


Melanotan 1 (MT1)
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Melanotan 1 (Afamelanotide): What It Is and How It Works
Melanotan 1, also known as afamelanotide, is a synthetic peptide that mimics the natural α-melanocyte-stimulating hormone (α-MSH) to activate the melanocortin 1 receptor (MC1R), boosting the production of eumelanin — a dark, photoprotective pigment in the skin. This molecule is approved in the EU and US under the brand name Scenesse specifically for treating erythropoietic protoporphyria (EPP), a rare condition that causes severe light sensitivity.
In clinical studies, afamelanotide has demonstrated its ability to help patients with EPP tolerate light exposure without pain, significantly improving their quality of life. However, its clinical use is limited to EPP, and it is not approved for cosmetic tanning or broad sun protection.
Despite its intriguing biological effects, using Melanotan 1 outside of its approved indication comes with risks and misunderstandings — especially when confused with unregulated "tanning peptides."
Melanotan 1 (MT-1) / Afamelanotide (Scenesse): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Melanotan 1 and afamelanotide are the same molecule: [Nle4,D-Phe7]-α-MSH, a 13-amino-acid synthetic analogue of the endogenous hormone α-melanocyte-stimulating hormone (α-MSH). This molecule was created in 1980 at the University of Arizona chemistry laboratory of Victor Hruby — one of the oldest research peptides in this entire series. It took 34 years from its synthesis to its first regulatory approval (EMA, 2014) and 39 years to its FDA approval (2019).[1]
The compound occupies an unusual position in the peptide landscape: it is genuinely FDA-approved — first-in-class for erythropoietic protoporphyria (EPP), an orphan disease that forces patients to avoid virtually all light exposure due to excruciating photo-induced pain. For these patients, Scenesse restored something they had never had: the ability to be outdoors in daylight. The same molecule circulates in an entirely parallel, unregulated market as “melanotan-1” sold online for cosmetic tanning — with no pharmaceutical oversight or validated dosing.
| At a glance | |
|---|---|
| Common names | Melanotan 1 (MT-1); afamelanotide; NDP-α-MSH; [Nle4,D-Phe7]-α-MSH; CUV1647 |
| Approved brand | Scenesse (afamelanotide, Clinuvel Pharmaceuticals) |
| Sequence | Ac-Ser-Tyr-Ser-Nle-Glu-His-D-Phe-Arg-Trp-Gly-Lys-Pro-Val-NH&sub2; |
| Modifications from α-MSH | Leu4→Nle4; Phe7→D-Phe7 |
| Class | Melanocortin 1 receptor (MC1R) agonist; tridecapeptide |
| Molecular weight | ~1,646 Da |
| Discovery | 1980 — University of Arizona (Hruby, Sawyer, Dorr, Hadley) |
| EMA approval | January 2015 (Scenesse) — EPP |
| FDA approval | October 8, 2019 (Scenesse) — EPP |
| Indication | Increasing pain-free light exposure in adults with EPP |
| Formulation (approved) | 16 mg subcutaneous slow-release PLGA biodegradable implant |
| Dosing schedule | Every 60 days (implant) |
| Not to be confused with | Melanotan II (MT-2) — different compound, different receptors, different effects |
| WADA | ❌ Prohibited (S4 — Hormone and Metabolic Modulators) |
Discovery: From University of Arizona Chemistry Laboratory to Approved Drug
Working in the chemistry laboratory of Victor Hruby at the University of Arizona, graduate student Tomi Sawyer created afamelanotide in 1980. The design goal was pharmacological: native α-MSH has a 2–3 minute half-life in plasma due to rapid proteolysis. The norleucine substitution at position 4 (replacing the oxidation-susceptible methionine) improved chemical stability. The D-phenylalanine substitution at position 7 conferred critical proteolytic resistance — D-amino acids are not substrates for most mammalian endopeptidases. The result was a peptide 100–1,000-fold more potent than native α-MSH with dramatically improved stability.[1]
