





Kisspeptin-10
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Kisspeptin-10: A Short Peptide With Major Research Interest in Reproductive Neuroendocrinology
Kisspeptin-10 is a short active fragment of the KISS1/KISS1R system that, in the research context, is used as a molecule for studying how the brain initiates the reproductive hormonal axis. In published observations in men, it rapidly enhanced GnRH-dependent release of LH and FSH, and in certain infusion regimens this was accompanied by an increase in testosterone; in women, the response depended noticeably on the phase of the cycle.
In experimental and preclinical data, this makes Kisspeptin-10 especially interesting as a precise upstream signal rather than as a "ready-made hormone in a syringe." At the same time, the molecule acts for a very short time, the clinical base for it is still early, and the far-reaching promises from marketing are clearly running ahead of the data.
That is why Kisspeptin-10 attracts attention not because of noise, but because it allows a look into the very logic of reproductive neuroendocrinology. If you are interested in peptides with strong research biology and a clear mechanism, this is exactly the kind of case that makes you want to take a closer look.
Kisspeptin-10: A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Kisspeptin is one of the most biologically important peptides discovered in the past thirty years. It is the master upstream regulator of human reproductive function — the “switch” that the brain uses to activate puberty and maintain adult fertility. Without functional kisspeptin signalling, humans fail to develop sexually and remain infertile regardless of otherwise intact gonads and pituitary glands. With activating mutations, puberty begins years too early.
Three threads of evidence distinguish kisspeptin from most peptides in this series. The genetic proof is airtight: loss-of-function mutations in KISS1 or KISS1R in humans produce a completely predictable and specific phenotype — absent puberty and infertility — while gain-of-function mutations produce precocious puberty.[1][2] The human clinical evidence is real and controlled: multiple randomised trials at Imperial College London have demonstrated that kisspeptin-54 can trigger oocyte maturation in IVF cycles with live birth rates of 45–62% per transfer and no cases of severe OHSS in high-risk patients.[7] The community use is pharmacologically confused: most commercial use is of KP-10, not KP-54, but KP-10’s 4-minute half-life severely limits its therapeutic utility, and all the clinical IVF and FHA evidence comes from KP-54.
| At a glance | |
|---|---|
| Gene | KISS1 (also historical name: KiSS-1, metastin gene) |
| KP-10 sequence | Tyr-Asn-Trp-Asn-Ser-Phe-Gly-Leu-Arg-Phe-NH&sub2; |
| MW (KP-10) | ~1,302 Da |
| Half-life (KP-10) | ~4 minutes in humans |
| Half-life (KP-54) | ~28 minutes in humans |
| Primary receptor | KISS1R (formerly GPR54) |
| Discovery | 2001 (KISS1 gene/receptor orphan ligand); 2003 (reproductive role via KISS1R mutations) |
| Key clinical group | Imperial College London / Hammersmith Hospital (Dhillo, Jayasena, Abbara) |
| Clinical form studied | ⚠️ Kisspeptin-54 (not KP-10) in most controlled trials |
| FDA status | ❌ Not approved; not on 503A compounding list |
| WADA | ❌ Prohibited at all times (S2) |
Discovery: Three Labs, One Molecule
The KISS1 gene was first identified in the late 1990s as a metastasis suppressor gene in melanoma cells. The gene product was named “metastin” by Ohtaki and colleagues at Takeda (2001), who characterised the KISS1-encoded peptide as a ligand for the orphan receptor GPR54.[3] The reproductive role was unknown until 2003, when two simultaneously published papers changed the field entirely:
De Roux et al. and Seminara et al. independently identified loss-of-function mutations in the GPR54 receptor gene (KISS1R) in patients from consanguineous families with hypogonadotropic hypogonadism — absent puberty, low LH/FSH, prepubertal sex hormone levels, and infertility, despite structurally intact pituitaries and gonads.[1][2] GPR54 knockout mice phenocopied the human syndrome. Despite the identification of KISS1 products in 2001, the reproductive aspect remained undiscovered until these simultaneous 2003 publications revealed the correlation of the kisspeptin system with the HPG axis and its crucial function in puberty onset and fertility. Activating mutations in KISS1R subsequently confirmed the reverse: central precocious puberty — completing the proof that kisspeptin signalling is both necessary and sufficient for driving reproductive axis activation.
