

Gonadorelin Acetate
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Gonadorelin Acetate: A Smart Endocrine Peptide Where Rhythm Changes Everything
Gonadorelin acetate is not a "peptide for boosting testosterone," but a synthetic form of GnRH — the upstream regulatory signal for the LH and FSH axis.
In clinical and research contexts, it was valued most in settings where the goal was not to "push hormones up in general," but to precisely reproduce a physiological rhythm: it was exactly under pulsatile administration that it showed its most convincing results, including ovulation induction in hypothalamic amenorrhea and use in diagnostic testing.
And that is where its main intrigue lies: with gonadorelin, what matters is not only the molecule itself, but also how exactly it is delivered — with this peptide, rhythm really does decide everything. This is not a universal wellness tool, but a finely tuned endocrine mechanism for very specific tasks.
This is exactly the kind of peptide that becomes interesting to people who look at biology beyond the level of "let's raise something hormonal and hope for the best."
Practical Takeaway
If you want to study not hype, but genuinely intelligent peptides with strong physiological logic, gonadorelin acetate absolutely deserves attention.
Gonadorelin Acetate (GnRH, Pulsatile GnRH): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Gonadorelin acetate is synthetic gonadotropin-releasing hormone (GnRH) — a perfect copy of the decapeptide that the hypothalamus secretes every 90–120 minutes to drive the entire reproductive hormonal axis. Unlike every other compound in this article series, it is not a synthetic analogue modified to improve potency or stability. It is the endogenous molecule itself, made by solid-phase peptide synthesis.
This identity with the natural hormone is gonadorelin’s most important characteristic — and it gives the compound a pharmacological story unlike anything else in this series. The same molecule, delivered in two different patterns, produces opposite biological effects:
- Pulsatile delivery (mimicking the natural hypothalamic pulse pattern) → sustains gonadotropin secretion → maintains or restores fertility and sex hormone production
- Continuous delivery → desensitises GnRH receptors → suppresses gonadotropin secretion → chemical castration
This principle — discovered by Ernst Knobil and colleagues in 1978 — underlies not only the therapeutic use of pulsatile gonadorelin for hypogonadotropic hypogonadism and fertility, but also the clinical exploitation of GnRH agonists (leuprolide, goserelin, triptorelin) for prostate cancer, endometriosis, and precocious puberty through continuous receptor downregulation. Gonadorelin acetate is the only compound in this series with a Nobel Prize in its backstory: Roger Guillemin and Andrew Schally shared the 1977 Nobel Prize in Physiology or Medicine for elucidating the structure of GnRH.[1][2]
| At a glance | |
|---|---|
| Generic name | Gonadorelin acetate (USAN, BAN) |
| Also known as | GnRH, LHRH, gonadoliberin, luteinising hormone-releasing hormone |
| Structure | Decapeptide: pGlu-His-Trp-Ser-Tyr-Gly-Leu-Arg-Pro-Gly-NH&sub2; |
| Molecular weight | ~1,183 Da |
| Natural identity | Bioidentical to endogenous human GnRH |
| Half-life | 2–10 minutes (distribution); 10–40 minutes (terminal) |
| Former US brand names | Factrel (diagnostic, Wyeth); Lutrepulse (pulsatile pump, Ortho Pharmaceutical) |
| Current US status | Both brands discontinued; available from compounding pharmacies |
| Compounding status | ⚠️ Contested — regulatory position unclear under 503A/503B frameworks |
| Off-label use (current) | TRT adjunct (fertility preservation, testicular atrophy); CHH/Kallmann syndrome |
| WADA | ❌ Prohibited at all times (S2 — Peptide Hormones) |
| Nobel Prize | Guillemin and Schally, 1977, for GnRH structure elucidation |
The Biological Foundation: The GnRH Pulse Generator
Discovery and structure
GnRH was isolated and structurally characterised in the early 1970s in one of the most intense scientific competitions in modern neuroendocrinology. Burgus et al. (1971) and Guillemin’s laboratory elucidated the structure from ovine hypothalami; Schally’s team processed over 160,000 pig hypothalami to isolate the microgram quantities needed for structural analysis. The sequence established was the decapeptide pGlu-His-Trp-Ser-Tyr-Gly-Leu-Arg-Pro-Gly-NH&sub2;. Both ends are protected against proteolytic degradation — though not enough to give it a long half-life: GnRH is degraded within minutes in plasma.[1][2]
The critical 1978 discovery: pulsatile vs. continuous
The most important finding about GnRH was not its structure but its required delivery pattern. Belchetz, Knobil, and colleagues demonstrated in 1978, in rhesus monkeys, that continuous GnRH infusion paradoxically suppressed LH and FSH, while intermittent hourly pulses maintained normal gonadotropin output.[3] Intermittent secretion of GnRH results in the synthesis and release of FSH and LH; continuous GnRH infusion results in a cessation of gonadotropin release through down-regulation (internalisation) and desensitisation (uncoupling) of GnRH receptors.[4]
Chemistry: Why the Acetate Salt Matters
Gonadorelin exists in several salt forms: gonadorelin hydrochloride (used in Factrel, diagnostic); gonadorelin acetate (gonadorelin diacetate tetrahydrate, used in Lutrepulse); and free alcohol gonadorelin used in some European products. The acetate salt was developed specifically for Lutrepulse to improve purity, stability, and tolerability for prolonged pulsatile pump delivery. The gonadorelin acetate drug substance was found to be stable for at least 12 months when stored at 24°C in 50% relative humidity.[11] Reports of adverse reactions after pulsatile gonadorelin hydrochloride therapy suggested that high-purity material may be advantageous in controlling unwanted side effects — making the salt distinction clinically relevant for prolonged infusion protocols.
