
Triptorelin Acetate
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Triptorelin Acetate: When a Strong Signal Is Needed to Switch Everything Off
Triptorelin acetate is a synthetic analogue of GnRH, interesting primarily for its almost paradoxical logic: in a research and clinical context, it first produces a brief hormonal "surge", and then, with continuous exposure, leads to suppression of LH, FSH, and sex hormones.
It is precisely this controlled shift between phases that has made it an important tool in the study of hormone-dependent conditions and neuroendocrine regulation. In published data, the drug demonstrated the ability to bring testosterone levels to castration values in the majority of patients with advanced prostate cancer, and in the context of studying central precocious puberty — to suppress the pubertal hormonal signal in children.
For those with a research interest, this is one of those molecules where it is particularly clear how the same receptor pathway can first be activated, and then practically "go silent." No magic — just very illustrative endocrinology.
Triptorelin Acetate: A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Triptorelin is not a performance enhancer or a research chemical — it is an established, widely prescribed pharmaceutical that has been transforming endocrine medicine since 1986. It is the treatment backbone for approximately 70% of advanced prostate cancer patients globally. It arrests premature puberty in children, manages endometriosis pain, reduces uterine fibroids before surgery, controls ovulation timing in IVF, and in Europe is used in gender-affirming puberty suppression. It appears on the WHO Model List of Essential Medicines.
The story begins with Andrew Schally, the Polish-American endocrinologist who dissected 250,000 pig hypothalami to isolate 5 mg of GnRH, determined its sequence in 1971, and shared the Nobel Prize in Physiology or Medicine in 1977. Triptorelin was the first GnRH agonist analogue Schally synthesised, in 1973 — a single D-tryptophan substitution at position 6 that created the entire modern class of GnRH agonist pharmaceuticals.
The mechanism is one of the most counterintuitive in pharmacology: an agonist that causes hormone suppression through receptor desensitisation. Given pulsatilely (as GnRH naturally is), it stimulates gonadotropin release. Given continuously (as depot formulations deliver), the same receptor is overwhelmed, desensitises, and stops responding. Within 4 weeks of the first depot injection, testosterone or oestrogen falls to castration/post-menopausal levels and is maintained indefinitely.[4]
| At a glance | |
|---|---|
| INN / Generic name | Triptorelin |
| Brand names | Trelstar (US, prostate cancer); Triptodur (US, CPP); Decapeptyl (Europe); Diphereline (Ferring); Salvacyl (UK/Germany) |
| Type | Synthetic decapeptide GnRH superagonist |
| Sequence | pGlu-His-Trp-Ser-Tyr-D-Trp-Leu-Arg-Pro-Gly-NH&sub2; |
| Key modification | D-Trp at position 6 (vs. L-Gly in native GnRH) |
| Developer | Andrew Schally (Tulane University, 1973); licensed to Debiopharm 1982; marketed by Ipsen (Decapeptyl) and others |
| First approval | 1986 (France, Decapeptyl) |
| FDA approval | ✅ 2000 (Trelstar, prostate cancer); ✅ 2017 (Triptodur, CPP) |
| WHO status | ✅ Essential Medicine (therapeutic alternative) |
The Nobel Prize Context: Schally and GnRH
For most of the mid-20th century, the molecular nature of hypothalamic signals controlling the pituitary was unknown. Andrew Schally and his researchers dissected 250,000 pig hypothalami in order to isolate 5 mg of the hormone thyrotropin-releasing hormone (TRH). Together with Roger Guillemin he described gonadotropin-releasing hormone (GnRH), which controls FSH and LH secretion. The 1977 Nobel Prize in Physiology or Medicine was shared between Schally, Guillemin, and Rosalyn Yalow for work that defined the molecular basis of the hypothalamic-pituitary axis.[1]
GnRH was discovered by Schally in 1971 (Tulane University), and he performed the first synthesis of the GnRH agonist triptorelin in 1973. In 1981 he was the first to show that GnRH agonists inhibit growth of prostate cancer in rats, and together with Dr. George Tolis he organised the first clinical trial of GnRH agonists in patients with advanced prostate cancer in 1982 — demonstrating the clinical efficacy of LH-RH agonists in palliative treatment of androgen-dependent prostate cancer. Andrew Schally died on October 17, 2024, aged 97 — leaving a therapeutic legacy treating tens of millions of patients across prostate cancer, endometriosis, precocious puberty, and reproductive medicine.[2]
Structure: The D-Amino Acid Substitution
Native GnRH: pGlu-His-Trp-Ser-Tyr-Gly-Leu-Arg-Pro-Gly-NH&sub2;
Triptorelin: pGlu-His-Trp-Ser-Tyr-D-Trp-Leu-Arg-Pro-Gly-NH&sub2;