In 1995, the University of Arizona licensed the drug to a Melbourne-based biotechnology start-up that initially planned to develop it as a tanning agent / injectable sunscreen. This plan was not favoured by regulatory agencies, and after strategic restructuring, the company (Clinuvel) chose to develop the drug as a treatment for EPP — a rare skin condition with no approved treatment and profound quality-of-life impairment. The orphan drug pathway, with its smaller required trial sizes and expedited review, made regulatory approval achievable. The EMA approved Scenesse in January 2015; the FDA followed in October 2019.[2]
The Melanocortin System: Biology Before Pharmacology
α-Melanocyte-stimulating hormone (α-MSH) is a 13-amino acid neuropeptide produced by post-translational processing of proopiomelanocortin (POMC) — the same precursor that produces ACTH and β-endorphin. The melanocortin receptor family (MC1R through MC5R) mediates the diverse effects of α-MSH and related peptides:
| Receptor | Primary location | Primary function |
|---|---|---|
| MC1R | Melanocytes, keratinocytes, immune cells | Melanogenesis (eumelanin), anti-inflammatory |
| MC2R | Adrenal cortex | ACTH-mediated cortisol production |
| MC3R | Hypothalamus, gut | Energy homeostasis |
| MC4R | Hypothalamus, brainstem | Appetite suppression, satiety |
| MC5R | Exocrine glands | Exocrine secretion |
Afamelanotide/MT-1 acts predominantly on MC1R. This receptor selectivity is the key pharmacological advantage over MT-2 (Melanotan II), which is a non-selective melanocortin agonist activating MC1R, MC3R, and MC4R. The MC4R activation by MT-2 produces CNS effects — appetite suppression, spontaneous erections — that afamelanotide does not produce at therapeutic implant doses.[3]
MC1R signalling and UV-independent melanogenesis
MC1R is a Gαs-coupled GPCR. Binding of α-MSH or afamelanotide activates adenylyl cyclase → elevated cAMP → PKA activation → phosphorylation of CREB and MITF → transcriptional upregulation of melanogenesis enzymes, particularly tyrosinase (the rate-limiting enzyme in melanin synthesis). The outcome is eumelanogenesis — preferential synthesis of brown-black eumelanin over yellow-red pheomelanin. Eumelanin absorbs broadly across UVA, UVB, and visible light wavelengths, scavenges free radicals, and acts as a neutral-density filter.[4]
Beyond melanogenesis, MC1R activation on fibroblasts, keratinocytes, and endothelial cells results in antioxidant activities, stimulation of DNA repair mechanisms, and immunomodulatory effects including IL-10 stimulation. Critically, afamelanotide stimulates melanogenesis without ultraviolet radiation. Normal tanning requires UV exposure — UV damages DNA, triggering a stress response that ultimately drives α-MSH production and delayed melanin synthesis 72–96 hours after the damage. Afamelanotide bypasses this entire cascade, producing photoprotective eumelanin within days, before any sun exposure. For EPP patients, this means photoprotective melanin can accumulate before entering the light that triggers their incapacitating pain.
Chemistry and Formulation
Afamelanotide’s sequence is: Ac-Ser-Tyr-Ser-Nle-Glu-His-D-Phe-Arg-Trp-Gly-Lys-Pro-Val-NH&sub2;. Compared to native α-MSH: position 4 Met is replaced by Nle (norleucine, removing the oxidation-prone sulfur while preserving hydrophobicity); position 7 Phe is replaced by D-Phe (D-stereochemistry resists protease cleavage while maintaining aromatic receptor contact). Both N-terminal acetylation and C-terminal amide — essential for receptor binding — are preserved from native α-MSH.
Native afamelanotide injected in saline has a plasma half-life of approximately 30 minutes. The Scenesse formulation is a biodegradable poly(lactic-co-glycolic acid) (PLGA) rod implant approximately 1.7 cm long and 1.45 mm in diameter — about the size of a grain of rice. PLGA degrades by hydrolysis, releasing the encapsulated peptide at a controlled rate. After subcutaneous implantation, the majority of the drug is released within two days, with 90% released by the fifth day; by the tenth day, no drug is detectable in plasma. The PLGA polymer fully biodegrades with no foreign material remaining after several weeks. Subcutaneous implants require implantation by a trained healthcare provider using a trocar needle — they cannot be self-administered.[8]
The Disease Context: What Is Erythropoietic Protoporphyria?