The Kisspeptin Family: Peptides and Their Sizes
The KISS1 gene encodes a 145-amino acid prepropeptide processed into four bioactive C-terminal fragments, all sharing the same C-terminal decapeptide (KP-10) as their core active sequence:
| Form | Amino acids | Half-life | Notes |
|---|---|---|---|
| Kisspeptin-54 (KP-54) | 54 | ~28 min | Predominant circulating form; most clinical trial data; original name “metastin” |
| Kisspeptin-14 (KP-14) | 14 | Short | Intermediate form |
| Kisspeptin-13 (KP-13) | 13 | Short | Intermediate form |
| Kisspeptin-10 (KP-10) | 10 | ~4 min | Minimal active sequence; full KISS1R binding; research tool; half-life limits clinical utility |
All four forms bind KISS1R with equivalent affinity and produce the same intracellular signalling cascade. KP-54’s 7-fold longer half-life compared to KP-10 makes it substantially more suitable for sustained clinical applications. The clinical utility of all kisspeptins is limited by their short duration of action and the need for parenteral administration.[10]
Mechanism: The Master Regulator of GnRH Pulsatility
The central circuit
Kisspeptin’s mechanism places it upstream of every other component of the reproductive hormonal axis, including GnRH. Kisspeptin neurons in the hypothalamic arcuate nucleus (ARC) and anteroventral periventricular nucleus (AVPV) secrete kisspeptin → KISS1R activation on GnRH neurons → Gq/11 coupling → phospholipase C → IP&sub3; + DAG → intracellular Ca²+ rise → GnRH neuron depolarisation → GnRH pulse secretion → pituitary gonadotrophs → LH + FSH secretion → gonadal function. In vitro experiments confirm that kisspeptin-10 fails to stimulate LH or FSH release from isolated pituitary tissue — all observed gonadotropin responses depend on an intact hypothalamus. This means kisspeptin’s effect is strictly hypothalamus-dependent and allows differentiation of hypothalamic from pituitary causes of hypogonadism.[4]
The KNDy neuron: the pulse generator
The ARC kisspeptin neurons co-express neurokinin B (NKB) and dynorphin — collectively termed KNDy neurons. Neurokinin B activates NK3R on other KNDy neurons → positive autocrine/paracrine feedback → synchronised kisspeptin burst release → GnRH pulse. Dynorphin inhibits NK3R signalling → terminates the KNDy burst → allows pulse reset. This NKB-kisspeptin-dynorphin autoregulatory circuit in the ARC is currently understood as the primary GnRH pulse generator.[10]
Sexual dimorphism and menstrual cycle phase effects
⚠️ A pharmacologically critical finding: in healthy women during the follicular phase of the menstrual cycle, no alterations in serum gonadotropins were observed after IV bolus, subcutaneous bolus, or IV infusion of kisspeptin-10 at maximal doses. In women during the preovulatory phase, serum LH and FSH were elevated after IV bolus kisspeptin-10 (10 nmol/kg).[5] Kisspeptin-10 does not work at all in women during the follicular phase — the phase that comprises the majority of the menstrual cycle. Any community use of KP-10 by women without accounting for menstrual cycle phase is pharmacologically likely to produce no response during the majority of the cycle.
Human Clinical Evidence
LH pulse frequency in men (George et al. 2011)
IV bolus KP-10 doses 0.01–3.0 µg/kg in healthy men produced a rapid and dose-dependent rise in serum LH concentration, with maximal stimulation at 1 µg/kg (from 4.1 ± 0.4 to 12.4 ± 1.7 IU/L at 30 minutes). Administration of 3 µg/kg elicited a reduced response vs. 1 µg/kg — an inverted dose-response suggesting receptor desensitisation at supratherapeutic doses. Infusion of KP-10 at 4 µg/kg/h for 22.5 hours increased LH from 5.4 to 20.8 IU/L and serum testosterone from 16.6 to 24.0 nmol/L.[4]
IVF oocyte maturation trigger: the best clinical evidence
The most rigorously controlled clinical data for any kisspeptin involves kisspeptin-54 as an oocyte maturation trigger in IVF. Following a standard recombinant FSH/GnRH antagonist protocol, oocyte maturation occurred in 95% of women. At all doses of kisspeptin-54, biochemical pregnancy, clinical pregnancy, and live birth rates per transfer were 63%, 53%, and 45%, respectively. Highest pregnancy rates were observed following 9.6 nmol/kg kisspeptin-54 (85%, 77%, and 62%). No woman developed moderate, severe, or critical OHSS.[7]
Hypothalamic amenorrhea (FHA)
Twice-weekly subcutaneous KP-54 for 8 weeks produced an increase in gonadotropins from the first dose, with a comparable increase by day 14, and the response remained consistent after 8 weeks. Kisspeptin-54 administration twice weekly resulted in a lower degree of desensitisation compared to twice-daily administration. However, the protocol did not restore menstruation in women with hypothalamic amenorrhoea.[8] This is important: FHA reflects a complex metabolic and stress-driven suppression of kisspeptin neurons, not simply kisspeptin deficiency. Exogenous kisspeptin partially overcomes this suppression, but the underlying energy deficit driving KNDy neuron silencing is not reversed by kisspeptin administration alone.
