


HCG
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
HCG: A Real Hormone with a Precise Job, Not a "Cutting Injection"
HCG is not a "cutting injection" and not a universal testosterone booster, but a real human hormone with a very specific job: to imitate an LH-like signal where that signal is actually needed.
In the clinical context, its main strength showed up not in lifestyle promises, but in clearly defined scenarios — for example, as an ovulation trigger in reproductive protocols and as part of strategies aimed at preserving or restoring spermatogenesis in selected men.
That is exactly what makes HCG interesting: not because it "raises everything," but because it works in a targeted way and through a clear endocrine logic.
The molecule has a real medical biography, and that is precisely why it should not be reduced to a "hormonal life hack." In the research and clinical setting, HCG is valuable where an LH-like signal is truly needed — not where someone is looking for magic in an ampoule.
Practical Takeaway
If you are interested not in hype peptides but in serious molecules with real physiology behind them, HCG absolutely deserves attention.
Human Chorionic Gonadotropin (hCG): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
hCG is unusual in this article series: it is not a research peptide. It is a fully characterised endogenous glycoprotein hormone — the molecule that tells the corpus luteum to keep producing progesterone in early pregnancy, thereby maintaining the uterine environment necessary for a developing embryo. It has been clinically used in reproductive medicine for decades, is FDA-approved in the United States, and has a substantial evidence base across multiple indications.
Its clinical uses span two entirely different physiological systems: in women, it triggers ovulation and supports early luteal function in fertility treatment; in men, it acts as a long-acting LH surrogate, stimulating Leydig cells to produce intratesticular testosterone, which preserves spermatogenesis in the context of suppressed gonadotropins.
The compound carries three complicating factors that need honest treatment. The compounding restriction: following a 2020 FDA ruling, most compounding pharmacies can no longer legally produce hCG in the US, creating access gaps that drove practitioners toward alternatives including gonadorelin — a compound with far less evidence for TRT-adjunct use. The weight-loss fraud: hCG was promoted for years as a weight-loss agent; controlled studies have consistently shown zero efficacy for weight loss beyond the caloric restriction that accompanied hCG protocols, and the FDA has explicitly prohibited this use. The cancer marker identity: hCG is simultaneously a fertility hormone, a therapeutic agent, and a tumour marker — elevated serum hCG in a non-pregnant man requires evaluation for germ cell tumours.
| At a glance | |
|---|---|
| Full name | Human chorionic gonadotropin |
| Abbreviation | hCG |
| Structure | Heterodimeric glycoprotein; α-subunit (92 AA) + β-subunit (145 AA); MW ~36.7 kDa |
| Endogenous source | Placental syncytiotrophoblast; minor pituitary contribution |
| Receptor | LHCG receptor (shared with LH) |
| Half-life | 24–37 hours (dramatically longer than LH at 25–30 minutes) |
| Pharmaceutical sources | Urinary-derived (Pregnyl, Novarel) or recombinant (Ovidrel = choriogonadotropin alfa) |
| FDA-approved indications (men) | Hypogonadotropic hypogonadism; cryptorchidism; prepubertal induction |
| FDA-approved indications (women) | Anovulatory infertility; ART trigger; luteal support |
| Compounding status (US) | ⚠️ Restricted since 2020 for 503A; limited availability through 503B |
| Weight-loss use | ⚠️ Explicitly FDA-determined fraud; no evidence base |
| Tumour marker role | Elevated β-hCG in men: screening for testicular germ cell tumours |
| WADA | ❌ Prohibited in men at all times (S2); permitted in women in competition |
Biology: What hCG Actually Is and Does
Structure: the glycoprotein architecture
hCG belongs to the glycoprotein hormone family alongside LH, FSH, and TSH. All four share an identical α-subunit; each has a hormone-specific β-subunit that confers receptor selectivity. hCG is heterodimeric, with a molecular mass of 36.7 kDa, approximately 14.5 kDa α-hCG and 22.2 kDa β-hCG.[1]
The β-subunit of hCG shares the first 121 amino acids with β-LH (approximately 80% sequence homology) but has a unique 24-amino-acid C-terminal peptide extension (β-CTP) that is absent from LH. This CTP contains four O-linked oligosaccharide chains — and this is the molecular basis for hCG’s dramatically longer half-life. LH has a circulating half-life of just 25–30 minutes, while hCG has a circulating half-life of approximately 37 hours — 80-fold longer than LH — with approximately 80× the biological activity. Carbohydrate side chains comprise 25–40% of the molecular weight of hCG — among the highest carbohydrate content of any hormone.[3]
Endogenous functions
The textbook description — “hCG maintains the corpus luteum” — is accurate but significantly incomplete. Modern research has established multiple essential functions:
Corpus luteum maintenance and progesterone production: After implantation (~3 weeks gestation), the developing trophoblast begins producing hCG, which replaces pituitary LH in stimulating corpus luteal progesterone synthesis. Without this progesterone, the uterine lining would shed and pregnancy would fail. This continues until the placenta develops sufficient steroidogenic capacity (~6 weeks gestation).
