

PT-141
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
PT-141 (Bremelanotide): Not "a Peptide for Everyone," but a Targeted Melanocortin Tool
PT-141, also known as bremelanotide, is a cyclic heptapeptide from the melanocortin line that became interesting not as a "universal aphrodisiac," but as a molecule with a central rather than vascular mechanism of action. In both research and clinical contexts, it has been linked primarily to modulation of melanocortin receptors, especially along the MC4R line — that is, to the neurobiology of sexual desire rather than simply to mechanical enhancement of sexual function.
In published clinical data in premenopausal women with acquired, generalized HSDD, the drug showed statistically significant, but on average moderate, improvement in measures of desire and the associated distress. At the same time, the story of PT-141 is not about an "easy solution without trade-offs": the same data frequently noted nausea, vascular effects, and a risk of hyperpigmentation.
That is why PT-141 is interesting not as a loud wellness symbol, but as a rare example of a peptide that actually made it to approval while remaining very narrow in indication and fairly demanding in terms of tolerability. For a client, this is exactly the kind of case where attention is drawn not by hype, but by the fact that behind the molecule there is real pharmacology, real clinical data, and far less magic than people on the internet like to promise.
PT-141 (Bremelanotide / Vyleesi): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
PT-141 — bremelanotide — is the rarest kind of compound in the peptide research world: it made it all the way through. Phase 1, Phase 2, Phase 3, FDA review, commercial approval. It is the only on-demand, centrally-acting, peptide-based treatment for a disorder of sexual desire approved anywhere in the world. In that sense, it is the most clinically validated peptide in this entire series.
Its story begins in a university laboratory studying tanning peptides. The sexual arousal effects of Melanotan II (MT-2) were discovered when Mac Hadley accidentally self-administered twice his intended dose, triggering prolonged erection, nausea, and vomiting. That accidental discovery led to a commercial licensing deal, a chemical modification (removing the C-terminal amide and replacing it with a hydroxyl, converting MT-2 from a cyclic compound to what was designated “a likely metabolite”), and eventually bremelanotide — PT-141 — as a distinct pharmacological entity developed by Palatin Technologies.
The Phase 3 RECONNECT programme enrolled 1,267 premenopausal women with HSDD across two identical trials. Both coprimary endpoints were met: significant improvements in sexual desire (FSFI-D) and significant reductions in desire-related distress (FSDS-DAO).[2] The number of satisfying sexual events per month did not reach statistical significance as a secondary endpoint. Effect sizes were modest. Nausea affected 40% of users on the first dose.
| At a glance | |
|---|---|
| INN | Bremelanotide |
| Brand name | Vyleesi (Palatin Technologies) |
| Research designation | PT-141 |
| Type | Synthetic cyclic heptapeptide |
| Molecular weight | ~1,025 Da |
| Receptor targets | MC4R (primary), MC3R (secondary); does NOT activate MC1R at therapeutic doses |
| Parent compound | Derived from Melanotan II (MT-2) — differs at C-terminus (OH vs. NH&sub2;) |
| FDA approval | ✅ June 21, 2019 |
| Approved indication | Acquired, generalised HSDD in premenopausal women |
| Approved dose | 1.75 mg SC injection ≥45 minutes before sexual activity; max 1 dose/24 hours |
| NOT approved for | ⚠️ Men; postmenopausal women; performance enhancement |
| EMA status | ❌ Not approved |
| Plasma half-life | ~2.7 hours |
| Onset of action | 45–60 minutes |
The Developmental History: From Tanning to Desire
Melanotan II and the accidental discovery
The complete MT-2 developmental history is covered in the MT-2 article in this series. The essential points: Melanotan II was developed at the University of Arizona in the 1980s–1990s as a non-UV tanning agent. Its sexual effects were discovered accidentally when Mac Hadley self-administered twice the intended dose. Subsequent Phase 1 trials showed that 9 of the first 10 male volunteers experienced spontaneous erections after MT-2 injection, confirming that the sexual arousal effect was pharmacological, not coincidental. MT-2 was licensed to Palatin Technologies for sexual dysfunction development.