Clinical evidence summary
| Indication | Population | Form studied | Key finding |
|---|---|---|---|
| LH stimulation in men [4] | Healthy men | KP-10 (IV) | Dose-dependent LH/testosterone rise; inverted response at 3 µg/kg |
| LH stimulation in women [5] | Healthy women | KP-10 (IV/SC) | ⚠️ No response in follicular phase; response in preovulatory phase only |
| IVF oocyte trigger [7] | High-OHSS-risk women | KP-54 (SC) | 95% oocyte maturation; 45% live birth; zero severe OHSS |
| Hypothalamic amenorrhea [8] | Women with FHA | KP-54 (SC, twice weekly) | Increased LH pulsatility; did not restore menstruation |
| Sexual function | Men and women | KP-54 | Modulates sexual brain activity and physiological arousal |
Kisspeptin-10 vs. Kisspeptin-54: The Clinical Relevance Gap
| Feature | KP-10 | KP-54 |
|---|---|---|
| Amino acids | 10 | 54 |
| Half-life (IV) | ~4 min | ~28 min |
| KISS1R binding | Full agonist | Full agonist |
| Clinical trials completed | Pharmacodynamic studies only; no therapeutic RCTs | ✅ Multiple Phase 2 RCTs (IVF, FHA, IHH) |
| SC bioavailability established? | Not formally characterised | More studied |
| Community use | Predominant form sold commercially | Less common commercially |
MVT-602: The Next-Generation Analogue
MVT-602, a KISS1R agonist analogue developed by Myovant Sciences, has been studied in Phase 1/2 trials. MVT-602 induced an LH surge of similar amplitude to that of native KP-54, however the duration of the LH rise was markedly prolonged (time of peak LH: MVT-602 21–22 hours vs. KP-54 4.7 hours), resulting in a more than four-fold increase in the area under the LH exposure curve.[11] MVT-602’s prolonged LH elevation more closely resembles the physiological mid-cycle LH surge, potentially offering superior IVF trigger performance. This represents the next wave of kisspeptin pharmacology — analogue engineering for improved clinical performance.
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) | ❌ Not approved for any indication |
| FDA — 503A compounding | ❌ Not on the bulks list |
| FDA — 503B compounding | ❌ Not on the list |
| EMA (Europe) | ❌ Not approved |
| WADA | ❌ Prohibited at all times — S2 (Peptide Hormones, Growth Factors) |
| Research use | Active Phase 2 clinical research at multiple centres globally |
Desensitisation: The Continuous vs. Pulsatile Problem
In a pattern analogous to continuous GnRH administration, continuous kisspeptin administration leads to KISS1R downregulation. The George et al. study noted that LH pulses were obscured at high continuous infusion rates. The FHA study found reduced desensitisation with twice-weekly vs. twice-daily KP-54 administration. Pulsatile or intermittent kisspeptin delivery maintains HPG axis responsiveness; continuous high-dose delivery risks receptor downregulation or, at extreme doses, suppression of the reproductive axis — the same fundamental pharmacological constraint that applies to GnRH agonist therapy.[4]
Common Misconceptions
“Kisspeptin-10 is what the clinical trials used.”
⚠️ Most completed controlled clinical trials used kisspeptin-54. KP-10 has been studied in pharmacodynamic human studies but not in therapeutic trials for IVF triggering, FHA restoration, or IHH treatment. The evidence base for clinical efficacy belongs almost entirely to KP-54.
“Kisspeptin is natural and upstream, so it’s safer than other hormones.”
Upstream positioning in the HPG axis does not confer safety. Kisspeptin can desensitise its receptor with continuous exposure, could drive supraphysiological LH surges in responsive individuals, and the effects of chronic exogenous KP-10 administration on the GnRH pulse generator in healthy adults are not characterised.
“KP-10 and KP-54 are basically the same, just different sizes.”
They share the same receptor and identical intracellular signalling, but a 7-fold difference in half-life translates to a completely different exposure-response relationship in vivo. This is particularly important for sustained kisspeptin receptor engagement needed for pulsatile GnRH release.
Frequently Asked Questions
Is kisspeptin a treatment for low testosterone?
Kisspeptin stimulates endogenous testosterone by activating the HPG axis upstream. It will only work if the deficiency is hypothalamic (GnRH neuron dysfunction, as in CHH/Kallmann or FHA) and the pituitary and gonads are functional. It does not work in primary hypogonadism (testicular failure) or pituitary gonadotroph failure.[10]
Can kisspeptin help with functional hypothalamic amenorrhea?