Uterine vascular development: hCG promotes angiogenesis in the myometrial spiral arteries through the length of pregnancy, acting on LH/hCG receptors on the spiral arteries. This is probably a major function of hCG throughout gestation, ensuring adequate blood supply to the placenta.[2]
Syncytiotrophoblast formation, maternal immune tolerance, and myometrial suppression are additional well-documented roles in placentation and pregnancy maintenance.[2]
Why hCG is a tumour marker
Some cancerous tumours produce hCG; therefore, elevated levels measured when the patient is not pregnant may lead to a diagnosis of cancer. β-hCG is secreted by seminoma, choriocarcinoma, teratoma with elements of choriocarcinoma, other germ cell tumours, hydatidiform mole, and islet cell tumour. A positive result in a male can be a test for testicular cancer.[3] Specifically, serum hCG is elevated in approximately 20–40% of seminomas and 40–60% of non-seminomatous germ cell tumours (NSGCTs). hCG is used alongside AFP and LDH to stage, monitor treatment response, and detect recurrence in testicular cancer.
Pharmaceutical Preparations
| Brand | Type | Manufacturer | Primary use |
|---|---|---|---|
| Pregnyl | Urinary-derived | Merck | Hypogonadism, cryptorchidism, ovulation trigger |
| Novarel | Urinary-derived | Ferring | Ovulation induction, hypogonadism |
| Ovidrel (Choriogonadotropin alfa) | Recombinant | EMD Serono | ART trigger, ovulation induction |
Urinary-derived hCG is extracted from the urine of pregnant women and purified/standardised to International Units. Recombinant choriogonadotropin alfa (Ovidrel) is produced in Chinese hamster ovary cells; 250 µg provides approximately 6,500 IU of biological activity and is equivalent in clinical efficacy for ART triggering.[13]
FDA-Approved Indications and Evidence
In men: hypogonadotropic hypogonadism and fertility
For men with hypogonadotropic hypogonadism (secondary hypogonadism where the defect is in GnRH/LH/FSH signalling rather than testicular function), hCG stimulates Leydig cell testosterone production and, in combination with FSH, spermatogenesis. A 2024 systematic review and meta-analysis assessed 5,328 patients with congenital or acquired HH, mainly treated with hCG-based therapy. This therapy effectively increased testicular volume, penile size, and testosterone levels in over 98% of patients. Complete spermatogenesis was achieved in 86% of patients using combined therapy (hCG + FSH) compared with 40% with hCG monotherapy.[9] This is the strongest evidence base in this article series for any hormonal intervention.
In men: TRT adjunct for fertility preservation
Coolen et al. (2010) — the foundational study: This retrospective review examined patients on TRT given low-dose hCG (500 IU every other day). Mean sperm density was 34 M/mL prior to TRT and 26 M/mL during treatment (p=0.5). Mean sperm motility was 47% prior to therapy and 51% during therapy (p=0.8). No patient became azoospermic. Pregnancy was achieved in 9/12 patients attempting to conceive during treatment.[5] Additional dose-ranging studies established that even low doses (125 IU every other day) maintain intratesticular testosterone at 75–93% of baseline; 500 IU every other day is considered the minimum for most men requiring fertility preservation during TRT.