EPP is an inherited disorder of haem biosynthesis caused by mutations in the ferrochelatase (FECH) gene, encoding the enzyme that inserts iron into protoporphyrin IX (PPIX) to complete haem synthesis. Reduced ferrochelatase activity causes PPIX to accumulate. When PPIX in skin is exposed to visible light (particularly the Soret band around 400–420 nm), it absorbs photons and generates reactive oxygen species, producing immediate, intense phototoxic reactions.[5]
Unlike most photodermatoses triggered by UVA or UVB, EPP photosensitivity is triggered by visible light — including indoor fluorescent and LED lighting, sunlight through window glass, and operating theatre lighting. Standard sunscreens provide no protection. The sun-induced pain in childhood leads to an early and ingrained fear of sunlight. Patients modify their lives dramatically to minimise light exposure, wear protective clothing, or remain indoors — markedly affecting work, activities of daily living, and lifestyle choices from early childhood. Liver disease is a serious complication in a minority of patients due to high circulating PPIX levels causing hepatocellular damage.
Clinical Evidence
Phase 3 trials: the pivotal evidence
Two multicenter, randomised, double-blind, placebo-controlled Phase 3 trials were published in the New England Journal of Medicine (Langendonk et al., 2015). The European trial enrolled 74 patients; the US trial enrolled 94 patients. Both used 1:1 randomisation to afamelanotide or placebo implant every 60 days.[5]
European trial: Median total hours in direct sunlight without pain over 180 days: 64 hours (afamelanotide) vs. 41 hours (placebo) — a 56% increase in pain-free sunlight exposure. Statistically significant. US trial: Statistically significant increase in pain-free hours; median time in direct sunlight on a single day over the 270-day study period significantly favoured afamelanotide. Quality of life: The EPP-QOL questionnaire showed significant differences favouring afamelanotide in both trials for all questions.
Limitations: partial unblinding due to visible skin darkening in the afamelanotide group (unavoidable given the mechanism), and the observation that patients who did not develop visible tanning — whether on active drug or placebo — tended not to challenge sun exposure, likely underestimating the true treatment benefit.
Long-term observational study (Biolcati et al. 2015)
115 EPP patients treated across Italy over up to 8 years, totalling 314 patient-years and 1,023 implants. The study confirmed sustained efficacy and good long-term tolerability. No melanomas were observed. This represents the most extensive long-term safety data for the compound and is reassuring regarding the melanoma concern.[6]
Evidence summary
| Study | Design | N | Key outcome |
|---|---|---|---|
| CUV017 (Phase 3) [5] | RCT, EU | 74 | +23 hours pain-free sunlight (64 vs. 41 h) over 180 days |
| CUV039 (Phase 3) [5] | RCT, US | 94 | Significant pain-free hours increase; QoL improvement |
| Biolcati 2015 [6] | Long-term observational | 115 | 8 years, 314 patient-years; safety and efficacy confirmed; no melanomas |
Regulatory Status
| Jurisdiction | Status | Date |
|---|---|---|
| EMA (Europe) | ✅ Approved — prevention of phototoxicity in EPP (exceptional circumstances) | January 2015 |
| FDA (USA) | ✅ Approved — increase pain-free light exposure in EPP (first-in-class) | October 8, 2019 |
| TGA (Australia) | ✅ Approved — EPP | October 2020 |
| WADA | ❌ Prohibited — S4 (Hormone and Metabolic Modulators) | — |
The EMA approval was granted under “exceptional circumstances” — a pathway for conditions where standard Phase 3 trial sizes are not feasible due to disease rarity. The FDA’s “first-in-class” designation reflects that no prior drug had been approved that modulates melanocortin signalling for a therapeutic indication.
⚠️ A substantial parallel market exists in which “melanotan-1” is sold online for cosmetic tanning. Both Melanotan-I and Melanotan-II are commercially available without regulatory oversight. Illegal supply of unlicensed and unregulated products claiming to be Melanotan-I or Melanotan-II presents risks from potential chemical impurities and transmission of bloodborne diseases from needle sharing.[3]
Safety
From clinical trials (Scenesse formulation)
The overall safety profile across the clinical programme (800+ patients treated) is favourable, with no serious drug-related adverse events and no confirmed melanoma cases. Very common (>10%): nausea, headache. Common: fatigue, dizziness, somnolence, implantation site discolouration, skin hyperpigmentation including darkening of nevi and ephelides (expected pharmacological effect). Uncommon/rare: anaphylaxis (post-marketing reports; prescribers require training in emergency management).