The bremelanotide distinction
Palatin synthesised bremelanotide as what they designated a likely metabolite of Melanotan II. The structural difference is small but pharmacologically meaningful: the C-terminal amide (–NH&sub2;) of MT-2 is replaced by a hydroxyl group (–OH) in bremelanotide. The cyclic structure and core pharmacophore responsible for MC4R activation are retained. This modification created a distinct chemical entity for independent patent protection and altered the receptor affinity profile modestly — bremelanotide has somewhat lower MC1R activity relative to MC4R compared to MT-2, reducing the tanning liability for a sexual dysfunction indication.
The intranasal route and the blood pressure problem
Initial bremelanotide development used intranasal administration. Phase 2 intranasal trials showed efficacy in both men (erections) and women (sexual arousal). However, intranasal administration produced consistent, clinically significant blood pressure increases — systolic BP rising 6–8 mmHg — that were sustained and problematic from a regulatory safety standpoint. Palatin’s solution: switch from intranasal to subcutaneous injection. The SC route produces slower absorption and lower peak concentration, substantially attenuating the blood pressure effect. This route switch allowed development to continue but changed the user experience — from a nasal spray to a self-administered injection pen.
Structure and Pharmacology
Molecular structure
Bremelanotide is a synthetic cyclic heptapeptide: Ac-Nle-cyclo[Asp-His-D-Phe-Arg-Trp-Lys]-OH. The ring is formed by a lactam bond between the side chains of Asp and Lys. The D-Phe substitution at position 7 is critical for high-potency MC receptor activation; the C-terminal hydroxyl distinguishes bremelanotide from MT-2 (C-terminal amide); and Nle substitution at position 4 (replacing methionine) improves stability.
Receptor pharmacology
MC4R (primary target; Ki ~0.16 nM): highest affinity within the melanocortin family; drives the pro-sexual CNS effects. MC3R (secondary; Ki ~7.5 nM): co-activation contributes to effects on energy balance and reward. MC1R: activated at higher concentrations, responsible for pigmentation effects that can occur with repeated use — less pronounced than with MT-2 at the approved dose. MC2R: minimal activity — does not meaningfully stimulate the adrenal axis at therapeutic doses.
Pharmacokinetics
After SC injection of 1.75 mg: Tmax ~1 hour; Cmax ~4.3 ng/mL; half-life ~2.7 hours; bioavailability ~100% (complete SC absorption); protein binding ~21%; metabolism via non-specific aminopeptidases (no significant CYP450 involvement — minimal drug-drug interactions through enzymatic pathways); excretion primarily renal (~64% of dose recovered in urine as metabolites).[1]
Mechanism of Action: Central, Not Peripheral
The paraventricular nucleus (PVN) and adjacent hypothalamic structures are the primary anatomical locus of bremelanotide’s pro-sexual effects. MC4R is densely expressed in the PVN, where it modulates oxytocin neurons projecting to the limbic system, spinal cord sexual function centres, and the autonomic nervous system. When bremelanotide activates PVN MC4R: oxytocin is released from PVN neurons projecting to limbic and brainstem sites; dopamine release in the mesolimbic reward pathway increases, enhancing motivation and desire; descending pathways to the sacral spinal cord sexual function centres are activated, facilitating arousal; and nitric oxide synthase activity in the PVN increases, mediating some downstream pro-arousal effects through a CNS-mediated mechanism.[7]
Distinction from PDE5 inhibitors: Sildenafil and tadalafil act peripherally in the corpus cavernosum and genital vasculature — preventing cGMP degradation in smooth muscle → vasodilation → increased blood flow. They require sexual stimulation for nitric oxide release and do not address desire or motivation. Bremelanotide acts centrally in the hypothalamus, activating the neural circuits that generate desire and initiate arousal before any peripheral vascular response — producing arousal independent of direct genital stimulation, and potentially facilitating erection through central mechanisms even when peripheral vascular response is compromised.