A 2025 retrospective analysis in a Netherlands harm reduction clinic found that hCG administered to men using non-prescribed androgens without cessation produced clinically meaningful spermatogenesis restoration in a proportion of patients — the first clinical data on hCG efficacy in the real-world context of continued androgen use.[8]
In men: monotherapy for subclinical hypogonadism
A multi-institutional retrospective case series of 44 men (2018) evaluated hCG monotherapy (~2,000 IU weekly) in men with hypogonadal symptoms but testosterone >300 ng/dL. hCG monotherapy significantly improved testosterone levels, with symptom improvement reported in 50% of patients and no reported side effects or complications.[6] A 2022 study of 31 men with hypogonadal symptoms and testosterone >300 ng/dL found that hCG monotherapy led to subjective improvements in libido (80%), energy (79%), and erectile dysfunction (86%).
In women: fertility medicine
hCG (5,000–10,000 IU IM or 250 µg Ovidrel SC) triggers final follicular maturation and ovulation by mimicking the LH surge, typically 36–40 hours before egg retrieval in ART cycles or intercourse in ovulation induction cycles. This is a core component of virtually every ART protocol globally.[12]
The Compounding Restriction (2020)
The 2020 FDA ruling that hCG is not appropriate for compounding under Section 503A had significant clinical impact. The FDA’s determination: commercially available hCG products (Pregnyl, Novarel) adequately meet patient needs, making compounded hCG redundant under the Drug Quality and Security Act. Six of the 8 pharmacies surveyed that stopped making hCG cited the 2020 FDA mandate as the reason. Of the 75 pharmacies responding to survey, only 5 provided hCG (6.67%).[10]
The practical consequences were substantial: cost and access barriers increased significantly, particularly for men in rural areas. This created the market vacuum into which gonadorelin was positioned as an alternative — despite having a considerably weaker evidence base for TRT-adjunct use. 503B outsourcing facilities can still produce hCG in bulk for clinical use; commercial Pregnyl and Novarel remain available through specialty pharmacies.
Regulatory Status
| Jurisdiction/Context | Status |
|---|---|
| FDA — Men | ✅ Approved: hypogonadotropic hypogonadism, cryptorchidism (Pregnyl, Novarel) [12] |
| FDA — Women | ✅ Approved: ovulation induction, ART trigger (Pregnyl, Novarel, Ovidrel) |
| FDA — Weight loss | ⚠️ Explicitly fraudulent; prohibited marketing; no evidence of efficacy [11] |
| Compounding — 503A | ❌ Prohibited since 2020 |
| Compounding — 503B | Permitted (outsourcing facilities) |
| WADA | ❌ Prohibited in men at all times (S2); permitted in women (only in-competition permitted) |
Safety
Well-established in approved use
hCG at therapeutic doses has a well-documented safety profile spanning decades of use in millions of patients. Common effects include injection site reactions (mild), gynecomastia in men (from aromatisation of elevated intratesticular testosterone to oestradiol — manageable with monitoring), increased hematocrit (relevant for men; periodic CBC monitoring recommended), fluid retention (temporary), and occasional headache or fatigue.
In men: acne from elevated androgens; mild testicular swelling from Leydig cell stimulation; LH assay interference (commercial LH assays may not fully distinguish hCG from LH, so serum LH values may be unreliable during hCG treatment).
In women: the primary serious risk is ovarian hyperstimulation syndrome (OHSS) — when ovarian response is excessive; severity ranges from mild (bloating, discomfort) to severe (respiratory compromise, thromboembolism). Multiple gestation risk also exists when used for ovulation induction.
The weight-loss safety concern
⚠️ hCG for weight loss, typically in the context of extremely low calorie diets (500 kcal/day), poses risk not from hCG itself but from the severely restrictive diet protocols. The FDA specifically warns that these products are fraudulent and potentially harmful.[11] Multiple RCTs have shown hCG produces no weight loss advantage over placebo when caloric restriction is matched.