The melanoma question: mechanistically reassuring
Melanoma arises from melanocyte stem cells in hair follicles, which do not express MC1R and therefore do not respond to α-MSH. Activating MC1R in differentiated skin melanocytes does not activate the cells from which melanoma arises. Furthermore, MC1R loss-of-function variants (fair skin, red hair, poor tanning) are associated with increased melanoma risk — the opposite of what would be expected if MC1R stimulation caused melanoma. Eight years of observational data in 115 EPP patients showed no melanomas.[6]
The Scenesse label nonetheless requires biannual full-body skin examinations to monitor nevi and other skin abnormalities, reflecting appropriate caution and the fact that the drug does cause visible darkening of pre-existing nevi.
Contraindications
Scenesse is contraindicated in: personal history of melanoma; dysplastic nevi syndrome; current or prior Bowen’s disease, BCC, SCC, or other malignant/premalignant skin lesions; pregnancy and lactation; age under 18 years.
Other Investigated Indications
Vitiligo: Phase 2 studies showed that afamelanotide combined with narrowband UVB phototherapy produced accelerated repigmentation compared to NB-UVB alone. NB-UVB stimulates undifferentiated melanoblasts in hair follicles to express MC1R; afamelanotide then drives these newly MC1R-expressing precursors to differentiate and migrate into depigmented areas. Phase 3 trials have been conducted or are recruiting.
Organ transplant recipients (actinic keratosis prevention): Immunosuppressed transplant recipients have dramatically elevated squamous cell carcinoma risk. Afamelanotide’s ability to induce photoprotective eumelanin without UV exposure was investigated as a chemopreventive strategy; early results were positive.
Xeroderma pigmentosum: Phase 2/3 trials underway. XP patients have defective nucleotide excision DNA repair and extreme UV sensitivity. Afamelanotide’s MC1R-mediated DNA repair stimulation and UV-independent melanin induction provide a dual theoretical rationale.
Comparison: MT-1 vs. Melanotan II
| Feature | MT-1 / Afamelanotide | Melanotan II (MT-2) |
|---|---|---|
| Structure | Linear tridecapeptide (13 AA) | Cyclic heptapeptide (7 AA) |
| Primary receptor | MC1R (selective) | MC1R + MC3R + MC4R (non-selective) |
| Tanning | ✅ Yes — eumelanin | ✅ Yes — eumelanin |
| Appetite suppression | ❌ No | Yes (MC4R) |
| Penile erections | ❌ No | Yes (MC4R, CNS) |
| Blood-brain barrier | Does not cross at therapeutic doses | Crosses BBB; CNS effects |
| FDA approval | ✅ Yes (Scenesse, EPP) | ❌ No |
| Molecular weight | ~1,646 Da | ~1,025 Da |
| WADA | ❌ Prohibited | ❌ Prohibited |
The non-selectivity of MT-2 is not merely a side-effect issue — MC4R agonism that drives erections and appetite suppression represents activation of hypothalamic circuits with significant neurological and cardiovascular implications. MT-2 has no approved indication anywhere and has a substantially more concerning safety profile than MT-1.
Common Misconceptions
“Online melanotan-1 has the same safety as Scenesse.”
⚠️ They are the same molecule but in profoundly different regulatory contexts. Scenesse is manufactured to pharmaceutical-grade standards, tested for purity and sterility, formulated in a validated slow-release implant, administered by a trained clinician, and the patient is monitored with biannual skin examinations. Online MT-1 has none of these safeguards. The molecule may be the same; the safety context is not.
“MT-1 is the same as MT-2 — just a different number.”
Pharmacologically distinct compounds. Different structures, different receptor profiles, different effects, different safety concerns. MT-2’s MC4R activation produces CNS effects that MT-1 does not. These are not interchangeable.
“Afamelanotide increases melanoma risk by activating melanocytes.”