Clinical studies show KP-54 can partially restore LH pulsatility in FHA, but menstrual restoration in the studied protocols was not demonstrated.[8] The primary treatment for FHA remains addressing the underlying energy deficit. Kisspeptin may have a future adjunctive role, but this remains unvalidated.
How does kisspeptin compare to gonadorelin for HPG axis stimulation?
Gonadorelin acts directly at the pituitary GnRH receptor; kisspeptin acts upstream at hypothalamic GnRH neurons. Both ultimately produce pulsatile GnRH release. Gonadorelin requires a pump for true pulsatile delivery in most clinical contexts. The IVF evidence base strongly favours kisspeptin-54 as an ovulation trigger; gonadorelin’s evidence base is stronger for CHH spermatogenesis induction. Neither is approved in the US.
Key Takeaways
- Kisspeptin is the master upstream regulator of the HPG axis — the only known peptide whose loss of function specifically abolishes puberty and reproductive function while leaving all other pituitary axes intact. Its obligate role is confirmed by genetic evidence.[1][2]
- Kisspeptin-10 is the minimal bioactive fragment with full KISS1R affinity and the complete signalling cascade. Its 4-minute half-life severely limits clinical utility compared to KP-54 (28 minutes), and most therapeutic clinical trials used KP-54.
- The clinical evidence for kisspeptin is genuinely good — in the right indications with the right form. The Imperial College IVF trigger data (95% oocyte maturation, 45–62% live birth rates, zero severe OHSS) represents some of the most clinically meaningful peptide data in this series. This evidence belongs to KP-54 in properly conducted IVF cycles.[7]
- ⚠️ The sexual dimorphism finding is a critical clinical caveat. KP-10 produces no gonadotropin response in women during the follicular phase — the phase comprising the majority of the menstrual cycle. Community use without phase-specific timing will have no pharmacological effect during this period.[5]
- ⚠️ The community market sells KP-10; the clinical literature studied KP-54. This mismatch between what is commercially available and what has been clinically validated is the central evidentiary problem for anyone attempting to translate the kisspeptin evidence base into community use.
- MVT-602 represents the next generation — a KISS1R agonist analogue with a prolonged LH surge profile that more closely resembles the natural mid-cycle surge and may eventually find a path to regulatory approval.[11]
References
Discovery and Genetics
- de Roux N, Genin E, Carel J-C, Matsuda F, Chaussain J-L, Milgrom E. Hypogonadotropic hypogonadism due to loss of function of the KiSS1-derived peptide receptor GPR54. Proceedings of the National Academy of Sciences. 2003;100:10972–10976.
- Seminara SB, Messager S, Chatzidaki EE, et al. The GPR54 gene as a regulator of puberty. New England Journal of Medicine. 2003;349:1614–1627.
- Ohtaki T, Shintani Y, Honda S, et al. Metastasis suppressor gene KiSS-1 encodes peptide ligand of a G-protein-coupled receptor. Nature. 2001;411(6837):613–617.
KP-10 Human Pharmacodynamics
- George JT, Veldhuis JD, Roseweir AK, Newton CL, et al. Kisspeptin-10 is a potent stimulator of LH and increases pulse frequency in men. Journal of Clinical Endocrinology and Metabolism. 2011;96(8):E1228–E1236. PMC3380939
- Jayasena CN, Nijher GMK, Comninos AN, Abbara A, et al. The effects of kisspeptin-10 on reproductive hormone release show sexual dimorphism in humans. Journal of Clinical Endocrinology and Metabolism. 2011;96(12):E1963–E1972. PMC3232613
IVF Trigger Trials
- Jayasena CN, Abbara A, Comninos AN, Nijher GMK, et al. Kisspeptin-54 triggers egg maturation in women undergoing in vitro fertilization. Journal of Clinical Investigation. 2014;124(8):3667–3677.
- Abbara A, Jayasena CN, Christopoulos G, Narayanaswamy S, et al. Efficacy of kisspeptin-54 to trigger oocyte maturation in women at high risk of OHSS during IVF therapy. Journal of Clinical Endocrinology and Metabolism. 2015;100(9):3322–3331. PMC4570165
FHA and Clinical Reviews
- Patel AH, Koysombat K, Pierret A, et al. Kisspeptin in functional hypothalamic amenorrhea: pathophysiology and therapeutic potential. Annals of the New York Academy of Sciences. 2024;1540(1):21–46.
