal derives from cortisol’s euphoric, anti-fatigue, and analgesic properties at supraphysiological levels — a temporary performance gain at the cost of significant physiological disruption.[12]
References
Foundational Endocrinology
- StatPearls. Physiology, Adrenocorticotropic Hormone (ACTH). Reviewed December 1, 2025. NCBI Bookshelf NBK500031
- Endotext. ACTH Action on the Adrenals. NCBI Bookshelf NBK279118
- StatPearls. Physiology, Cortisol. Reviewed December 1, 2025. NCBI Bookshelf NBK538239
Mechanism
- ACTH Action in the Adrenal Cortex — From Molecular Biology to Pathophysiology. Frontiers in Endocrinology. 2017. PMC5467431
Pharmaceutical ACTH
- H.P. Acthar Gel and Cosyntropin Review: Clinical and Financial Implications. P&T Journal. PMC2697107
- Cosyntropin (Cortrosyn) prescribing information. Amphastar Pharmaceuticals. FDA approval 1970.
- Tetracosactide (Synacthen). EMA-approved prescribing information. Mallinckrodt. 2008.
West Syndrome / Infantile Spasms
- Effectiveness of ACTH in Patients with Infantile Spasms. Brain Sciences. 2022;12(2):254. (50-patient series; 84% spasm cessation with tetracosactide)
- Adrenocortical Function Recovery from Secondary Adrenal Insufficiency After ACTH Therapy in a Patient with West Syndrome. Yonago Acta Medica. 2024;67(2):169–175. PMC11128082
- UK Infantile Spasms Study (UKISS). Hormonal therapy vs. vigabatrin RCT. Lancet. Referenced in clinical pathway guidelines.
Doping Context
- Wikipedia. Adrenocorticotropic hormone (medication) — Doping use section. Citing press reports from 1998 Festina affair and 2007 cycling investigations.
- WADA Prohibited List 2024. S2: Peptide Hormones, Growth Factors, Related Substances and Mimetics — ACTH listed.
Structure and POMC Biology
- Harno E, Gali Ramamoorthy T, Coll AP, White A. POMC: The Physiological Power of Hormone Processing. Physiological Reviews. 2018;98(4):2381–2430.
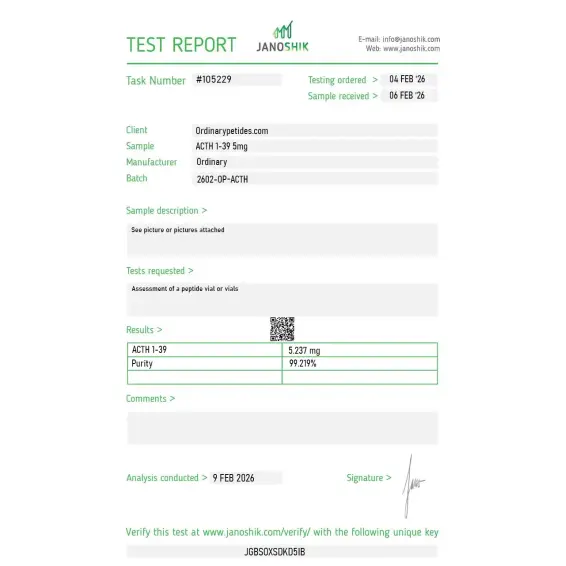
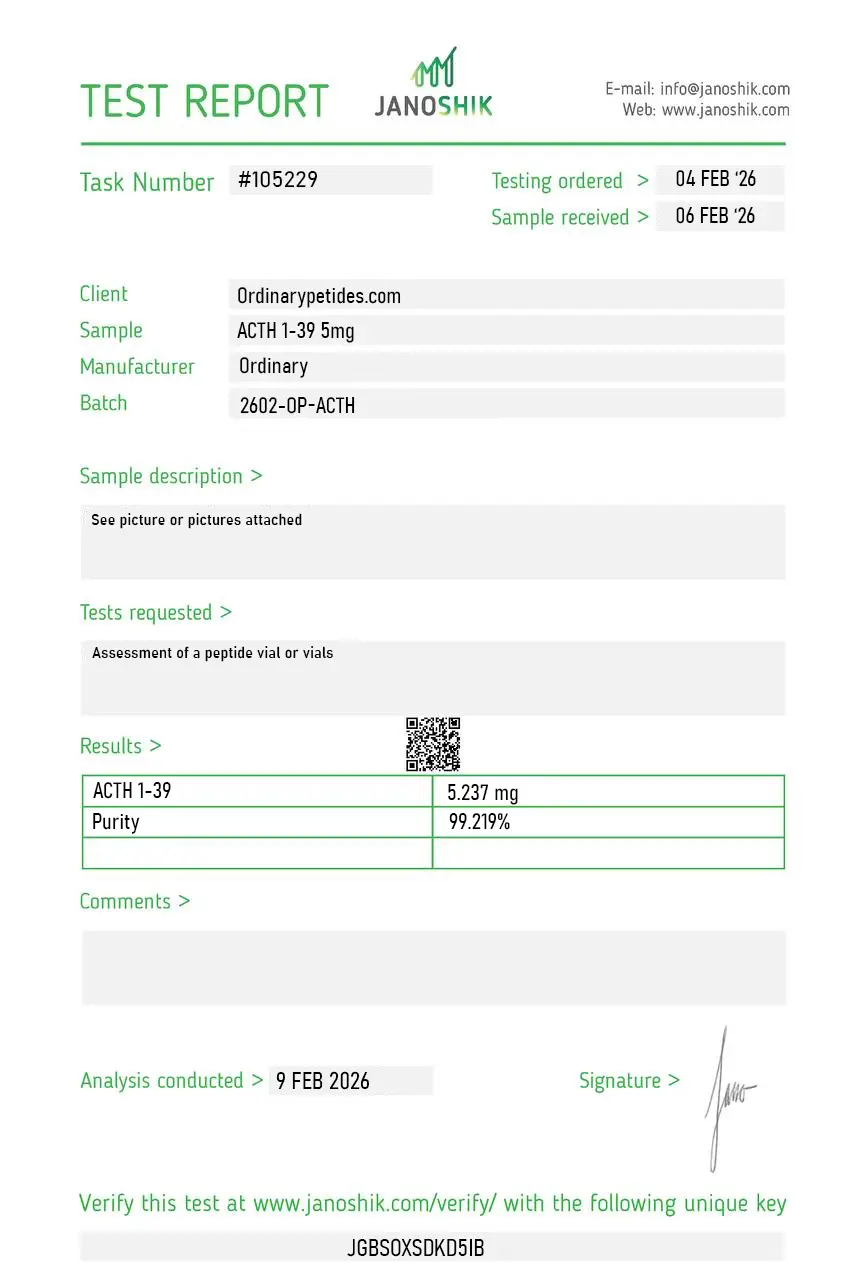
Certificate of Analysis
An independent test report is available for ACTH 1-39 5mg. This report provides batch-level documentation and analytical verification information for research reference.