Comparison with Gonadorelin as TRT Adjunct
| Feature | hCG | Gonadorelin (pulsatile) |
|---|---|---|
| Mechanism | Direct LH receptor agonist (acts on Leydig cells) | GnRH receptor agonist (acts on pituitary → LH + FSH) |
| Stimulates FSH | ❌ No | ✅ Yes (via pituitary) |
| Requires intact pituitary | No | Yes |
| Dosing frequency | 2–3× weekly | Every 90–120 min (pump) or daily (controversial SC injection) |
| Evidence base (TRT adjunct) | Multiple retrospective studies; established protocols [5] | Small open-label study; mechanistically plausible |
| Long-term evidence | Decades of use | Not established in this context |
| Half-life | 24–37 hours | 2–10 minutes |
| US availability | FDA-approved (Pregnyl, Novarel); compounding restricted | Compounding pharmacies; US brand discontinued |
Common Misconceptions
“hCG is a natural, bioidentical hormone so it’s safe for weight loss.”
⚠️ This combines two falsehoods. “Natural” does not mean safe or effective for any given indication. More directly: hCG has zero evidence of efficacy for weight loss — the weight lost on “hCG diet” protocols is entirely attributable to the 500 kcal/day caloric restriction imposed alongside it. The FDA considers this use fraudulent.[11]
“Elevated hCG in men is harmless if they’re using it for TRT.”
⚠️ Elevated hCG in men requires evaluation for germ cell tumours even if they are using exogenous hCG. Unexpectedly high levels warrant tumour evaluation regardless of reported pharmaceutical use.
“hCG is the same as LH.”
They act through the same receptor but are structurally distinct. The critical difference is half-life — 25 minutes for LH versus 24–37 hours for hCG. This is why hCG produces steady, sustained Leydig cell stimulation while LH produces pulsatile testosterone peaks that would require continuous infusion to replicate therapeutically.[1]
“Low-dose hCG is enough for complete spermatogenesis.”
hCG alone stimulates LH-mediated testosterone production. Full spermatogenesis requires FSH in addition to intratesticular testosterone. For men who need to induce spermatogenesis from azoospermia, adding FSH alongside hCG substantially improves outcomes: 86% spermatogenesis with hCG + FSH vs. 40% with hCG alone in the 2024 meta-analysis.[9]
Frequently Asked Questions
Is hCG covered by insurance for hypogonadism?
Coverage varies substantially by insurer and indication. For an established diagnosis of hypogonadotropic hypogonadism or cryptorchidism (FDA-approved indications), there is a stronger basis for coverage. Off-label use for TRT adjunct/fertility preservation is less consistently covered.
Can hCG restart natural testosterone production after stopping TRT?
hCG can help reactivate the HPG axis after TRT-induced suppression by stimulating testicular steroidogenesis while the pituitary recovers. However, it does not directly restart pituitary LH/FSH production — that recovery occurs on its own timeline (weeks to months) after removing exogenous testosterone. hCG can make the transition more comfortable by providing LH-like activity during the recovery window.
What is the difference between Pregnyl and Ovidrel?
Pregnyl is urinary-derived hCG standardised in International Units. Ovidrel is recombinant choriogonadotropin alfa, standardised by mass (250 µg ≈ 6,500 IU of biological activity). They have equivalent clinical efficacy for ovulation triggering in ART. Ovidrel is generally preferred for ART because of its consistent recombinant manufacturing and prefilled delivery; Pregnyl/Novarel are widely used for male hypogonadism protocols.[12][13]
Is hCG the same as the “pregnancy hormone” in home test kits?
Yes. Pregnancy tests detect hCG in urine. Men who are using pharmaceutical hCG (including for TRT purposes) will produce a positive result on a home pregnancy test — this is pharmacologically expected and not a cause for alarm, though it can be alarming if encountered unexpectedly.
Key Takeaways
- hCG is a well-characterised endogenous glycoprotein hormone with FDA-approved indications, not a research peptide. Its biology spans reproductive physiology, early pregnancy maintenance, placental development, and tumour marker status. It has been used clinically for decades.[1][2]
- The β-CTP extension that distinguishes hCG from LH is the molecular basis for its dramatically longer half-life (24–37 hours vs. 25–30 minutes for LH), which makes it pharmacologically practical in a way that LH itself is not.