- Sharma B, Koysombat K, Comninos AN, Dhillo WS, Abbara A. Use of kisspeptin to trigger oocyte maturation during in vitro fertilisation (IVF) treatment. Frontiers in Endocrinology. 2022;13:972137.
- Clarke H, Dhillo WS, Jayasena CN. Comprehensive review on kisspeptin and its role in reproductive disorders. Endocrinology and Metabolism. 2015;30:124.
- Abbara A, Clarke SA, Dhillo WS. Clinical potential of kisspeptin in reproductive health. Trends in Molecular Medicine. 2021;27:807–823.
Key Investigators
- Waljit S. Dhillo, PhD, FRCP — Imperial College London; principal investigator of the kisspeptin clinical research programme; first to study kisspeptin-54 in human volunteers (2005) and to conduct controlled IVF trigger trials.
- Channa N. Jayasena, PhD, MRCP — Imperial College London and Hammersmith Hospital; conducted the foundational kisspeptin-10 and -54 human pharmacodynamic and therapeutic studies.
- Ali Abbara, PhD, MRCP — Imperial College London; lead author on kisspeptin-54 OHSS-risk IVF trigger trial (2015) and subsequent kisspeptin clinical development work.
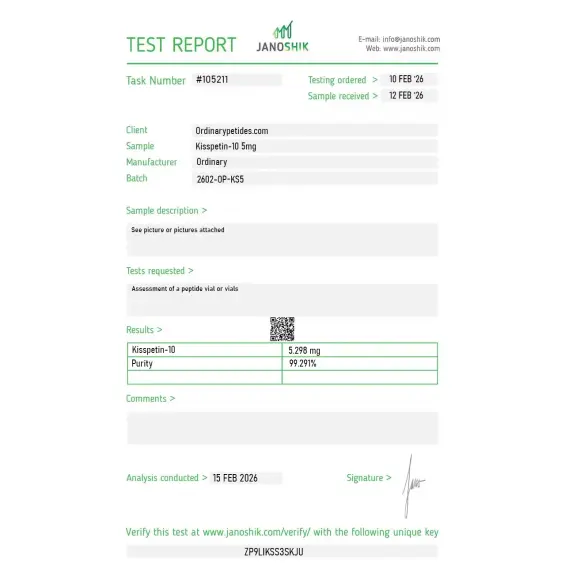
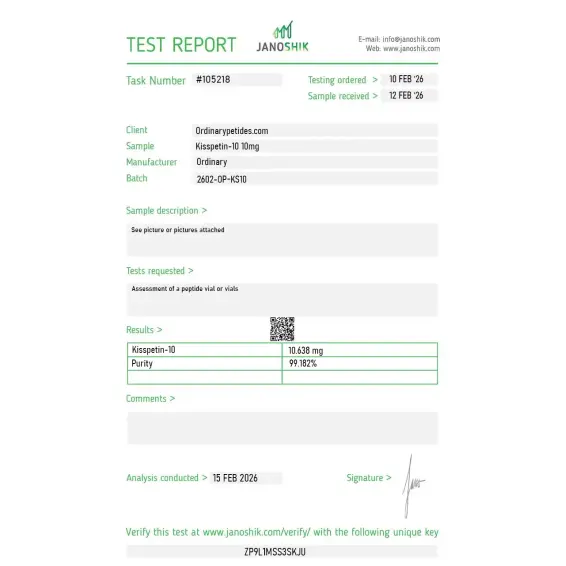
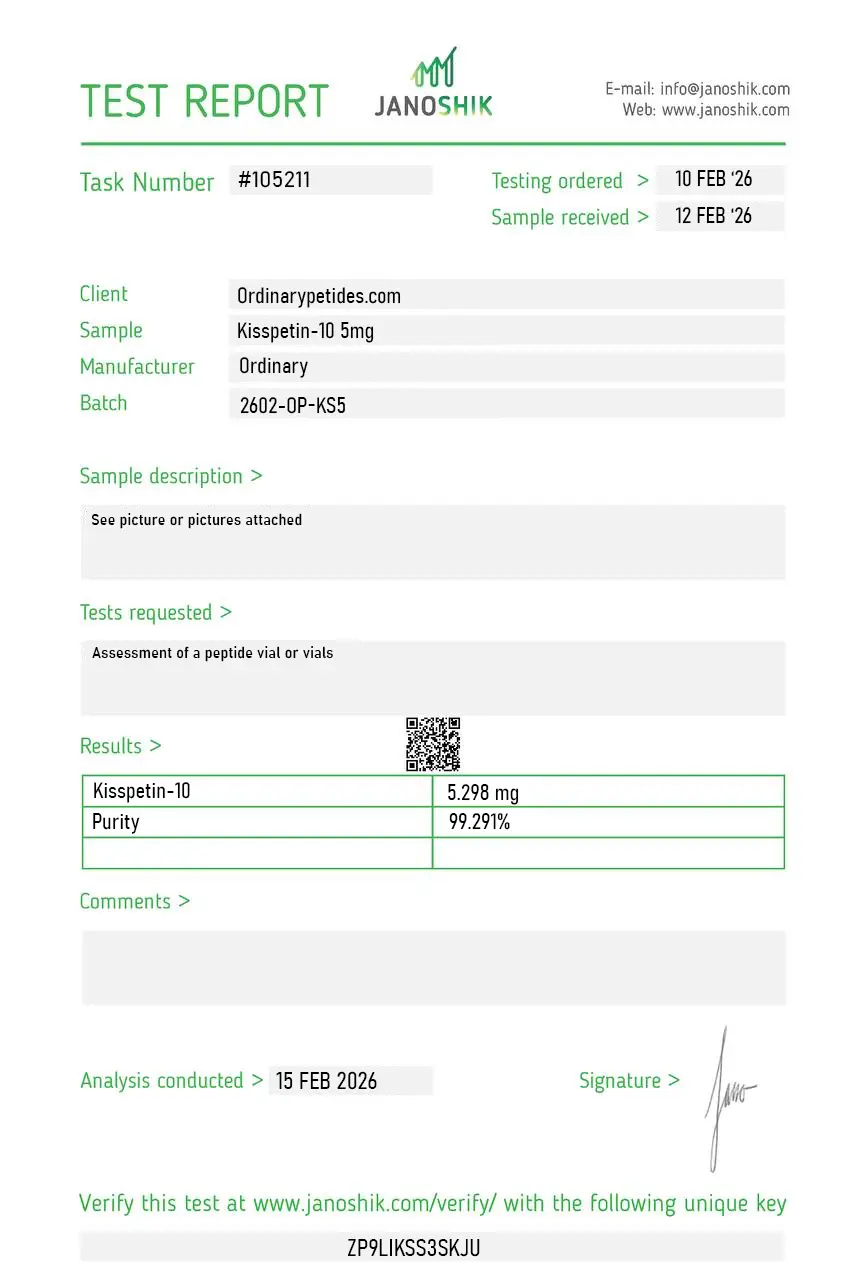
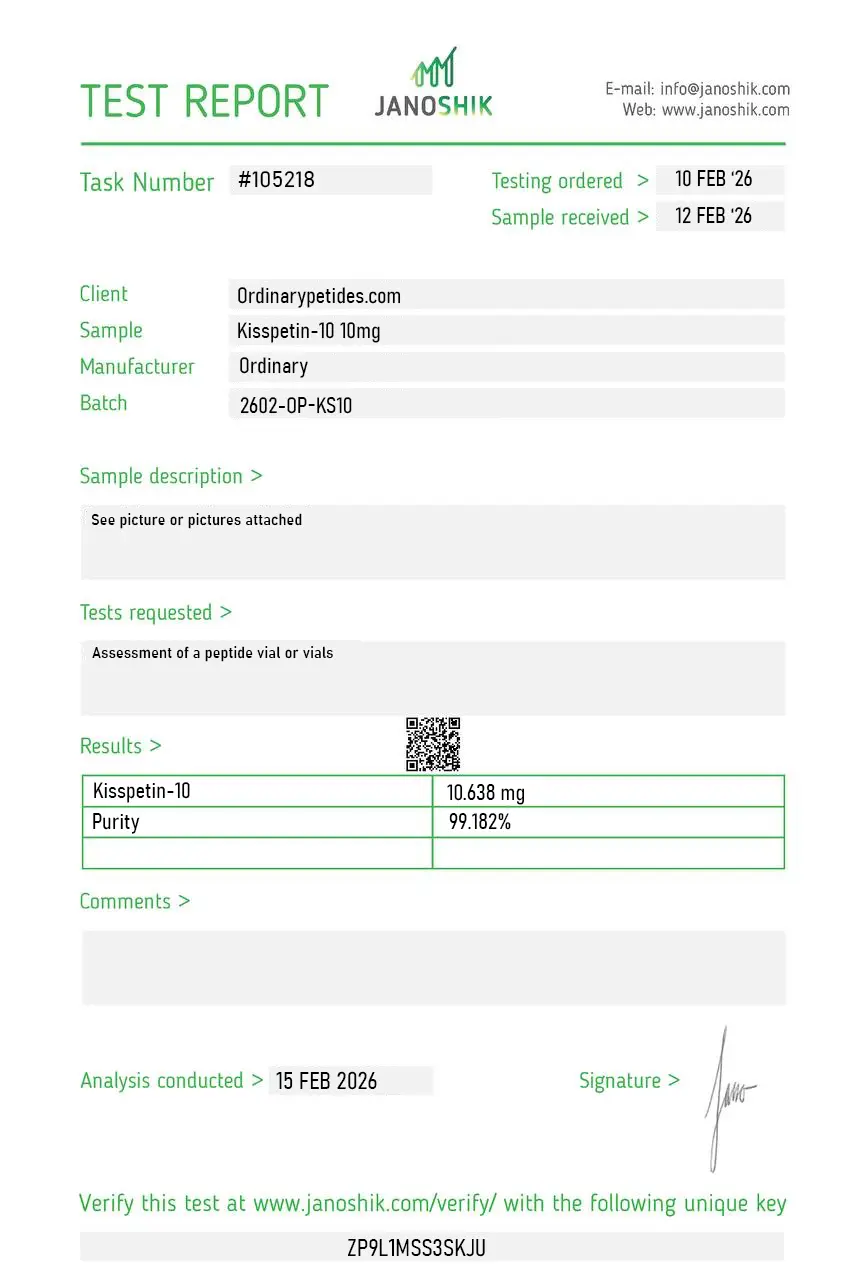
Certificate of Analysis
Independent test reports are available for Kisspeptin-10 5mg and 10mg batches. These reports provide batch-level documentation and analytical verification information for research reference.
Based on 1 reviews
5.0