Melanoma arises from melanocyte stem cells that do not express MC1R and do not respond to α-MSH. MC1R loss-of-function variants are associated with increased melanoma risk. Eight years of observational data in 115 treated EPP patients showed no melanomas.[6]
Frequently Asked Questions
Why is Scenesse given as an implant rather than an injection?
Native afamelanotide injected in saline has a ~30-minute plasma half-life, requiring daily injections for sustained melanogenesis induction. The PLGA implant provides sustained release over approximately 10 days — sufficient to drive continuous eumelanogenesis through an entire EPP treatment cycle. It also avoids the compliance and quality problems of daily self-injection with a highly potent peptide.
What is dersimelagon (MT-7117)?
An oral small-molecule MC1R agonist developed by Dermavant Sciences for EPP, currently in Phase 3 trials. Unlike afamelanotide (a peptide requiring subcutaneous implantation), dersimelagon can be taken as a daily tablet — potentially addressing the administration burden of Scenesse. If Phase 3 results are positive, it would represent a significant advance in EPP treatment.
Is MT-1 tested for in sports drug testing?
Yes. WADA prohibits afamelanotide/MT-1 under S4 (Hormone and Metabolic Modulators). Multiple validated test methods have been developed for detecting MT-1 in urine and blood samples, including UHPLC-HRMS in dried blood spots.
Key Takeaways
- Afamelanotide (Scenesse) is a genuine FDA-approved pharmaceutical — the first approved treatment for EPP, a debilitating orphan disease that prevents patients from tolerating normal daylight exposure. Its Phase 3 clinical trials showed a 56% increase in pain-free sunlight hours and significant quality-of-life improvement.[5]
- The 39-year journey from synthesis (1980) to FDA approval (2019) at the University of Arizona is a remarkable story of translational science — and a reminder of how long converting a compelling laboratory discovery into an approved therapeutic actually takes.
- MT-1/afamelanotide works by unique pharmacological mechanism — activating MC1R to drive eumelanogenesis without UV exposure. This produces photoprotective melanin before sun exposure, rather than the UV-dependent tanning that requires sun damage to initiate.
- ⚠️ MT-1 is fundamentally different from MT-2 (Melanotan II) — a distinction routinely obscured in the research peptide market. MT-1’s selectivity for MC1R avoids the CNS and reproductive side effects produced by MT-2’s MC4R activation. Confusing these compounds is a potentially significant clinical error.
- The melanoma safety concern is mechanistically unsubstantiated — melanoma stem cells lack MC1R; MC1R activation stimulates DNA repair and anti-inflammatory pathways; and eight years of long-term observational data showed no melanoma signals in treated EPP patients.[6]
- ⚠️ Online “melanotan-1” is the same molecule as Scenesse in an entirely different regulatory context. No pharmaceutical-grade quality assurance, no validated formulation, no medical oversight, and no equivalent to the biannual skin monitoring required in the Scenesse prescribing programme.
References
Discovery and Development
- Sawyer TK, Sanfilippo PJ, Hruby VJ, et al. 4-Norleucine, 7-D-phenylalanine-alpha-melanocyte-stimulating hormone: a highly potent alpha-melanotropin with ultralong biological activity. Proceedings of the National Academy of Sciences. 1980;77(9):5754–5758.
- Dorr RT. UA-discovered drug for skin disease approved for patients in Europe. University of Arizona Cancer Center. October 2014.
Biology and Pharmacology
- Afamelanotide. Wikipedia. en.wikipedia.org/wiki/Afamelanotide
- Afamelanotide in protoporphyria and other skin diseases: a review. PMC. 2024. PMC11110213
Clinical Evidence — EPP
- Langendonk JG, Balwani M, Anderson KE, et al. Afamelanotide for Erythropoietic Protoporphyria. New England Journal of Medicine. 2015;373(1):48–59.