Mechanism of Action
The GnRH receptor
GnRH receptor is a Gq/11-coupled G-protein receptor expressed on anterior pituitary gonadotroph cells. Binding triggers phospholipase C activation → IP&sub3; and DAG → intracellular Ca²+ release → protein kinase C activation → synthesis and secretion of LH and FSH. The pulsatile requirement is a consequence of receptor regulation: sustained GnRH receptor activation leads to receptor internalisation (downregulation) and uncoupling (desensitisation), progressively reducing gonadotropin output. Periods of GnRH absence allow receptor recovery and resensitisation. The natural hypothalamic pulse generator delivers GnRH every 60–120 minutes, which maintains receptor responsiveness while preventing desensitisation.
The HPG axis in sequence
Gonadorelin’s effect operates through the complete hypothalamic-pituitary-gonadal (HPG) axis: Gonadorelin → pituitary GnRH receptor → LH + FSH release → LH → Leydig cells → testosterone synthesis; FSH → Sertoli cells → spermatogenesis support. Unlike hCG (which acts directly on Leydig cells mimicking LH only), pulsatile gonadorelin stimulates both LH and FSH through the pituitary’s own regulatory machinery. This preserves the normal LH:FSH ratio and pituitary regulatory function — a meaningful advantage for restoring complete reproductive physiology.
History of Approved Use and Discontinuation
Factrel (gonadorelin hydrochloride, diagnostic)
Factrel was FDA-approved from 1978 as a diagnostic agent for assessing pituitary gonadotroph function. The test protocol: baseline LH drawn, 100 µg gonadorelin administered IV or SC, LH and FSH measured at intervals. An LH increase >10 mIU/mL indicates an intact pituitary gonadotroph response, helping distinguish pituitary-origin from hypothalamic-origin hypogonadism. It has since been commercially discontinued in the US.[12]
Lutrepulse (gonadorelin acetate, pulsatile pump)
Lutrepulse was FDA-approved for treatment of primary hypothalamic amenorrhea — women with absent periods caused by GnRH deficiency rather than pituitary or ovarian failure. The treatment required a portable subcutaneous infusion pump delivering 5–20 µg gonadorelin every 90–120 minutes around the clock. Success rates were clinically meaningful: ovulation was induced in approximately 75–90% of appropriately selected women. Because of the complexity of administration, this treatment modality was rarely used, and Lutrepulse is no longer available in the United States.[13]
Current regulatory position (compounding)
The regulatory position of compounded gonadorelin in the US is genuinely complicated and contested. Compounding pharmacies are producing gonadorelin on the basis that it has been a component of FDA-approved drug products. However, some regulatory authorities argue that discontinued FDA-approved products do not automatically qualify for compounding, and the use of gonadorelin as a TRT adjunct represents off-label use of a compounded version of a discontinued product — involving multiple layers of regulatory uncertainty. Veterinary GnRH products (Cystorelin, Fertagyl, Gonabreed) are legally distinct from human compounding and do not confer compounding rights for human use.
Regulatory and Legal Status
| Jurisdiction/Context | Status |
|---|---|
| FDA — human Factrel | Commercially discontinued |
| FDA — human Lutrepulse | Commercially discontinued |
| FDA — veterinary products | ✅ Currently approved (Cystorelin, Factrel cattle, Fertagyl, Gonabreed) — for dairy/beef cattle only |
| Compounding (503A) | ⚠️ Legally contested; many pharmacies compound it; regulatory basis disputed |
| Compounding (503B) | ❌ Not on 503B bulks list |
| WADA | ❌ Prohibited at all times — S2 (Peptide Hormones, Growth Factors, Related Substances) |
| Europe | Lutrelef (Ferring) and other pulsatile pump products remain available in some European markets |
Clinical Evidence
Hypogonadotropic hypogonadism and Kallmann syndrome: the strongest evidence base
The strongest and most established human evidence for gonadorelin is in congenital hypogonadotropic hypogonadism (CHH) — a condition caused by GnRH deficiency from birth (with or without anosmia; the anosmia-associated form is Kallmann syndrome). These patients have functional pituitary glands but lack hypothalamic GnRH drive. Pulsatile gonadorelin is the most physiologically rational treatment, directly addressing the primary defect.