The C-terminal Phe-amide is the receptor-engaging end and worth understanding when ordering — the active site of KP-10 is concentrated in the C-terminal RFamide motif (Arg-Phe-NH₂), which is conserved across the RFamide peptide family (NPFF, NPVF, prolactin-releasing peptide). For studying RFamide pharmacology comparatively, KP-10 is the GPR54-engaging member of that broader family rather than a standalone compound. The material gave the expected RFamide-class signaling profile in our assays.
Kisspeptin-10 (KP-10) is a naturally occurring decapeptide — ten amino acids — representing the minimal bioactive C-terminal sequence of the kisspeptin family of peptides encoded by the KISS1 gene. The kisspeptin family includes four isoforms named by their amino acid length — kisspeptin-10, -13, -14, and -54 — all of which share the same C-terminal arginine-amidated phenylalanine (RFamide) sequence that confers receptor activity. Kisspeptin-54 is the predominant circulating form in humans, but KP-10 retains equivalent potency at KISS1R in vitro and has a shorter half-life with more rapid onset of action — making it more practical for research and certain clinical applications. Originally discovered in 1996 as a tumor metastasis suppressor — initially named metastin — its critical role in reproductive neuroendocrinology was only established in 2003 when inactivating mutations of KISS1R (then called GPR54) were found to cause pubertal failure and hypogonadotropic hypogonadism.
Not in the usual sense. It is better described as a regulatory neuropeptide that acts upstream of GnRH, LH, and FSH in the control of reproduction.
In some human studies, yes. In men, Kisspeptin-10 has been shown to stimulate the reproductive axis and can increase testosterone under certain experimental conditions. But that does not mean it has proven long-term therapeutic benefit.