The single substitution of L-glycine at position 6 with D-tryptophan produces three consequences: the bulky D-tryptophan indole ring creates steric hindrance at the primary endopeptidase cleavage site (Tyr-Gly, positions 5-6), dramatically increasing plasma stability; the D-amino acid enforces a rigid β-turn conformation that the GnRH receptor prefers, increasing binding affinity; and the combined effect produces a GnRH agonist approximately 100-fold more potent than native GnRH for LH release. Other GnRH agonists use different position 6 substitutions (leuprolide D-Leu6; goserelin D-Ser(But)6) — all produce the same clinical effect through the same mechanism.[4]
The paradox of the agonist
Native GnRH is secreted in pulses every 60–90 minutes from the hypothalamus. The pituitary GnRH receptor requires a recovery interval between pulses to re-sensitise and respond to the next pulse. Continuous GnRH receptor stimulation — which is what a depot injection delivers — overwhelms this system: receptors are occupied continuously, receptor internalisation is triggered by persistent agonist binding, GnRH receptors are downregulated at the cell surface, pituitary gonadotrophs become refractory to GnRH signalling, and LH/FSH secretion collapses, with downstream sex hormone production falling to castrate/post-menopausal levels. The pharmacological hallmark of triptorelin is its biphasic HPG axis effect: a transient surge in LH, FSH, and sex hormones during the first 1–2 weeks, followed by profound suppression to castrate levels after ~4 weeks of continuous receptor stimulation, maintained indefinitely with continued dosing.
Depot Formulations: PLGA Microspheres
Triptorelin as a freely injected peptide has a plasma half-life of ~5 hours, requiring daily injections for pituitary suppression. The key pharmaceutical innovation enabling clinical use is depot injection technology. Triptorelin was incorporated into microgranules of the biocompatible and biodegradable copolymer poly(lactide-co-glycolide) (PLGA). By varying the PLGA polymer ratio (lactic acid:glycolic acid), the degradation rate and release duration can be controlled, producing 1-, 3-, 6-, and now 12-month sustained-release formulations from a single IM injection. Debiopharm is currently conducting Phase 3 trials (LIBELULA, enrollment complete November 2025) for a 12-month triptorelin formulation.[10]
The Testosterone Flare: Clinical Importance
⚠️ The initial stimulatory phase — the “testosterone flare” in the first 1–2 weeks after first injection — is clinically important and requires management in prostate cancer patients. The testosterone surge transiently worsens disease, with clinical consequences including spinal cord compression, urinary obstruction, and bone pain worsening. Patients at high risk (spinal metastases, obstructive urinary disease) require anti-androgen pre-treatment (bicalutamide 50 mg/day starting 1–2 weeks before the first triptorelin injection and continuing 2–4 weeks after) to block the testosterone surge’s effects. In prostate cancer patients with high-volume spinal metastases, the flare can cause acute spinal cord compression and paralysis — a medical emergency. GnRH antagonists (degarelix, relugolix) avoid the flare entirely and are now preferred in high-flare-risk patients.
FDA-Approved Indications (US)
Advanced prostate cancer (Trelstar — FDA 2000)
Medical castration via testosterone suppression to <50 ng/dL within 4 weeks; maintained indefinitely with continued dosing. Dosing: 3.75 mg IM every 4 weeks; 11.25 mg IM every 12 weeks; 22.5 mg IM every 24 weeks. Multiple Phase 3 RCTs have demonstrated equivalent testosterone suppression and clinical outcomes to surgical castration and other GnRH agonists. The landmark CHAARTED and STAMPEDE trials established that combining ADT (like triptorelin) with docetaxel or novel hormonal agents (abiraterone, enzalutamide) significantly improves overall survival in metastatic hormone-sensitive prostate cancer — for high-volume mHSPC, ADT+docetaxel improved median OS from 44.0 to 57.6 months. Triptorelin is clinically equivalent to other GnRH agonists for testosterone suppression; choice between agents is primarily driven by depot duration preference, formulation availability, and cost.[6][7]
Central precocious puberty (Triptodur — FDA 2017)
Central precocious puberty (CPP) is defined as puberty onset before age 8 in girls and 9 in boys, caused by premature activation of the hypothalamic GnRH pulse generator. Consequences include accelerated bone maturation and premature epiphyseal fusion, paradoxically resulting in shorter adult stature. Triptorelin suppresses premature GnRH axis activation, arresting pubertal development and protecting bone maturation timing. Dosing: 22.5 mg IM every 6 months for children ≥2 years. All patients achieve GnRH-stimulated LH peak levels below 3 mIU/mL between 6 and 24 months of treatment. Long-term follow-up confirms fertility is preserved after discontinuation.[8]
International Indications (Beyond US Approval)
Endometriosis (Europe, EMA-approved): Triptorelin suppresses oestradiol to post-menopausal levels, causing endometrial implant atrophy and pain relief. Dosing: 3.75 mg IM monthly × 3–6 months; add-back therapy (norethindrone 5 mg/day) is recommended beyond 3 months to mitigate bone density loss. Symptoms typically recur after treatment stops; treatment is used for symptom relief, pre-surgical fibroid/lesion size reduction, or as a bridge therapy.