- Biolcati G, Marchesini E, Sorge F, et al. Long-term observational study of afamelanotide in 115 patients with erythropoietic protoporphyria. British Journal of Dermatology. 2015;172(6):1601–1612. PMID: 25494545
- Fokkema T, et al. Afamelanotide for prevention of phototoxicity in erythropoietic protoporphyria. Expert Review of Clinical Pharmacology. 2021. doi: 10.1080/17512433.2021.1879638
Regulatory
- FDA Approval Package — Scenesse (afamelanotide) NDA 210797. October 2019. accessdata.fda.gov
Key Investigators
- Victor J. Hruby, PhD — University of Arizona; Regents Professor Emeritus of Chemistry and Biochemistry; principal investigator in the synthesis and structure-activity relationship work that produced afamelanotide; pioneer of melanocortin peptide pharmacology.
- Robert T. Dorr, PhD — University of Arizona Cancer Center; led the preclinical pharmacology and toxicology development of afamelanotide.
- Mac Hadley, PhD (deceased) — University of Arizona; contributed fundamental research on α-MSH biology and the melanocortin system that underpinned the drug discovery programme.
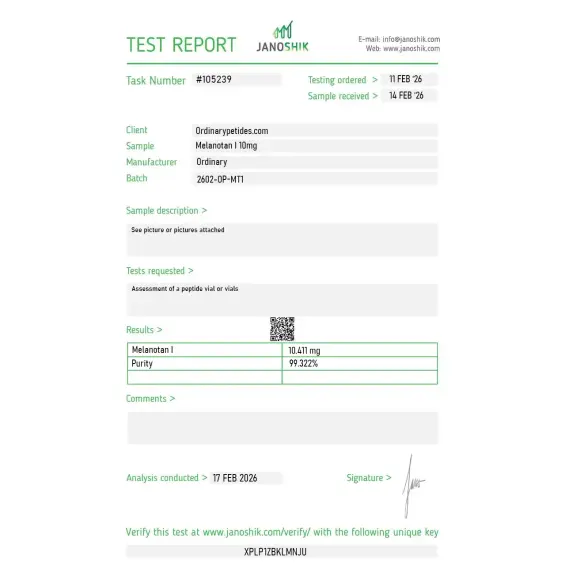
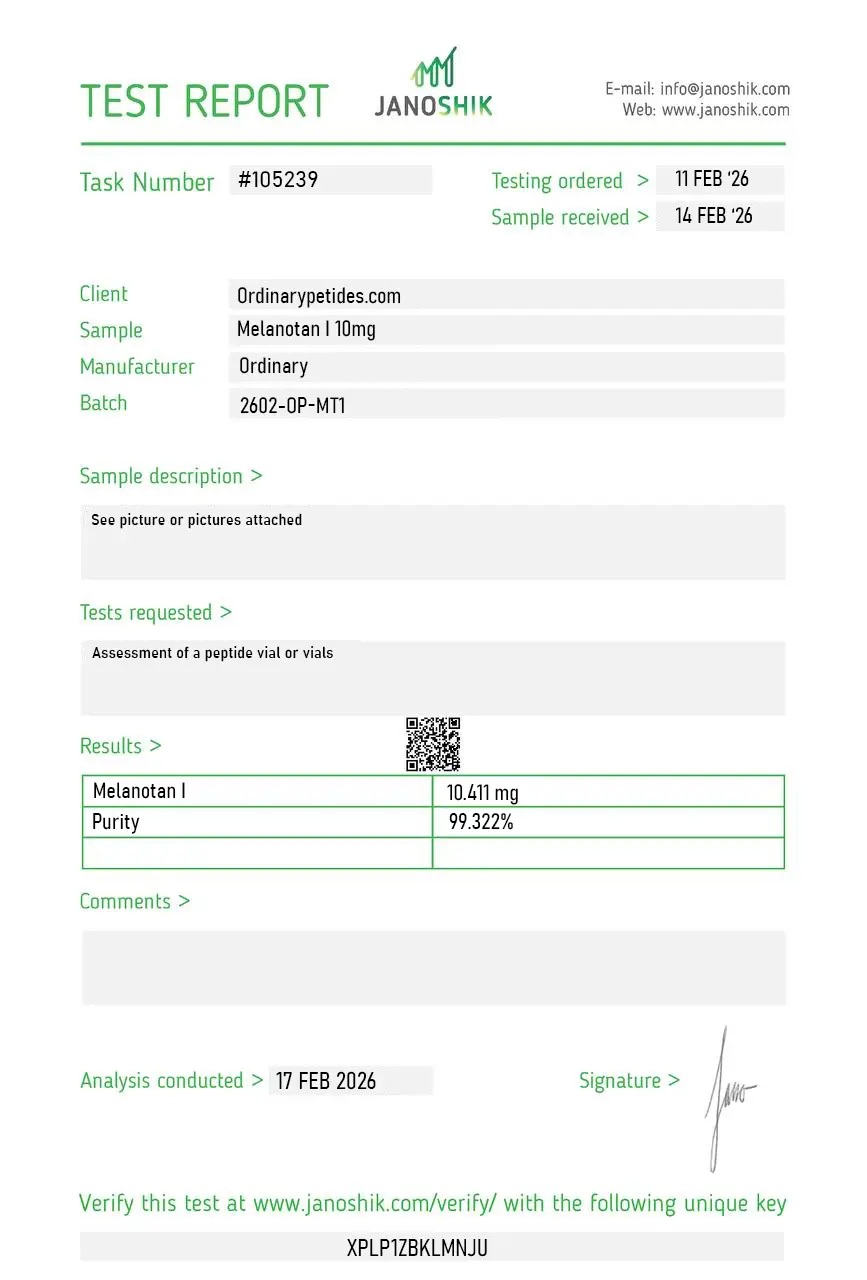
Certificate of Analysis
An independent test report is available for Melanotan I 10mg. This report provides batch-level documentation and analytical verification information for research reference.
Based on 1 reviews
5.0
The linear-13-residue architecture is the structural distinction from MT-II's cyclic heptapeptide, and worth understanding when ordering — MT-I retains the full α-MSH sequence backbone with only two substitutions (Nle-4 and D-Phe-7) for stability, while MT-II compressed and cyclized the same active region into seven residues. For studying how length-and-cyclization decisions shape melanocortin receptor engagement, MT-I is the linear-extended-sequence reference point. The material delivered the expected MC1R-preferring activation in our receptor assays.
Yes. Afamelanotide is a synthetic thirteen-amino-acid peptide, a structural analog of α-MSH.
Essentially yes: Melanotan 1 is the historical/informal name, while afamelanotide is the international nonproprietary name of the approved molecule.
Yes, but only as Scenesse and only for adult patients with EPP within the approved indication.