It is scientifically important because it allows a relatively physiological activation of the GnRH axis and helps researchers study puberty, fertility, hypogonadism, and LH pulse regulation.
One major limitation is that it is broken down very quickly and remains in circulation only for a short time, while long-term clinical data remain limited.
No. Based on the official materials referenced, Kisspeptin-10 is not FDA-approved. Regulatory discussions instead point to limited safety data for some forms of use.
For the human product, a commonly listed sequence is YNWNSFGLRF-NH2. Some non-human versions differ; for example, Cayman's mouse/rat Kisspeptin-10 is listed as YNWNSFGLRY-NH2. The correct sequence should always be taken from the supplier's product page or COA.
For human Kisspeptin-10, PubChem lists a molecular weight of 1302.4 g/mol. Species-specific variants may differ slightly; Cayman's mouse/rat product is listed at 1318.4 Da.
Kisspeptin-10 is commonly supplied as a solid or lyophilized peptide powder. Different vendors use slightly different wording, but product pages consistently describe it in dry peptide form rather than as a ready-to-use liquid.
Common storage guidance is to keep the peptide desiccated and frozen below about -18°C to -20°C, avoid repeated freeze-thaw cycles, and after reconstitution store it at 4°C for short-term use. Exact storage instructions can vary slightly by supplier, so the label or datasheet should control.
Commercial research listings commonly state that Kisspeptin-10 is for laboratory research use only and not for human or veterinary diagnostic or therapeutic use.