Approved Indication: HSDD in Premenopausal Women
Hypoactive Sexual Desire Disorder is persistently or recurrently deficient or absent sexual fantasies, thoughts, and desire for sexual activity, causing marked personal distress or interpersonal difficulty, and not better accounted for by another medical, psychiatric, or relationship condition. HSDD is the most common female sexual dysfunction, affecting an estimated 8–10% of premenopausal women with associated distress. The FDA-approved indication is specifically acquired (developed in a patient who previously had normal sexual desire), generalised (across all contexts, types of stimulation, and partners — not situational), and in premenopausal women. Before bremelanotide’s 2019 approval, flibanserin (Addyi, 2015) was the only FDA-approved pharmacotherapy, requiring daily dosing and carrying significant limitations.
Phase 3 Evidence: The RECONNECT Trials
Study design
Two identical Phase 3 RCTs (Studies 301 and 302) constituted the RECONNECT programme: 1,267 premenopausal women aged ≥18, with acquired generalised HSDD of ≥6 months’ duration, in stable monogamous relationships; 24-week double-blind treatment with bremelanotide 1.75 mg SC vs. placebo, self-administered as-needed ≥45 minutes before sexual activity (maximum 1 dose/24 hours; maximum 12 doses/month); mean age 39 years; 85.6% white; 96.6% from US sites.[2]
Coprimary endpoints — both met
Women taking bremelanotide had statistically significant increases in sexual desire (FSFI-D: integrated mean improvement 0.35 points, p<0.001) and statistically significant reductions in distress related to low sexual desire (FSDS-DAO Item 13: mean reduction 0.33 points, p<0.001) compared with placebo. The pre-established minimal clinically important difference (MCID) for FSFI-D was 0.6 points — meaning the mean treatment difference of 0.35 falls below the MCID. The FDA accepted this as approvable based on responder analyses and the distress endpoint.
The secondary endpoint complication
⚠️ The number of satisfying sexual events per month — arguably the most intuitively meaningful clinical outcome — did not significantly improve on bremelanotide vs. placebo (integrated: bremelanotide 0.0, placebo −0.1, p=0.630). Per the pre-specified hierarchical statistical analysis plan, this failure ended formal testing of subsequent ranked secondary endpoints.[2]
A post hoc analysis reframed the question: the proportion of sexual encounters that were satisfying increased substantially in the bremelanotide group compared with placebo (25.0% vs. 9.8%, p<0.001). This reframing — from absolute events to proportion of satisfying events — provided a more favourable picture but was not a pre-specified analysis and should be interpreted with appropriate caution.
Long-term extension (52 weeks)
Of the 856 eligible patients who completed the core phase, 684 elected to participate in the open-label extension and 272 completed it. Efficacy was maintained through 52 weeks, with further improvements in FSFI-D and FSDS-DAO scores. The most common treatment-emergent adverse events were nausea (40.4%), flushing (20.6%), and headache (12.0%). The only severe treatment-emergent adverse event experienced by more than one participant was nausea.[3] Important limitation: the open-label extension enrolled only those who completed the core phase, introducing selection bias toward responders and tolerators.
Safety Profile
Common adverse events
| Adverse event | Bremelanotide (%) | Placebo (%) |
|---|---|---|
| Nausea | ~40% (first dose) | ~1% |
| Flushing | ~20% | <5% |
| Headache | ~11% | ~7% |
| Injection site reactions | Common | N/A |
| Vomiting | ~5% | <1% |
Nausea is dose-dependent and peaks with the first dose; many users report it diminishes with subsequent use. Pre-medicating with antiemetics (e.g., ondansetron) is commonly used in practice. Approximately 10% of women discontinued in the RECONNECT trials due to nausea.[6]
Cardiovascular: blood pressure
⚠️ Bremelanotide consistently produces a transient, dose-dependent increase in blood pressure (mean maximum increase ~6–8 mmHg systolic, occurring 4–8 hours post-dose) with compensatory decrease in heart rate. There is no evidence of any cumulative or sustained effects on BP with repeated dosing. However, Vyleesi is contraindicated in patients who have uncontrolled hypertension or known cardiovascular disease, and is not recommended in patients at high risk for cardiovascular disease. Blood pressure should be well-controlled before initiating treatment.[1]
Pigmentation changes
Because bremelanotide activates MC1R at higher plasma concentrations, skin hyperpigmentation — particularly darkening of existing moles, facial skin, and breasts — can occur with repeated use. This is not a melanoma risk signal but a cosmetic concern that should be monitored. The FDA advises patients to report new or worsening skin darkening to their clinician.