A retrospective study by Huang et al. (2015) in China compared pulsatile GnRH (10 µg every 90 min) with continual HCG/HMG therapy in 92 CHH patients, concluding that pulsatile gonadorelin induced higher and earlier spermatogenesis than continual HCG/HMG therapy.[7] A 2019 study confirmed that the pulsatile gonadorelin pump induced earlier spermatogenesis than cyclical gonadotropin therapy.[8] A 2025 retrospective study in 155 CHH patients confirmed these findings and added that pulsatile GnRH produced more beneficial testicular volume development than gonadotropin therapy.[9] For patients who fail first-line gonadotropin therapy, switching to pulsatile GnRH can rescue the response: sperm was detected in 17/28 patients (60.7%) who had previously failed one year of HCG/HMG therapy.[10]
Spermatogenesis rates of 60–85% across studies represent the most compelling evidence for this therapy.
Primary hypothalamic amenorrhea (women)
The original Lutrepulse indication: women with absent menstruation due to hypothalamic GnRH deficiency. Pulsatile gonadorelin restores ovulatory cycling in approximately 75–90% of patients. Evidence is from Phase 2/3 trials conducted in the 1980s–1990s — the basis for Lutrepulse’s original FDA approval.[5][6]
TRT adjunct use (off-label, emerging)
The off-label use of compounded gonadorelin in men on testosterone replacement therapy has grown substantially since HCG compounding was restricted in the US. Exogenous testosterone suppresses the HPG axis at the hypothalamic-pituitary level, causing LH and FSH suppression, testicular atrophy, and suppressed spermatogenesis. Gonadorelin, by stimulating the pituitary directly, might maintain LH/FSH signalling to the testes even in the presence of exogenous testosterone.
The pharmacological challenge: exogenous testosterone produces high circulating androgen levels that suppress GnRH receptor sensitivity at the pituitary through steroid feedback mechanisms. Whether intermittent subcutaneous gonadorelin injection (without a proper pump) produces sufficient pulsatile stimulation to meaningfully maintain pituitary gonadotropin output against this backdrop is genuinely uncertain.
Clinical evidence summary
| Indication | Evidence level | Evidence quality |
|---|---|---|
| CHH/Kallmann (male spermatogenesis) [7]–[10] | Multiple clinical trials and retrospective cohorts | Moderate-high (50–85% spermatogenesis rates consistently) |
| Primary hypothalamic amenorrhea [5][6] | Phase 2/3 trials (1980s–1990s) | Moderate (Lutrepulse approval basis; not replicated in modern trials) |
| GnRH stimulation test | Extensive clinical experience | High — well-established diagnostic use |
| TRT adjunct (male) | Small open-label study | Very low; anecdotal/off-label |
| Post-cycle therapy | No controlled data | ❌ No evidence base |
Comparison: Gonadorelin vs. HCG vs. GnRH Analogues
| Feature | Gonadorelin (pulsatile) | HCG | GnRH analogues (continuous) |
|---|---|---|---|
| Acts at | Pituitary (GnRH-R) | Testis directly (LH-R) | Pituitary (GnRH-R, downregulates) |
| Stimulates FSH | ✅ Yes (through pituitary) | ❌ No | ❌ No — suppresses |
| Stimulates LH | Yes | Mimics LH directly | ❌ Suppresses |
| Preserves pituitary function | Yes | No (bypasses pituitary) | No (downregulates) |
| Requires intact pituitary | ⚠️ Yes — ineffective in pituitary damage | No | Yes (to be suppressed) |
| Delivery complexity | Pump required for true pulsatile effect | Simple SC injections 2–3× week | Depot injections or implants |
| Human evidence (TRT adjunct) | Very limited | Extensive | N/A (used to suppress) |
| Half-life | 2–10 minutes | 24–36 hours | Hours to days (synthetic analogues) |
The Delivery Problem: Why Pulsatility Matters
This is the central practical challenge with gonadorelin in current off-label use. The natural hypothalamic GnRH pulse generator delivers discrete pulses every 60–120 minutes. Lutrepulse and current CHH research protocols use pumps programmed to deliver 5–20 µg every 90 minutes subcutaneously, 24 hours a day, with needle replacement every 72 hours.