Uterine fibroids (Europe): Pre-surgical triptorelin reduces fibroid volume by 25–50%, decreases operative blood loss, and may allow conversion from laparotomy to laparoscopy. Limited to 3–6 months due to bone density concerns.
IVF — long protocol and GnRH agonist trigger: In long protocol IVF, triptorelin suppresses endogenous LH surges, allowing the clinician to control follicular stimulation timing with exogenous gonadotrophins. A single-dose bolus of triptorelin (~0.1–0.2 mg SC) can also be used instead of hCG to trigger final oocyte maturation in GnRH antagonist IVF cycles — reducing ovarian hyperstimulation syndrome (OHSS) risk in high-responder patients.
Hormone-sensitive breast cancer: In premenopausal women with hormone receptor-positive breast cancer, triptorelin achieves ovarian suppression as an adjunct to endocrine therapy. GnRH agonist class evidence (SOFT and TEXT trials) shows adding ovarian function suppression improves disease-free survival in premenopausal high-risk patients.
Gender-affirming puberty suppression: Triptorelin is the primary GnRH agonist used for pubertal suppression in youth with gender dysphoria in many European countries. GnRHa treatment caused suppression of gonadotropins and sex steroids within 3 months in clinical cohorts; treatment did not have to be adjusted because of insufficient suppression in any subject. This use has become politically contested in some jurisdictions; evidence for psychological benefit exists from European cohort studies while long-term data on bone density, fertility, and neurodevelopment is still accumulating.[9]
Sexual deviation / male hypersexuality (Salvacyl — UK, Germany): Approved for the treatment of sexual deviations and male hypersexuality, including in convicted sex offenders as “chemical castration” — a controversial application with distinct ethical dimensions related to consent.
Approved Formulations
| Formulation | Dose | Interval | Indication |
|---|---|---|---|
| Trelstar (US) | 3.75 mg IM | Every 4 weeks | Prostate cancer |
| Trelstar (US) | 11.25 mg IM | Every 12 weeks | Prostate cancer |
| Trelstar / Triptodur (US) | 22.5 mg IM | Every 24 weeks | Prostate cancer; CPP ≥2 years |
| Decapeptyl (Europe) | 3.75 mg IM | Monthly | Prostate cancer; endometriosis; fibroids; CPP |
| Decapeptyl (Europe) | 11.25 mg IM | Every 3 months | Prostate cancer; CPP |
| Debio 4326 (Phase 3) | TBD | Every 12 months | CPP (LIBELULA trial, enrollment complete Nov 2025) |
The Community Off-Label Use: “Testosterone Restart”
⚠️ Triptorelin appears in the anabolic steroid community as a claimed single-dose treatment to “restart” testosterone production following suppressive steroid cycles. This is pharmacologically incorrect and dangerous.
Triptorelin does not “reset” pituitary receptors. A single dose causes a testosterone surge (flare) followed by weeks of testosterone suppression — worsening the hypogonadism it is supposed to treat. No published controlled trial or case series has validated triptorelin for post-cycle testosterone recovery. An inappropriate testosterone surge from the flare effect could cause cardiovascular events in individuals with underlying risk factors. The subsequent suppression is unpredictable and not rapidly reversible once a depot injection has been administered.
Standard post-cycle therapy uses selective oestrogen receptor modulators (SERMs — clomiphene, tamoxifen) and/or hCG with a documented evidence base, prescribed under physician supervision. This off-label use should be clearly distinguished from triptorelin’s legitimate medical applications.