There is a clinical signal of benefit in combination with NB-UVB, but that is not equivalent to a broad approved indication
That description is misleading. It reflects the popular everyday use of the name, but poorly describes the evidentiary and regulatory reality of afamelanotide.
MT1/afamelanotide is a real, existing, and approved peptide drug, but its proven clinical value today relates primarily to erythropoietic protoporphyria, not cosmetic tanning or "universal photoprotection."
Melanotan 1 (MT-1) is the original research name for afamelanotide — a synthetic 13-amino acid tridecapeptide and structural analog of alpha-melanocyte stimulating hormone (α-MSH), with the sequence Ac-Ser-Tyr-Ser-Nle-Glu-His-D-Phe-Arg-Trp-Gly-Lys-Pro-Val-NH₂. It was developed in the 1980s at the University of Arizona as a more potent and proteolytically stable version of endogenous α-MSH — originally as a sunless tanning agent. It was later developed by the Australian company Clinuvel Pharmaceuticals and brought to clinical approval as Scenesse for a rare genetic disorder. Pharmaceutical afamelanotide (Scenesse) received EMA approval in 2014, FDA approval in October 2019, and TGA approval in 2020 — making it a first-in-class approved peptide drug. Unregulated "Melanotan 1" or "MT-1" products sold online as tanning peptides represent a completely different and legally problematic category from the approved pharmaceutical.
MT-1 / afamelanotide binds to and activates melanocortin receptors — primarily MC1R (melanocortin-1 receptor) on melanocytes in the skin, but also MC3R, MC4R, and MC5R to varying degrees. MC1R activation increases intracellular cyclic AMP (cAMP), which activates downstream signaling including MITF (microphthalmia-associated transcription factor) and the key melanogenic enzyme tyrosinase, dramatically increasing eumelanin production and skin darkening even without UV exposure. Crucially eumelanin — the darker brown-black melanin form — provides significantly more UV and visible light protection than pheomelanin (the lighter reddish form). In EPP patients this increased eumelanin acts as a natural photoprotective filter, absorbing the visible light wavelengths that excite protoporphyrin IX and cause the characteristic severe phototoxic pain. Beyond pigmentation, MC1R activation also promotes DNA repair in keratinocytes, reduces reactive oxygen species, and modulates inflammation.