Pregnancy
Based on animal reproductive studies, bremelanotide may cause foetal harm. Women must use effective contraception while taking Vyleesi. Bremelanotide is not recommended during pregnancy or breastfeeding.
Off-Label Use in Men
Before the pivot to HSDD in women, bremelanotide was extensively studied for male erectile dysfunction. Rosen et al. (2004): SC PT-141 in men with inadequate response to Viagra showed significant improvements in erectile rigidity in early trials.[5] A study in sildenafil-resistant men (N=180) found 62% improvement in PT-141-treated men vs. 21% placebo — a significant result in a population that had failed first-line therapy. No large-scale Phase 3 trial in men has been completed.
The rationale for bremelanotide in men, and particularly in combination with PDE5 inhibitors, is mechanistically coherent: bremelanotide activates central desire and arousal circuits (MC4R → dopamine → desire), while PDE5 inhibitors facilitate peripheral vascular response. The two mechanisms are complementary and do not overlap, suggesting synergistic potential in the approximately 40% of ED patients who do not respond adequately to PDE5 inhibitors alone. A 2024 Phase 2 clinical study by Palatin examined this combination. Off-label prescribing in men is legal in the US under physician direction, typically through compounding pharmacies.
Comparison with Flibanserin (Addyi)
| Feature | Bremelanotide (Vyleesi) | Flibanserin (Addyi) |
|---|---|---|
| Mechanism | MC4R agonist (central, dopamine/oxytocin) | 5-HT1A agonist + 5-HT2A antagonist (daily CNS modulator) |
| Dosing | On-demand (before sexual activity) | Daily (regardless of sexual activity) |
| Route | SC injection | Oral tablet |
| Alcohol interaction | No restriction | ⚠️ Severe — alcohol contraindicated (hypotension/syncope risk) |
| Nausea | ~40% (first dose) | ~10% (chronic) |
| BP effect | Transient increase | Risk of hypotension (especially with alcohol/CNS depressants) |
| Onset | 45–60 minutes | 4–8 weeks of daily dosing |
Bremelanotide’s on-demand dosing is a significant practical advantage over flibanserin’s daily dosing requirement. Women who found flibanserin’s alcohol interaction and CNS side effects limiting may prefer bremelanotide. The injection route is a practical barrier for some patients.
Evidence Summary
| Endpoint | Population | Finding | Evidence quality |
|---|---|---|---|
| FSFI-D desire score (coprimary) [2] | Premenopausal HSDD women (N=1,202) | ✅ Significant improvement, p<0.001; effect size modest | Strong (Phase 3 RCT) |
| FSDS-DAO distress (coprimary) [2] | Same | ✅ Significant reduction, p<0.001 | Strong (Phase 3 RCT) |
| Satisfying sexual events/month (pre-specified secondary) | Same | ❌ Not significant (p=0.630) | Negative (pre-specified) |
| Proportion of satisfying encounters (post hoc) | Same | 25.0% vs. 9.8%, p<0.001 | Moderate (post hoc) |
| Long-term safety (52-week OLE) [3] | RECONNECT completers | Maintained efficacy; tolerability consistent | Moderate (open-label extension) |
| Erections in sildenafil-resistant men | N=180 men | 62% improvement vs. 21% placebo | Moderate (Phase 2) |
| Postmenopausal HSDD | No Phase 3 data | Not established | ❌ No data |
Common Misconceptions
“PT-141 is basically the same as Viagra — just more focused on desire.”
The mechanisms are completely different. Sildenafil inhibits PDE5 in peripheral vasculature, facilitating erections by preventing breakdown of cGMP in already-stimulated genital tissue. Bremelanotide activates MC4R in the hypothalamus, stimulating central desire and arousal circuits that precede and initiate genital response. One works peripherally on blood flow; the other works centrally on motivation and desire.