The subcutaneous injections prescribed as a TRT adjunct — typically 100–200 µg once or twice daily — do not replicate this pulse pattern. They are pharmacokinetically more analogous to frequent bolus injections than to true pulsatile delivery. Whether twice-daily injections in a high-androgen background maintain sufficient GnRH receptor cycling to produce meaningful FSH/LH output has not been validated. The GnRH receptor desensitisation concern applies: injections that are too frequent risk producing the same receptor downregulation as continuous delivery. The optimal protocol for this off-label indication remains undefined.
Safety
In approved pulsatile pump use
Injection site reactions (redness, swelling, bruising) are common. Tachyphylaxis (reduced response) can occur with very prolonged or inappropriately dosed therapy. Multiple gestation risk exists in women if ovulation is hyperstimulated. Rare anaphylaxis — more common with older, less pure formulations; reduced with gonadorelin acetate.[11]
In TRT-adjunct off-label use
The safety profile of twice-daily SC gonadorelin in testosterone-supplemented men is not formally characterised. No serious adverse events have been documented in the limited published experience. Long-term effects on pituitary GnRH receptor regulation in this context are not known.
In athletes (WADA context)
WADA prohibits gonadorelin because pulsatile administration could stimulate endogenous testosterone production above normal levels in athletes with suppressed HPG axes (from anabolic steroid use), providing both a recovery aid and a performance-enhancing mechanism. The MRPL (minimum required performance level) for detection is 2 ng/mL.
Common Misconceptions
“Gonadorelin is a safer version of testosterone.”
It is not a replacement for testosterone — it is a signal to the pituitary to produce LH/FSH, which then signals the gonads to produce testosterone. It only works if the pituitary and gonads are functional. In primary hypogonadism (testes damaged), gonadorelin produces no testosterone increase because the testes cannot respond to LH.
“A subcutaneous injection twice daily is equivalent to a pulsatile pump.”
⚠️ Pharmacokinetically, they are not equivalent. The Lutrepulse pump delivered 5–20 µg every 90 minutes — 16 pulses per day of short-acting stimulation separated by recovery intervals. Twice-daily 100–200 µg injections create two large pulses separated by 12-hour gaps, with potential for both receptor saturation (around the peak) and insufficient stimulation (at the trough). Whether this is pharmacologically adequate is genuinely unresolved.
“Because Factrel/Lutrepulse were FDA-approved, compounded gonadorelin is automatically legal.”
⚠️ The legal basis for compounding a discontinued FDA-approved drug is contested. Some compounding pharmacies operate on the basis that it qualifies as a component of an FDA-approved product; regulatory authorities have questioned this reasoning. The regulatory position is not settled.
“Gonadorelin can restore fertility in any man with low testosterone.”
Gonadorelin only works for hypogonadotropic (secondary) hypogonadism — where the deficit is in GnRH or LH/FSH signalling, not in testicular function itself. In primary hypogonadism (Klinefelter syndrome, testicular damage), the pituitary already secretes high LH/FSH and adding more GnRH will not improve testicular function.
Frequently Asked Questions
Is gonadorelin available in the US?
Not as an FDA-approved pharmaceutical product — both Factrel and Lutrepulse have been discontinued.[12][13] Compounding pharmacies make it, and many are prescribing and dispensing it, but the legal and regulatory position is contested.
What happened to HCG compounding that made gonadorelin popular?
The FDA restricted compounding of HCG after determining that commercially available HCG products (Pregnyl, Novarel) met patient needs, making compounded HCG redundant. This drove practitioners to seek alternatives. Gonadorelin emerged as the primary alternative, despite having a much weaker evidence base for the TRT-adjunct indication.
Can gonadorelin be used for post-cycle therapy (PCT) after anabolic steroid use?
This is biologically plausible — anabolic steroids suppress the HPG axis at the hypothalamic level, and administering pulsatile GnRH could help restart the axis from the hypothalamic level. However, no controlled clinical data exists for this specific application. Given the WADA prohibition and the lack of evidence, this remains speculative.
Is pulsatile gonadorelin available in Europe?
Yes — several European products (Lutrelef, Luforan, Lutamin) with pulsatile pump delivery remain available in some European markets and are used clinically for hypothalamic amenorrhea and CHH, consistent with established protocols.
Key Takeaways
- Gonadorelin is the endogenous GnRH molecule itself — its structure, mechanism, and biology are among the most thoroughly understood in reproductive endocrinology, with a Nobel Prize as part of its intellectual heritage.[1][2] It is categorically different from the synthetic peptide drug candidates throughout the rest of this series.