EPP is a rare autosomal dominant genetic disorder caused by partial deficiency of the enzyme ferrochelatase, leading to accumulation of protoporphyrin IX in red blood cells, plasma, and skin. Protoporphyrin IX is a photosensitizer activated by visible light wavelengths around 400 to 420 nm — meaning EPP patients experience severe burning pain within minutes of sun or bright indoor light exposure. The pain lasts for days, is unresponsive to analgesics, and is followed by erythema, edema, and skin erosions. The condition is profoundly life-limiting — patients must avoid sunlight entirely, wear protective clothing year-round, and are often unable to participate in normal social and occupational activities. Afamelanotide's ability to increase eumelanin density provides a natural photoprotective barrier that substantially reduces protoporphyrin IX excitation, dramatically increasing the time patients can tolerate light exposure without pain. In Phase 3 clinical trials it significantly increased pain-free direct sun exposure compared to placebo. Clinicians report it is substantially more effective in clinical practice than the trial data suggest.
The pharmaceutical Scenesse formulation is a bioresorbable subcutaneous implant — a small rod approximately 1.7 cm long containing 16 mg of afamelanotide — inserted under the skin of the lower abdomen by a healthcare professional using a trocar. After implantation approximately 90% of the drug is released within five days and is undetectable in plasma by day ten. The implant is biodegradable and does not need to be removed. Up to four implants per year are approved at 60-day intervals, though clinical experience suggests some EPP patients need more frequent treatment. The short plasma half-life of approximately 30 minutes after release is offset by the sustained release depot formulation. This is a completely different route and formulation from the injectable research peptide versions sold online.
Beyond EPP, afamelanotide is in active clinical trials for vitiligo — where it promotes repigmentation, particularly when combined with narrowband UVB phototherapy — polymorphous light eruption, solar urticaria, xeroderma pigmentosum, variegate porphyria, and acne vulgaris where it reduced inflammatory lesion count in a Phase 2 trial. Research also documents secondary beneficial effects on mood and quality of life in treated EPP patients. Additional exploratory research has examined anti-inflammatory, metabolic, and neurological effects through MC3R, MC4R, and MC5R signaling.
In clinical trials the most common adverse events were headache, fatigue, and nausea, each affecting more than 10% of patients. Flushing, implant site reactions, and temporary darkening of existing pigmented lesions including moles occurred. The most clinically relevant safety signal is skin — afamelanotide intensifies existing freckles and moles, can darken existing nevi, and reports of eruptive melanocytic nevi and new mole formation following use have been published. This raises theoretical concern about melanoma promotion in susceptible individuals, though no causal relationship with melanoma has been established in clinical trial populations. Post-authorization safety monitoring is ongoing through mandated registry studies.
This is a distinct and considerably more concerning category. Unregulated MT-1 products sold online as injectable tanning agents, nasal sprays, or research chemicals are manufactured without pharmaceutical quality control, carry unknown purity and potency, and are associated with nausea, vomiting, stomach cramps, flushing, fatigue, yawning, spontaneous erections, changes in mole shape and color, new mole formation, and documented cases of melanoma in users. The nevi and melanoma concern is particularly serious — people with fair skin using unregulated MT-1 face real risk of pathological mole changes. These products are illegal to sell in most jurisdictions without a prescription, are not equivalent to pharmaceutical Scenesse, and should not be used.
Anyone with a personal or family history of melanoma or atypical nevi should not use it. People with any pre-existing pigmented lesions should have baseline dermatological evaluation and monitoring if using pharmaceutical afamelanotide. Pregnant or breastfeeding women should not use it. Anyone considering unregulated online products should understand these are illegal in most jurisdictions, carry serious dermatological risks, and are not equivalent to the approved pharmaceutical. The entire category of self-administered cosmetic tanning use represents an unacceptable risk-benefit profile given the mole and melanoma signals.