“PT-141 is a research peptide with no human evidence.”
PT-141 (bremelanotide) completed two Phase 3 RCTs with over 1,200 participants, has an approved NDA, a 52-week open-label extension, and is commercially sold as Vyleesi. It is one of the most clinically validated peptides in this entire series. The “research peptide” framing applies only to its off-label use in men and off-label populations.
“The trials proved it works perfectly.”
The trials proved statistical significance on two coprimary outcomes. The number of satisfying sexual events per month — arguably the most clinically meaningful outcome — did not significantly improve in the pre-specified analysis. Mean FSFI-D change of 0.35 falls below the pre-established MCID of 0.6. Bremelanotide helps many women with HSDD, but the magnitude of effect is real and limited, not transformative.
⚠️ “The blood pressure effect is minor and can be ignored.”
The blood pressure effect is real, it is contraindicated in patients with uncontrolled hypertension or CVD, and it warrants consideration in any patient with borderline cardiovascular risk. This is not a theoretical warning.
Frequently Asked Questions
Who is a good candidate for bremelanotide?
Premenopausal women with acquired, generalised HSDD — meaning loss of sexual desire that was previously present, occurring across all contexts, causing personal distress, and not explained by another medical condition, relationship problem, or medication side effect. It should not be the first intervention; addressing underlying causes, relationship factors, and psychological contributors is essential context.
Can postmenopausal women use it?
The FDA approval is specifically for premenopausal women. The prescribing information states it is not indicated for postmenopausal women. The hormonal environment of menopause affects sexual function through mechanisms that bremelanotide does not address.
Is the nausea manageable?
For most users, yes. Nausea peaks with the first dose and diminishes with subsequent use. Taking bremelanotide with food before sexual activity may help. Pre-medicating with ondansetron (if prescribed) is an option clinicians use. Approximately 10% of women discontinued in the RECONNECT trials due to nausea.
Does it cause skin darkening?
It can, with repeated use, because MC1R activation stimulates melanocytes. Darkening of existing moles, face, and breasts has been reported. This is not a cancer risk but should be monitored — regular skin self-examination and clinician review are recommended.[1]
Key Takeaways
- ✅ Bremelanotide is the only FDA-approved, on-demand, centrally-acting treatment for HSDD in premenopausal women. It represents a genuine pharmacological advance — the first approved drug that targets desire itself at the neural level rather than peripheral vascular function.
- ✅ The Phase 3 evidence is real and robust on two coprimary endpoints — sexual desire improvement and reduction in desire-related distress. The number of satisfying sexual events per month did not reach significance in the pre-specified analysis, which is an honest limitation of the evidence.[2]
- ⚠️ Effect sizes are modest. The mean FSFI-D change of 0.35 falls below the pre-established MCID of 0.6. Bremelanotide helps a meaningful proportion of treated women, but the average improvement is limited and the compound is not universally effective.
- ⚠️ The blood pressure contraindication is clinically real. Any prescriber must assess cardiovascular risk before initiating treatment. This is not a theoretical warning.[1]
- Off-label use in men is supported by preliminary Phase 2 data suggesting particular promise in PDE5 inhibitor non-responders. No Phase 3 male trial is yet completed.
- ⚠️ The nausea burden is substantial (40% on first dose) and is the primary reason for discontinuation in clinical practice. Management strategies exist but should be discussed before treatment initiation.[3]
References
Regulatory
- FDA NDA 210557 Approval Letter, June 21, 2019. Vyleesi (bremelanotide injection) prescribing information. Cranbury, NJ: Palatin Technologies, Inc. accessdata.fda.gov
Phase 3 Pivotal Trials
- Kingsberg SA, Clayton AH, Portman D, et al. Bremelanotide for the treatment of hypoactive sexual desire disorder: Two randomized phase 3 trials. Obstetrics & Gynecology. 2019;134(5):899–908. PMC6819021
- Simon JA, Kingsberg SA, Portman D, et al. Long-term safety and efficacy of bremelanotide for hypoactive sexual desire disorder. Obstetrics & Gynecology. 2019;134(5):909–917. PMC6819023
Early Clinical Development
- Molinoff PB, Shadiack AM, Earle D, Diamond LE, Quon CY. PT-141: A melanocortin agonist for the treatment of sexual dysfunction. Annals of the New York Academy of Sciences. 2003;994:96–102.