- In men with hypogonadotropic hypogonadism seeking fertility, hCG-based therapy (with or without FSH) is the gold-standard pharmacological approach with a robust evidence base — including 2024 meta-analysis data showing >98% testosterone response and 86% spermatogenesis with combined therapy.[9]
- The TRT-adjunct use for fertility preservation has a meaningful but modest evidence base — retrospective studies showing no azoospermia and maintained pregnancy potential at low doses (500 IU every other day).[5]
- ⚠️ The 2020 compounding restriction created significant access gaps and drove practitioners toward gonadorelin as an alternative, despite gonadorelin having a considerably weaker evidence base for this specific indication.[10]
- ⚠️ The weight-loss use is explicitly FDA-determined fraud — no evidence supports efficacy beyond caloric restriction, and the protocols involve potentially dangerous very-low-calorie diets.[11]
- ⚠️ Elevated serum hCG in any non-pregnant man is a clinically significant finding requiring evaluation for testicular germ cell tumours, regardless of whether the individual has also been using pharmaceutical hCG.
References
Biochemistry and Biology
- Cole LA. New discoveries on the biology and detection of human chorionic gonadotropin. Reproductive Biology and Endocrinology. 2009. PMC2649930
- Cole LA. Biological functions of hCG and hCG-related molecules. Reproductive Biology and Endocrinology. 2010. PMC2936313
- Human chorionic gonadotropin. Wikipedia. en.wikipedia.org/wiki/Human_chorionic_gonadotropin
Male Hypogonadism and Fertility
- Indications for the use of human chorionic gonadotropic hormone for the management of infertility in hypogonadal men. PMC6087849
- Coolen JM, et al. Low dose human chorionic gonadotropin prevents azoospermia and maintains fertility in hypogonadal men on testosterone replacement therapy. Fertility and Sterility. 2010.
- Human Chorionic Gonadotropin monotherapy for the treatment of hypogonadal symptoms in men with total testosterone >300 ng/dL. PMC6844348
- Esteves SC, et al. Human chorionic gonadotropin-based clinical treatments for infertile men with non-obstructive azoospermia. Andrology. 2025. doi: 10.1111/andr.70003
- Efficacy of hCG in restoring spermatogenesis in men using non-prescribed androgens (harm reduction clinic, Netherlands). F&S Reports. 2025.
CHH Spermatogenesis (Meta-Analysis)
- 2024 systematic review and meta-analysis: 5,328 HH patients, hCG-based therapy. Referenced in Esteves 2025 (Andrology). doi: 10.1111/andr.70003
Compounding Access
- The availability of gonadotropin therapy from FDA-approved pharmacies for men with hypogonadism and infertility. PMC10083688
Regulatory
- FDA. Avoid dangerous hCG diet products. Consumer update. fda.gov
- Pregnyl (chorionic gonadotropin) prescribing information. Merck & Company. Revised March 2023.
- Ovidrel (choriogonadotropin alfa injection) prescribing information. EMD Serono. Revised December 2023.