- ⚠️ The pulsatile vs. continuous pharmacology paradox is unique in pharmacology. The same molecule, delivered pulsatilely, stimulates the entire reproductive axis; delivered continuously, it suppresses it. Ignoring this means using the compound incorrectly.[3]
- The strongest evidence base is in CHH/Kallmann syndrome — where pulsatile pump therapy reliably induces spermatogenesis (60–85% success rates across multiple studies) and restores testicular function at the anatomical level.[7]–[10]
- ⚠️ The TRT-adjunct use (the dominant current off-label application) has a much weaker evidence base. It is mechanistically plausible but not pharmacokinetically validated for the twice-daily SC injection protocol in common use, and it has not been tested in controlled trials.
- ⚠️ The discontinuation of FDA-approved human gonadorelin products and its compounding from pharmacy-grade bulk material creates a regulatory and quality-control gap. Product purity, sterility, and accurate dose delivery from compounded preparations cannot be assumed equivalent to the original Lutrepulse formulation.
- WADA prohibition is appropriate and enforceable — gonadorelin can meaningfully stimulate endogenous testosterone production and has been detected in sports doping contexts.
References
Structure Elucidation (Nobel Prize)
- Schally AV, Arimura A, Baba Y, et al. Isolation and properties of the FSH and LH-releasing hormone. Biochemical and Biophysical Research Communications. 1971;43(2):393–399.
- Burgus R, Butcher M, Amoss M, et al. Primary structure of the ovine hypothalamic luteinizing hormone-releasing factor (LRF). Proceedings of the National Academy of Sciences. 1972;69(1):278–282.
Pulsatile Physiology
- Belchetz PE, Plant TM, Nakai Y, Keogh EJ, Knobil E. Hypophysial responses to continuous and intermittent delivery of hypothalamic gonadotropin-releasing hormone. Science. 1978;202(4368):631–633.
- Knobil E. The neuroendocrine control of the menstrual cycle. Recent Progress in Hormone Research. 1980;36:53–88.
Clinical Application — Reproductive Medicine
- Crowley WF Jr, McArthur JW. Stimulation of the normal menstrual cycle in Kallmann’s syndrome by pulsatile administration of luteinizing hormone-releasing hormone (LHRH). Journal of Clinical Endocrinology and Metabolism. 1980;51(1):173–175.
- Hoffman AR, Crowley WF Jr. Induction of puberty in men by long-term pulsatile administration of low-dose gonadotropin-releasing hormone. New England Journal of Medicine. 1982;307(20):1237–1241.
CHH/Kallmann Spermatogenesis Studies
- Huang B, Mao J, Xu H, et al. Spermatogenesis of pulsatile gonadotropin-releasing hormone infusion versus gonadotropin therapy in male idiopathic hypogonadotropic hypogonadism. Zhonghua Yi Xue Za Zhi. 2015;95:1568–1571.
- Zhang L, Cai K, Wang Y, et al. The Pulsatile Gonadorelin Pump Induces Earlier Spermatogenesis Than Cyclical Gonadotropin Therapy in Congenital Hypogonadotropic Hypogonadism Men. American Journal of Men’s Health. 2019;13(1). PMC6775549
- Comparison of outcomes between pulsatile GnRH and combined gonadotropin therapy in CHH (155-patient retrospective cohort). Reproductive Biology and Endocrinology. 2025. PMC11927256
- Pulsatile GnRH therapy for spermatogenesis in CHH patients who had poor response to combined gonadotropin therapy (28-patient rescue cohort). Archives of Endocrinology and Metabolism. 2024. PMC11156179
Gonadorelin Acetate Formulation
- Stability and purity profile of gonadorelin acetate. Pharmaceutical Research. 1991. PMID: 1980667
Regulatory
- Gonadorelin acetate (Lutrepulse). FDA drug information. [Discontinued].
- Gonadorelin hydrochloride (Factrel). FDA drug information. [Discontinued].
Key Investigators
- Andrew Schally, PhD — Tulane University; Nobel Prize in Physiology or Medicine (1977) for elucidation of GnRH structure; seminal isolation and characterisation of GnRH from porcine hypothalami.
- Roger Guillemin, MD, PhD — Salk Institute; Nobel Prize in Physiology or Medicine (1977) shared with Schally; independent elucidation of GnRH structure from ovine hypothalami.
- Ernst Knobil, PhD — University of Pittsburgh; established the pulsatile GnRH paradigm through rhesus monkey studies (1978); National Medal of Science recipient.