- Rosen RC, Diamond LE, Earle DC, Shadiack AM, Molinoff PB. Evaluation of the safety, pharmacokinetics and pharmacodynamic effects of subcutaneously administered PT-141, a melanocortin receptor agonist, in healthy male subjects and in patients with an inadequate response to Viagra. International Journal of Impotence Research. 2004;16(2):135–142.
Safety Review
- Clayton AH, Kingsberg SA, Portman D, et al. Safety profile of bremelanotide across the clinical development program. Journal of Women’s Health. 2022. doi: 10.1089/jwh.2021.0191
Preclinical Mechanistic
- Pfaus J, Giuliano F, Gelez H. Bremelanotide: An overview of preclinical CNS effects on female sexual function. Journal of Sexual Medicine. 2007;4(Suppl 4):269–279.
Key Investigators and Companies
- Palatin Technologies, Inc. — Cranbury, NJ; developed, patented, and commercialised bremelanotide; holds NDA 210557 and manufactures Vyleesi.
- Sheryl A. Kingsberg, PhD — Case Western Reserve/University Hospitals Cleveland; principal investigator of the RECONNECT Phase 3 programme; leading clinical researcher in female sexual dysfunction.
- James A. Simon, MD — George Washington University / IntimMedicine Specialists, Washington DC; co-PI on RECONNECT long-term extension; key female sexual medicine clinician and researcher.
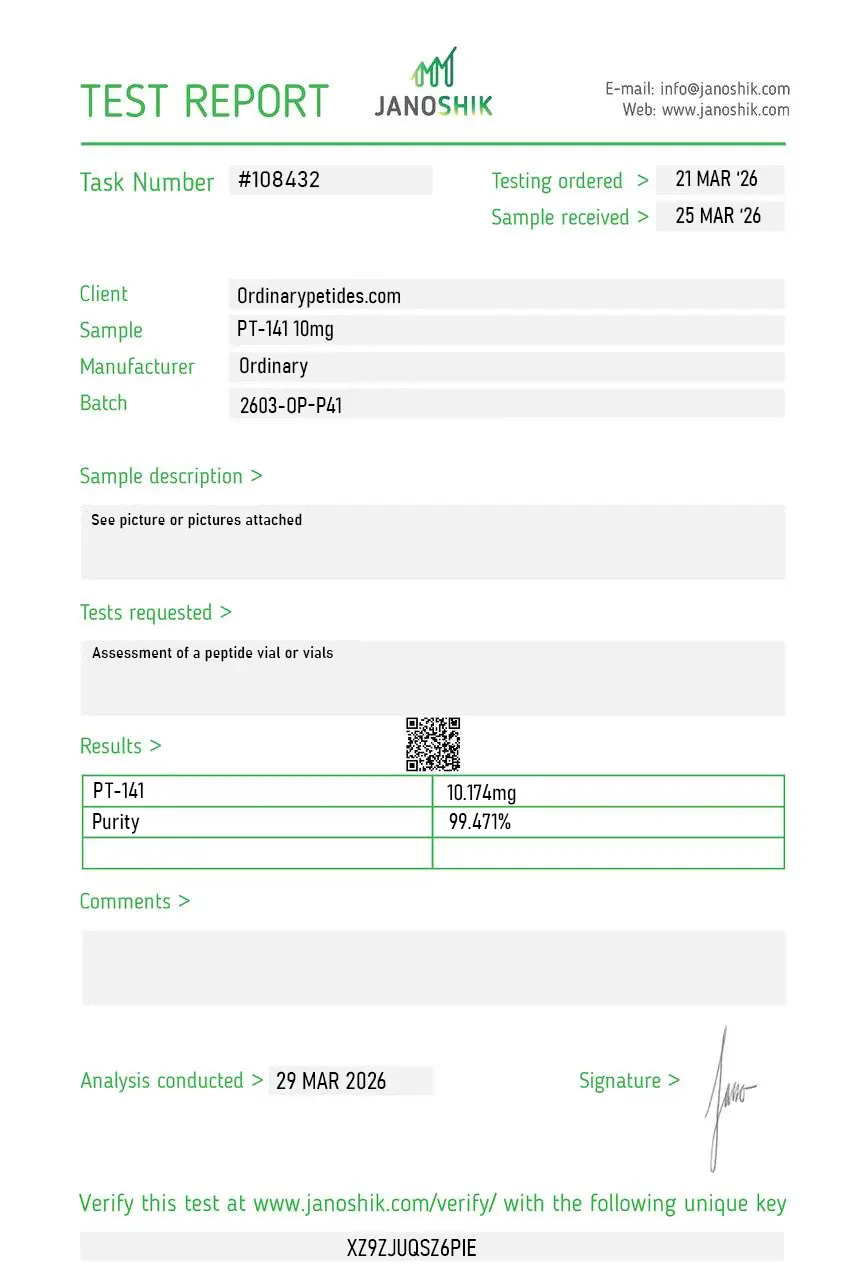
Certificate of Analysis
An independent test report is available for PT-141 10mg. This report provides batch-level documentation and analytical verification information for research reference.
We use bremelanotide in the wider melanocortin receptor pharmacology field — MC4R characterization in neuronal cell models, not the obvious indication-related work, because MC4R is expressed broadly in CNS neurons and the receptor's role in energy balance, autonomic regulation, and stress signaling is its own substantial research area. PT-141 as the MC4R-selective tool lets us probe those non-obvious receptor functions without confounding from the other melanocortin subtypes. The material activated MC4R cleanly across our neuronal-culture conditions.
Useful that the listing distinguishes bremelanotide from MT-II by selectivity rather than treating them as interchangeable cyclic melanocortin compounds, but it could note Palatin Technologies' specific development pathway — the original ED indication that didn't advance, the redirection to a different therapeutic area, the eventual Vyleesi approval in 2019. That clinical-history context is useful for researchers needing to justify procurement of an approved-drug research-grade compound. Material itself was reliable for our MC4R assays.