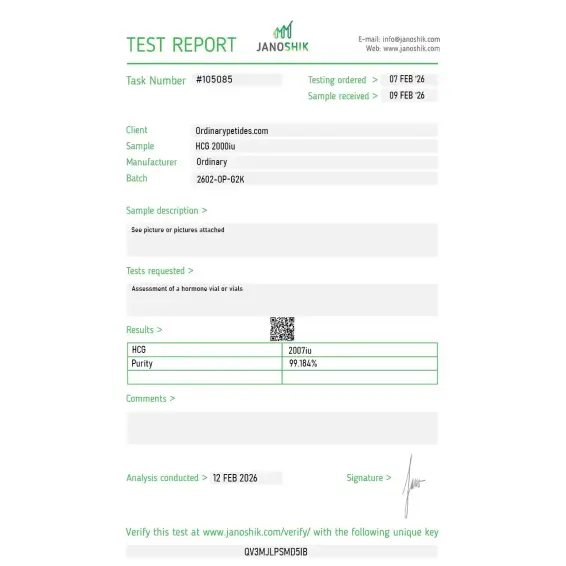
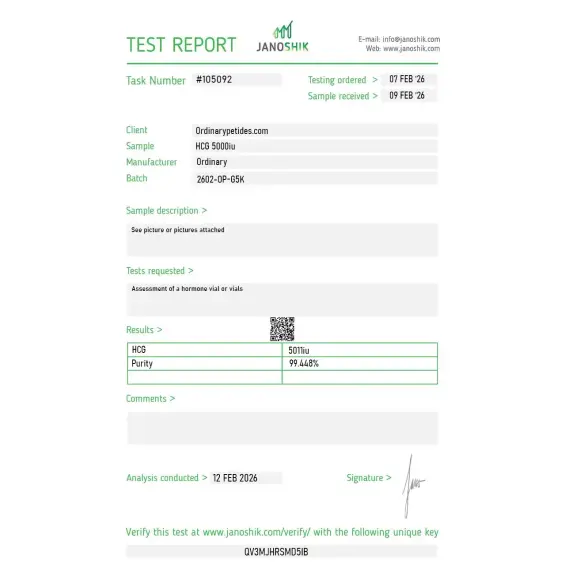
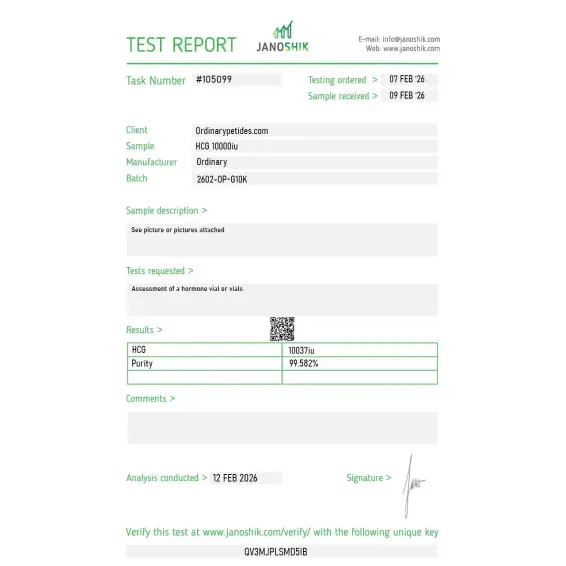
Certificate of Analysis
Independent test reports are available for HCG 2,000 IU, 5,000 IU, and 10,000 IU batches. These reports provide batch-level documentation and analytical verification information for research reference.



Based on 1 reviews
5.0
The α/β heterodimer architecture is what we actually study — HCG shares its α-subunit with LH, FSH, and TSH, and the β-subunit is what confers receptor specificity. For glycoprotein-hormone-family pharmacology where you're dissecting how the shared α and the distinct β contribute to receptor selectivity, HCG is the standard reference for the LH/CG-receptor-binding β. The material behaved as the intact heterodimer should in our assays.
Strictly speaking, not in the usual sense of a short peptide. HCG is a glycoprotein hormone.
It can. In some men, HCG can increase testosterone because it mimics the action of LH on Leydig cells in the testes.
Sometimes, yes. That is one reason it is used in certain fertility-preservation strategies. But it is not a universal guarantee.
Yes. One of its best-established uses in women is as an ovulation trigger in fertility treatment after appropriate ovarian stimulation.
No convincing evidence supports HCG as an effective weight-loss treatment.
No. WADA prohibits HCG in male athletes.
Human Chorionic Gonadotropin (HCG) is a glycoprotein hormone — not technically a peptide in the short-chain sense — produced naturally by the placenta during pregnancy, where it sustains the corpus luteum and maintains progesterone production during the first trimester. It is a large two-chain protein of approximately 36,700 daltons, structurally related to LH, FSH, and TSH, sharing the same alpha subunit with a unique beta subunit that confers its biological specificity. Pharmaceutical HCG is derived either from the urine of pregnant women (urinary HCG) or produced through recombinant DNA technology. It has been in clinical use since the 1930s and has FDA-approved indications. It is also one of the most misused substances in both the fertility and performance enhancement communities, and its regulatory status has become increasingly complex in the United States since 2020.