Yes, many suppliers provide or reference a Certificate of Analysis, often including batch-specific purity and identity data such as HPLC or related analytical results. Availability depends on the seller and batch.
Kisspeptin-10 binds to KISS1R — a G protein-coupled receptor — expressed predominantly on GnRH neurons in two key hypothalamic populations: the arcuate nucleus and the rostral periventricular region of the third ventricle. Activation of KISS1R on GnRH neurons triggers GnRH release into the hypothalamo-pituitary portal circulation, which then stimulates anterior pituitary gonadotrope cells to release both LH and FSH. LH drives gonadal testosterone production in men and ovulation in women. FSH drives spermatogenesis in men and follicular development in women. This places kisspeptin neurons at the very top of the reproductive endocrine hierarchy — upstream of GnRH, which is itself upstream of the entire HPG axis covered across multiple earlier entries in this series. Kisspeptin neurons also co-express neurokinin B and dynorphin in what is known as the KNDy network, which governs the pulsatile rhythm of GnRH secretion. This makes kisspeptin signaling not just a trigger but the master pacemaker of reproductive hormonal pulsatility.
Kisspeptin-10 has a meaningful published human evidence base. IV bolus administration in healthy men produced dose-dependent LH increases at doses as low as 0.3 nmol/kg, with a 2.5-fold increase in LH from baseline at standard doses — comparable to equimolar kisspeptin-54. LH pulse frequency increased significantly during IV infusion. In men with hypogonadotropic hypogonadism pulsatile kisspeptin administration restored LH pulsatility and testosterone production. A notable sexual dimorphism was documented — women in the follicular phase of the menstrual cycle showed markedly reduced LH response compared to men and women in the preovulatory phase, a finding with important clinical implications. In fertility medicine kisspeptin has been studied as an alternative to HCG for triggering final oocyte maturation in IVF, with promising results suggesting reduced ovarian hyperstimulation syndrome (OHSS) risk compared to standard HCG triggers. A published clinical trial in men with hypoactive sexual desire disorder showed 56% improvement in sexual response correlated with increased kisspeptin-driven activation of brain regions involved in sexual arousal including the posterior cingulate cortex.
Following the 2020 FDA ruling reclassifying HCG as a biological product — which significantly restricted compounded HCG availability — kisspeptin-10 has emerged as a clinically interesting upstream alternative for men on TRT who need to maintain testicular function, spermatogenesis, and fertility. Where HCG acts directly on Leydig cells mimicking LH, and gonadorelin stimulates pituitary LH and FSH release, kisspeptin-10 acts one step further upstream — stimulating hypothalamic GnRH neurons to generate their own pulsatile GnRH output. This is the most physiologically complete HPG axis maintenance strategy of the three. Its practical advantage over gonadorelin is that KISS1R desensitization with pulsatile dosing appears less pronounced than GnRH receptor desensitization, and its upstream position means it exercises and maintains the full neuroendocrine cascade rather than bypassing any part of it.
In published human research IV administration has been used most commonly due to KP-10's rapid enzymatic degradation in subcutaneous tissue — a plasma half-life of approximately 4 minutes makes subcutaneous bolus dosing pharmacokinetically challenging. Continuous IV or subcutaneous infusion using pump devices has been studied in reproductive medicine contexts. In TRT maintenance wellness protocols subcutaneous injection two to three times weekly is the most practical approach, acknowledging that the very short half-life means plasma exposure is brief and pulsatile by nature. Typical research and clinical protocol doses range from 1 mcg/kg body weight upward depending on indication.
Kisspeptin-10 has a generally favorable safety profile in published clinical trials. Mild headaches and abdominal discomfort are the most commonly reported effects. Flushing and injection site reactions have been noted. Tachyphylaxis — progressive loss of response with repeated dosing — is a documented concern particularly with twice-daily subcutaneous administration in women with hypothalamic amenorrhea, attributed to KISS1R desensitization. This limits continuous high-frequency dosing protocols and supports intermittent pulsatile approaches. Gonadotropin hypersecretion at excessive doses is a theoretical risk, particularly regarding precocious puberty implications in children. Long-term human safety data remains incomplete.
Children and adolescents should not use it given KISS1R's central role in pubertal timing — inappropriate activation could trigger precocious puberty. Pregnant women should not use it once pregnancy is established. People with hormone-sensitive cancers including breast and prostate cancer should not use it given its upstream role in driving testosterone and estrogen production. People with conditions made worse by elevated gonadotropins or sex hormones should exercise caution. It is banned by WADA under Peptide Hormones, Growth Factors, and Related Substances. It is not FDA-approved for any therapeutic indication, though it is under active clinical investigation for fertility and reproductive medicine applications.