Yes. PT-141 is the historical/research name, while bremelanotide is the international nonproprietary name of the active substance.
In its official form, this is an FDA-approved drug Vyleesi for a narrow indication, not just a research peptide.
At present, there is no official approval for men. There were early ED studies, but that is not the same as an approved indication.
No. It is approved for acquired generalized HSDD in premenopausal women after excluding other causes of reduced desire.
According to the published data, the effect is statistically significant, but on average moderate, not dramatic.
Above all nausea, then the injection format, vascular limitations, and the risk of hyperpigmentation.
PT-141 acts through the central melanocortin system and is linked with sexual desire/the neurobiology of motivation, while sildenafil acts through a peripheral vascular mechanism.
PT-141 is the research name for bremelanotide — a synthetic cyclic heptapeptide and the FDA-approved therapeutic form of the melanocortin receptor agonist class derived from Melanotan 2. It was developed by Palatin Technologies after they identified it as a likely metabolite of MT-2 that retained the sexual function-enhancing properties of its parent compound while offering improved pharmacological characteristics. Structurally it is identical to MT-2 except that it has a free carboxyl group at the C-terminus where MT-2 has an amide — a modification that meaningfully changes its metabolic profile. It received FDA approval in June 2019 under the brand name Vyleesi for the treatment of hypoactive sexual desire disorder (HSDD) in premenopausal women — making it the first non-hormonal, centrally acting pharmacological treatment for this condition and one of the few peptide drugs approved specifically for sexual health.
PT-141 / bremelanotide is a non-selective melanocortin receptor agonist binding MC1R, MC3R, MC4R, and MC5R — the same receptor profile as MT-2. Its therapeutic effects on sexual function are mediated primarily through MC4R activation in the central nervous system, particularly in the hypothalamus and limbic system. Unlike phosphodiesterase-5 inhibitors such as sildenafil and tadalafil — which work by increasing blood flow to genital tissue through a peripheral vascular mechanism — PT-141 works centrally by activating neural circuits governing sexual desire, arousal, and motivation. This distinction is clinically meaningful — it addresses the psychological and neurological dimensions of sexual desire rather than purely the vascular mechanics of arousal, which is why it can be effective in women with HSDD even when genital blood flow is not the primary limiting factor.