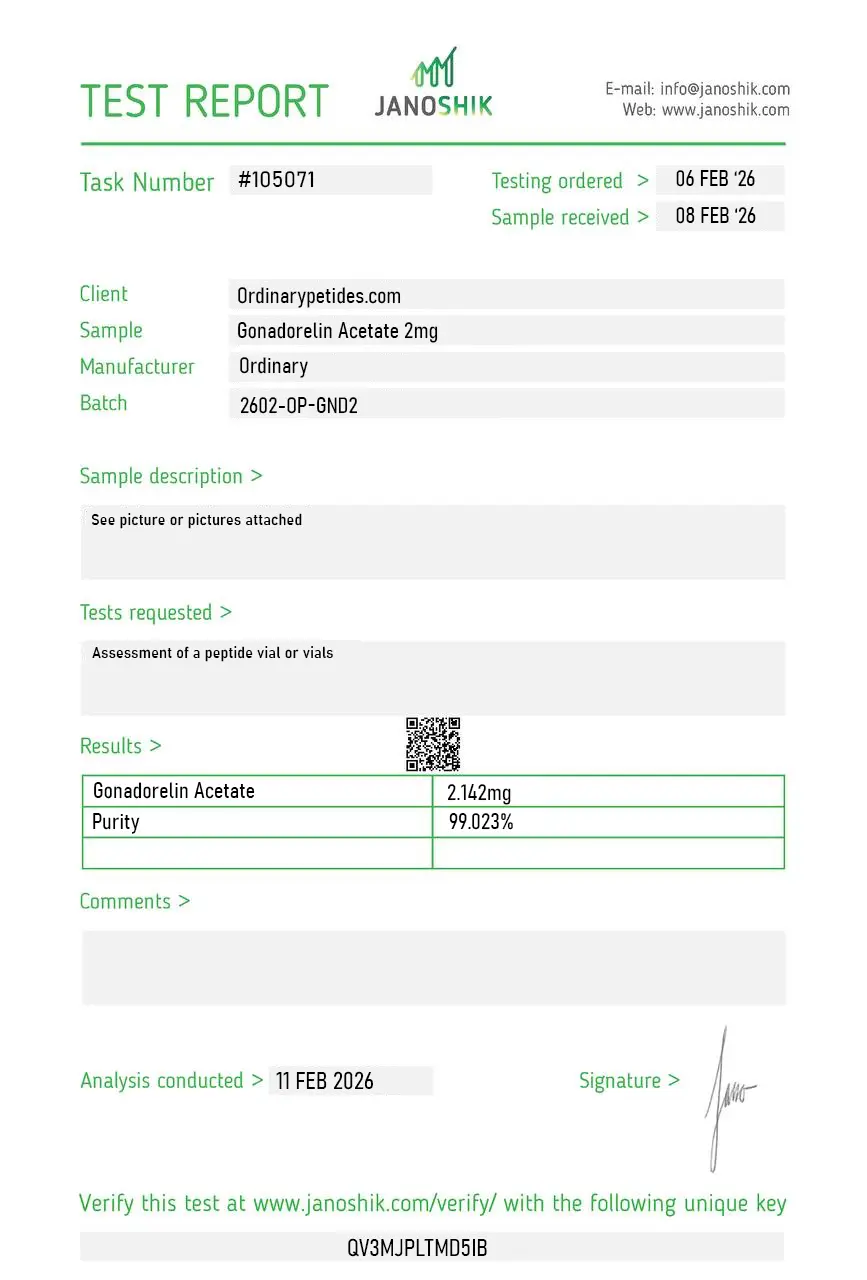
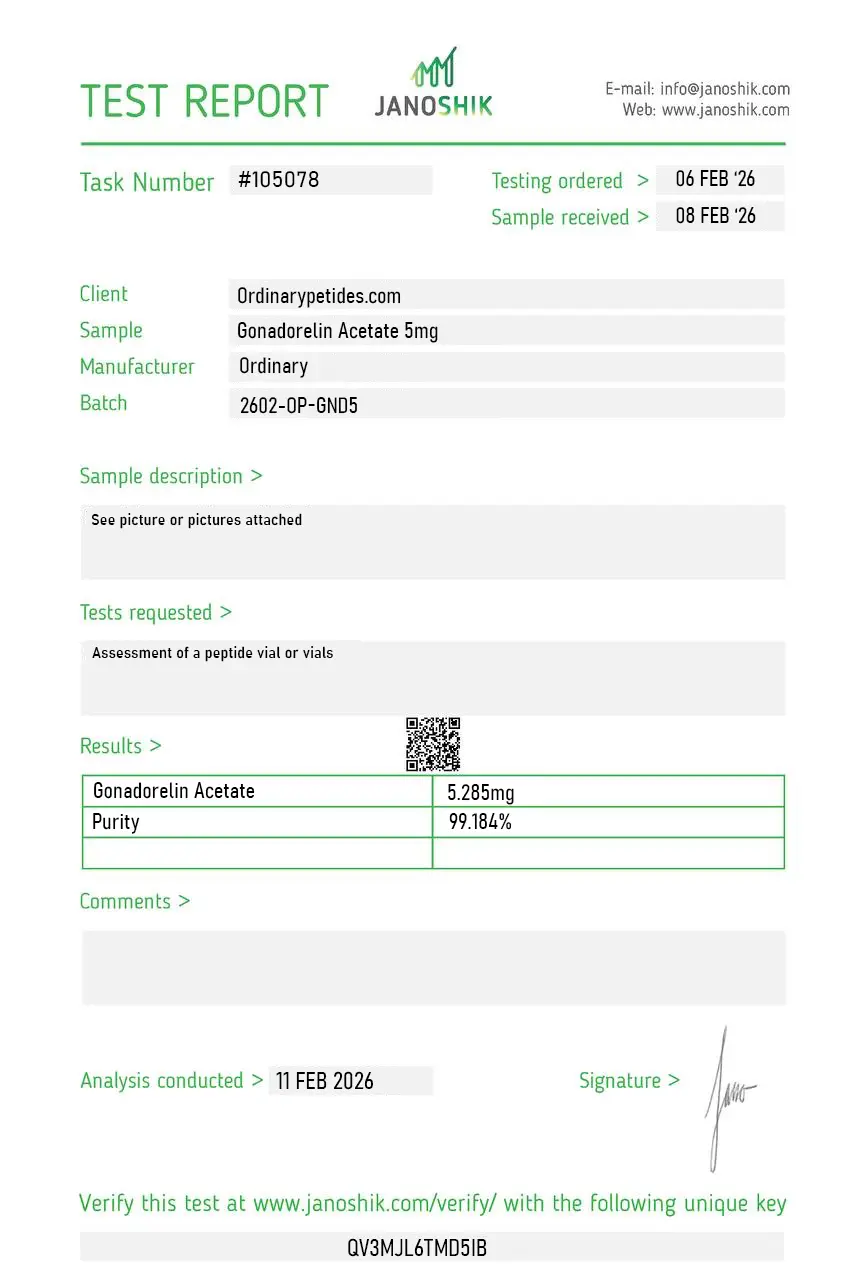
Certificate of Analysis
Independent test reports are available for Gonadorelin Acetate 2mg and 5mg batches. These reports provide batch-level documentation and analytical verification information for research reference.
Based on 1 reviews
5.0
The pulsatile-versus-continuous paradigm is the entire reason gonadorelin is a teaching-grade reference — native GnRH delivered in pulses stimulates gonadotroph LH/FSH release, but continuous exposure desensitizes and downregulates the receptor, which is the mechanism the GnRH-agonist drugs exploit therapeutically. For demonstrating that frequency-dependent receptor behavior in pituitary cell culture, gonadorelin is the canonical tool because it IS the native sequence. The material gave the expected pulse-dependent gonadotropin response in our assays.
Yes. Gonadorelin acetate is a decapeptide and a synthetic version of the body's natural GnRH (gonadotropin-releasing hormone).
No. It does not raise testosterone directly. Instead, it stimulates the release of LH and FSH, which may then influence testosterone production if the hormonal axis is functioning properly.
Its strongest evidence is in pulsatile ovulation induction for hypothalamic amenorrhea and in certain diagnostic GnRH stimulation tests.
No. A human product existed historically, but according to available official sources, it was withdrawn for commercial reasons, and there is currently no approved U.S. product for that purpose.
No. That would be too broad a claim. Gonadorelin has a much narrower and more specific endocrine role than many marketing claims suggest.
No. WADA prohibits gonadorelin and other GnRH agonists in sport.
The key point is that gonadorelin acetate is not a universal "hormone balance" peptide. It is a specialized endocrine tool used for specific reproductive and diagnostic purposes.
Gonadorelin acetate is the diacetate salt form of gonadorelin — a synthetic decapeptide that is chemically identical to endogenous gonadotropin-releasing hormone (GnRH), the peptide produced by the hypothalamus that serves as the master upstream regulator of the reproductive hormonal axis. It has been in medical use since at least 1978, when it became available under the brand name Factrel. It is used diagnostically to assess hypothalamic-pituitary function, therapeutically to induce ovulation and treat hypogonadotropic hypogonadism, and more recently in men's health and bodybuilding contexts as a means of maintaining testicular function during or after testosterone replacement therapy. Unlike GnRH analogs such as leuprolide, goserelin, or nafarelin — which are modified to resist degradation and produce continuous GnRH receptor stimulation leading to paradoxical suppression of LH and FSH — gonadorelin is bioidentical and requires pulsatile administration to mimic the natural hypothalamic signal and produce its intended stimulatory effects.