HCG binds to and activates the LH/HCG receptor — the same receptor that LH (luteinizing hormone) acts upon — because its beta subunit is structurally homologous to LH. In men this directly stimulates Leydig cells in the testes to produce testosterone, and supports the intratesticular testosterone levels needed for spermatogenesis. In women it triggers the LH surge necessary for final oocyte maturation and ovulation. Because it mimics LH so closely but has a much longer half-life — approximately 24 to 36 hours versus LH's 20 to 60 minutes — a single HCG injection produces a prolonged, robust gonadal stimulation. Unlike gonadorelin which works upstream at the hypothalamic-pituitary level, HCG bypasses the HPG axis entirely and acts directly on the gonads.
HCG has several FDA-approved indications. In women it is used to trigger final follicular maturation and ovulation in assisted reproductive technologies including IVF and intrauterine insemination, typically as a single 5,000 to 10,000 IU injection. In men it is approved for hypogonadotropic hypogonadism — where the pituitary fails to produce adequate LH — to stimulate testicular testosterone production and spermatogenesis. It is also approved for prepubertal cryptorchidism to stimulate testicular descent. Beyond formal indications it is widely used off-label in men on TRT to maintain testicular volume and function, prevent testicular atrophy, preserve fertility, and maintain intratesticular testosterone levels that support downstream androgen production — the same functional role as gonadorelin but acting directly at the testis level rather than upstream.
This is the most practically relevant comparison in contemporary men's health. HCG acts directly on Leydig cells mimicking LH, stimulating testicular testosterone and maintaining testicular size and spermatogenesis during TRT or after anabolic suppression. Gonadorelin works further upstream — stimulating the pituitary to release LH and FSH, thereby activating the full HPG axis. HCG's practical advantages are its longer half-life allowing less frequent dosing typically two to three times per week, established subcutaneous self-injection protocols, and a robust evidence base. Its limitation is that it does not stimulate pituitary FSH production — which drives spermatogenesis — directly, meaning fertility support may be incomplete for some men. It also does not exercise or maintain the pituitary component of the HPG axis. Gonadorelin is more physiologically complete but pharmacokinetically demanding. In clinical practice HCG remains the more commonly used and better-validated option for most men.
This changed significantly in 2020. The FDA ruled that HCG is a biological product rather than a drug, requiring it to transition to a BLA (Biologics License Application) regulatory pathway. As of October 2023 compounding pharmacies could no longer compound HCG under DSHEA and traditional pharmacy compounding exemptions. Approved pharmaceutical HCG products — such as Pregnyl, Novarel, and the recombinant choriogonadotropin alfa Ovidrel — remain available by prescription. However the practical effect is that the compounded HCG vials that were widely used in men's health and fertility clinics at low cost have become significantly less accessible, pushing many practitioners toward alternatives including gonadorelin and kisspeptin analogs. Pharmaceutical grade HCG by prescription from a licensed physician remains legal.
HCG is generally well tolerated at therapeutic doses. The most common effects in men are local injection site reactions, mild fluid retention, and acne consistent with elevated testosterone. Gynecomastia can develop if HCG elevates testosterone to levels that undergo significant aromatization to estradiol — monitoring estrogen levels and using aromatase inhibitors when needed is standard practice. At higher doses testicular discomfort or aching is reported. Prolonged or very high dose HCG use can cause Leydig cell desensitization — the same paradoxical downregulation seen with sustained GnRH agonists — reducing the testicular response over time. In women ovarian hyperstimulation syndrome (OHSS) is the most serious risk — potentially life-threatening in severe cases with massive fluid shifts, ovarian enlargement, and thromboembolism — requiring careful monitoring in fertility treatment settings. Multiple pregnancies are a significant risk when used for ovulation induction.
Men with androgen-sensitive prostate cancer or elevated PSA should not use it as testosterone stimulation can drive disease progression. Men with precocious puberty should not use it. Women with primary ovarian failure — where the ovaries cannot respond to gonadotropin stimulation — will not benefit. Those with ovarian cysts not caused by polycystic ovarian disease should not receive it for fertility purposes. People with a history of or risk factors for thromboembolism face elevated risk during fertility treatment particularly if OHSS develops. Anyone with hypersensitivity to HCG or its components should not use it. Pregnant women should not use it once pregnancy is confirmed.