Vyleesi (bremelanotide) is FDA-approved for the treatment of acquired, generalized hypoactive sexual desire disorder in premenopausal women. HSDD is characterized by low sexual desire that causes marked personal distress or interpersonal difficulty and is not attributable to a medical condition, medication, or another mental health disorder. The approval was based on two Phase 3 randomized controlled trials. In these trials, women using PT-141 reported significantly more satisfying sexual events and significantly reduced personal distress related to sexual desire compared to placebo. The magnitude of effect was modest but statistically significant and clinically meaningful to the treated population — an average increase of approximately 0.5 satisfying sexual events per month and reduction in distress scores. It was the second approved pharmacological treatment for HSDD after flibanserin (Addyi) — a daily oral serotonin agonist — but represents a mechanistically distinct on-demand option used approximately 45 minutes before anticipated sexual activity.
The MT-2 to PT-141 development story is one of rational drug design improving on a flawed parent compound. MT-2 has no approved therapeutic indication and is associated with significant safety concerns including mole changes, melanoma association, uncontrolled spontaneous erections, and substantial nausea — all of which limited its clinical development. PT-141 was developed specifically to address these limitations. The C-terminus modification results in faster metabolic clearance and a somewhat improved side effect profile versus MT-2. It is administered subcutaneously at a dose of 1.75 mg — lower than the doses typically used with unregulated MT-2 — and is available as a single-use autoinjector. It does not cause the prolonged erections or the degree of mole darkening seen with MT-2 at comparable clinical doses, though both effects can still occur. It is the only melanocortin agonist with FDA approval for a sexual health indication.
Vyleesi is administered as a single-use prefilled autoinjector delivering 1.75 mg subcutaneously into the abdomen or thigh approximately 45 minutes before anticipated sexual activity. No more than one dose in 24 hours is recommended and no more than one dose per day is approved. It should not be used more than approximately eight times per month. It is available by prescription only from a licensed physician.
Nausea is the most common and limiting side effect — occurring in approximately 40% of women in clinical trials, with 13% rating it as severe. It typically begins within one hour of administration and resolves within 12 hours. Flushing, injection site reactions, and transient facial and body flushing are very common. Headache is reported in a meaningful proportion of users. Transient blood pressure increases — both systolic and diastolic — occur in some patients, peaking approximately 12 minutes post-dose and resolving by 12 hours. For this reason PT-141 is contraindicated with high-risk cardiovascular disease and should not be used with nitrates given the blood pressure interaction risk. Hyperpigmentation — darkening of the face, gums, and breasts — can develop with more than eight doses per month due to MC1R activation, consistent with its melanocortin mechanism. Spontaneous erections in male users are an expected pharmacological effect.
Beyond the approved HSDD indication in premenopausal women, PT-141 is used off-label in men for erectile dysfunction and low libido — early clinical research did show significant erection induction in men with both psychogenic and organic erectile dysfunction, and this is the application that first captured attention during the MT-2 research era. Off-label use in postmenopausal women and men is practiced in wellness and men's health clinics. Compounded PT-141 products are available through some compounding pharmacies for these off-label applications, though the same product quality and dosing consistency concerns apply as with any compounded peptide. PT-141 is also banned by WADA for use in competitive sport.
Women who are pregnant or planning to become pregnant should not use it — there is insufficient safety data and animal studies suggest reproductive risks. People with known cardiovascular disease or uncontrolled hypertension should not use it given the blood pressure elevation effect. Anyone taking nitrates, nitric oxide donors, or other medications that lower blood pressure significantly should not use it given the compounding hypotensive risk. People with a history of hyperpigmentation disorders should be cautious given the melanocortin-driven pigmentation effects. Postmenopausal women should discuss with their physician as the approved indication is specifically for premenopausal women. Breastfeeding women should not use it.