Based on 1 reviews
5.0
The full 39-residue sequence is what makes this useful as a reference standard against the truncated ACTH 1-24 (cosyntropin) — for studying which residues beyond position 24 contribute to anything beyond receptor binding (binding affinity, plasma stability, immunogenicity), you need the complete native sequence as comparator. The supplier carrying both forms with matched documentation made the 1-39 vs 1-24 comparison feasible. Material gave consistent MC2R activation in our adrenal cortical cell assays.
ACTH 1-39 (Adrenocorticotropic Hormone) is the full-length, naturally occurring 39-amino acid peptide hormone produced and secreted by the anterior pituitary gland. It is derived from a larger precursor molecule called proopiomelanocortin (POMC), which also gives rise to alpha-MSH, beta-endorphin, and other biologically active peptides. ACTH 1-39 is the complete, unmodified form of corticotropin — the number refers to the full sequence of all 39 amino acids. Its biological activity resides primarily in the first 24 amino acids, which are identical across all mammalian species.
ACTH 1-39 binds to the melanocortin 2 receptor (MC2R) on adrenal cortex cells, triggering a G-protein signaling cascade that raises intracellular cAMP and activates enzymatic pathways leading to cortisol synthesis and secretion. This is the primary mechanism — stimulating the adrenal glands to produce glucocorticoids, particularly cortisol. It also influences adrenal androgen production including DHEA and androstenedione. Beyond the adrenal glands, ACTH binds to other melanocortin receptors found in the brain, immune cells, and other tissues, exerting cortisol-independent effects on neurological function, inflammation, and immune modulation.
ACTH is used both diagnostically and therapeutically. As a diagnostic tool, synthetic ACTH (cosyntropin) is the cornerstone of the ACTH stimulation test — used to assess adrenal gland function and diagnose conditions such as Addison's disease, adrenal insufficiency, and Cushing's syndrome. Therapeutically, it is FDA-approved and used to treat multiple sclerosis exacerbations, infantile spasms (West syndrome) — a severe form of epilepsy in infants — and certain inflammatory and autoimmune conditions. Its gel form (H.P. Acthar Gel) is a long-acting repository preparation used in these indications.
Research has shown that ACTH 1-39 has direct effects on the central nervous system independent of cortisol production. It promotes proliferation and differentiation of oligodendrocyte precursor cells — the cells responsible for myelin formation — which has implications for multiple sclerosis and white matter diseases. It also increases synaptic plasticity, enhances neuronal resilience, and protects oligodendrocyte precursors from excitotoxic and oxidative damage. These CNS effects are mediated through melanocortin receptors present in brain tissue rather than through adrenal stimulation.
Clinical ACTH preparations are given by intramuscular or subcutaneous injection. The standard diagnostic dose for the ACTH stimulation test is typically 250 micrograms of synthetic cosyntropin given as a single injection. For therapeutic use such as infantile spasms and MS exacerbations, H.P. Acthar Gel is administered intramuscularly or subcutaneously in protocols that vary by indication and are determined by a physician. ACTH levels in blood follow a natural circadian rhythm — peaking in the early morning and reaching their lowest around midnight — which is important for timing diagnostic tests.
Because ACTH stimulates cortisol production, many of its side effects mirror those of excess glucocorticoids. Common side effects include increased appetite, mood changes, fluid retention, elevated blood pressure, gastrointestinal upset, and insomnia. With prolonged use, excessive cortisol stimulation can lead to Cushing's syndrome — characterized by weight gain, bone loss, hyperglycemia, and immune suppression. Immune suppression itself increases susceptibility to infections. Adrenal gland overstimulation and HPA axis dysregulation are key concerns with long-term therapy.
It is contraindicated in people with active infections, particularly systemic fungal infections, as immune suppression from elevated cortisol significantly worsens outcomes. People with osteoporosis, uncontrolled hypertension, active peptic ulcers, or diabetes should use it with extreme caution and close monitoring. Pregnant women should avoid it unless the clinical benefit clearly outweighs the risk. Long-term use requires regular monitoring of blood pressure, blood glucose, bone density, and adrenal function by a qualified physician.