Gonadorelin binds to GnRH receptors on gonadotrope cells in the anterior pituitary gland, triggering release of both luteinizing hormone (LH) and follicle-stimulating hormone (FSH) into circulation. LH then acts on Leydig cells in the testes to stimulate testosterone production and on the ovaries to trigger ovulation. FSH stimulates spermatogenesis in men and follicular development in women. The critical pharmacological principle governing gonadorelin's use is that its stimulatory effects depend entirely on pulsatile administration — intermittent exposure that mimics the natural 60 to 120 minute hypothalamic pulse pattern. Continuous or sustained exposure to gonadorelin — or to longer-acting GnRH analogs — desensitizes and downregulates GnRH receptors on pituitary gonadotropes, paradoxically suppressing LH, FSH, and ultimately sex hormone production. This is the mechanism exploited therapeutically by GnRH agonists used to treat prostate cancer and endometriosis. Gonadorelin's very short half-life of 2 to 10 minutes for distribution and 10 to 40 minutes terminal half-life makes it naturally pulsatile when injected in standard doses.
Gonadorelin has several well-established uses. As a diagnostic agent a single 100 mcg injection — the Factrel test — measures the LH and FSH response to assess pituitary gonadotrope function, helping diagnose hypothalamic amenorrhea, hypogonadotropic hypogonadism, delayed puberty, and pituitary failure after surgery or radiation. Therapeutically, pulsatile subcutaneous infusion via portable pump at doses of 5 to 20 mcg per pulse every 90 to 120 minutes is the gold-standard treatment for hypothalamic amenorrhea and hypogonadotropic hypogonadism including Kallmann syndrome — conditions where the hypothalamus fails to produce adequate GnRH. It stimulates ovulation for fertility treatment in women with GnRH deficiency. It has been studied for cryptorchidism (undescended testes) and delayed puberty in boys. Importantly, it is approved and available in multiple countries but notably is not currently available for clinical use in humans in the United States, where the approved brand Factrel was discontinued.
This is the contemporary context in which gonadorelin most commonly appears in wellness and performance communities. Men on testosterone replacement therapy (TRT) suppress their own LH and FSH through negative feedback, leading to testicular atrophy, reduced sperm production, and impaired fertility. Gonadorelin administered in small pulsatile subcutaneous injections — typically 100 mcg twice daily — mimics the natural hypothalamic pulse and maintains pituitary stimulation of the testes, preserving testicular volume, spermatogenesis, and endogenous testosterone production alongside exogenous TRT. This is conceptually superior to the commonly used alternative, hCG, because gonadorelin works upstream to maintain the full HPG axis signal rather than simply mimicking LH directly at the testicular level. In post-anabolic steroid cycles where the entire HPG axis is suppressed, gonadorelin similarly represents a physiologically upstream restart mechanism compared to SERMs like clomiphene which work further downstream. However its very short half-life, the requirement for precise pulsatile dosing, and the practical challenge of achieving physiological pulse frequency outside medical infusion pump settings limit its practicality versus oral SERMs.
In clinical diagnostic settings a single 100 mcg IV or subcutaneous injection is used with serial blood sampling. For therapeutic hypogonadism treatment a portable pulsatile infusion pump delivers 5 to 20 mcg per pulse subcutaneously every 90 to 120 minutes. In TRT maintenance and PCT protocols used in wellness settings, subcutaneous injections of 100 mcg twice daily are most commonly cited — acknowledging this does not perfectly replicate physiological pulse frequency but achieves practical pulsatile exposure. It is supplied as a lyophilized powder reconstituted with saline or provided as a sterile solution.
Gonadorelin is generally well tolerated given its bioidentical nature. The most common side effects are local injection site reactions including redness, pain, and swelling, which occur in a meaningful proportion of users with repeated injections. Headache, nausea, lightheadedness, and abdominal discomfort have been reported. With repeated dosing, flushing and mild allergic reactions can occur. More serious but rare risks include anaphylaxis in hypersensitive individuals. Multiple pregnancies are a documented risk when gonadorelin is used for ovulation induction — twins, triplets, and higher-order multiples are possible and patients should be counseled accordingly. Paradoxical HPG axis suppression can occur if pulsatile dosing is not maintained — if doses are given too frequently or continuously, receptor desensitization will suppress rather than stimulate LH and FSH.
People with gonadotropin-releasing hormone adenoma — a rare pituitary tumor — should not use it as stimulation could cause serious pituitary complications including sudden blindness. Anyone with hormone-sensitive tumors — including estrogen-dependent tumors, androgen-dependent prostate cancer, or breast cancer — should not use it as the resulting hormone elevations could promote tumor growth. People with ovarian cysts should avoid it in fertility contexts. Those with known hypersensitivity to GnRH or its analogs should not use it. Infants are particularly sensitive and use is not recommended. Pregnant women should not use it after achieving pregnancy. Breastfeeding women should consult their physician as safety data is limited.