Safety Profile
All adverse effects reflect profound sex hormone suppression — they are pharmacological, predictable, and often manageable. In men (prostate cancer treatment): hot flushes (>50% of patients); loss of libido, erectile dysfunction; fatigue and mood changes including depression; muscle loss and increased fat mass; and osteoporosis (~2–3% bone mineral density decrease per year, requiring DEXA monitoring, calcium/vitamin D supplementation, and bisphosphonates for high fracture risk patients.
⚠️ Cardiovascular risk of ADT: Contemporary evidence confirms that GnRH agonist ADT increases cardiovascular risk including MI, stroke, sudden cardiac death, and diabetes. GnRH antagonists (relugolix, degarelix) appear to carry lower cardiovascular risk in patients with established cardiovascular disease, shifting prescribing patterns in this subgroup.
In women (endometriosis, fibroids): menopausal symptoms (hot flushes, vaginal dryness, mood disturbance) and bone density loss, limiting treatment to 3–6 months without add-back therapy. In children (CPP): injection site reactions; initial pubertal flare (1–2 weeks post first dose); bone density temporarily lags during treatment but recovers after cessation; long-term data confirms recovery of normal pubertal development and fertility. Contraindications: pregnancy (known foetal harm; can induce abortion or foetal malformation); women planning pregnancy during treatment; hypersensitivity to GnRH or GnRH agonists.
Comparison with GnRH Antagonists
| Feature | Triptorelin (agonist) | Degarelix / Relugolix (antagonists) |
|---|---|---|
| Mechanism | Agonist → desensitisation | Direct receptor blockade |
| Testosterone flare | ⚠️ Yes (weeks 1–2) | ✅ No |
| Speed to castrate | ~4 weeks | ~3 days |
| Cardiovascular risk | Higher (GnRH agonist class) | Lower in patients with established CVD |
| Formulation | Depot IM (1/3/6 months); generic available | IM (degarelix); oral daily (relugolix) |
| Cost | Lower | Higher |
Common Misconceptions
“Triptorelin raises testosterone.”
Initially, yes — the flare effect causes a testosterone surge in the first 1–2 weeks. After that, testosterone is suppressed to castrate levels (<50 ng/dL). The compound’s clinical purpose is testosterone suppression, not elevation. The community off-label use for testosterone “restart” misunderstands this pharmacology entirely.
“A single low dose is safe for experimental use.”
⚠️ Even a single dose can produce a testosterone surge (flare) followed by weeks of hypogonadism. In patients with undiagnosed cardiovascular risk, the flare can precipitate cardiac events. The pharmacokinetics of a depot injection are not rapidly reversible. There is no dose that can be considered safe for off-label experimental use outside medical supervision.
“Triptorelin is the same as testosterone or anabolic steroids.”
Triptorelin is a GnRH agonist whose purpose is to suppress gonadal sex hormone production by exhausting pituitary receptor responsiveness. It has the opposite clinical effect to testosterone supplementation.
Key Takeaways
- ✅ Triptorelin is a Nobel Prize-connected pharmaceutical that has transformed multiple clinical specialties. Derived from Schally’s 1973 synthesis work (Nobel Prize shared 1977), it has been used clinically since 1986, is on the WHO List of Essential Medicines, and has treated tens of millions of patients globally.[1][2]
- The mechanism is a pharmacological masterpiece. An agonist that causes inhibition — exploiting the distinction between pulsatile physiological GnRH signalling and continuous pharmacological receptor stimulation. This principle is now used in at least six approved GnRH agonist drugs.
- ✅ Triptorelin has the broadest approved indication set of any GnRH agonist: prostate cancer, CPP, endometriosis, uterine fibroids, IVF, hormone-sensitive breast cancer, sexual deviations, and gender-affirming puberty suppression.
- ⚠️ The testosterone flare is clinically important and potentially dangerous. In prostate cancer patients with spinal metastases, the initial testosterone surge can cause acute spinal cord compression and paralysis. Anti-androgen co-treatment for the first injection is mandatory in high-risk patients.
- ⚠️ Off-label community use as a “testosterone restart” agent is not supported by evidence and is pharmacologically dangerous. This use misunderstands triptorelin’s mechanism and risks inducing prolonged testosterone suppression rather than restoration.
References
Discovery and History
- Schally AV, Arimura A, Kastin AJ, et al. Gonadotropin-releasing hormone: one polypeptide regulates secretion of luteinizing and follicle-stimulating hormones. Science. 1971;173(3997):1036–1038. (The GnRH discovery paper)
- Schally AV. Nobel Biographical: from lab to bedside: emerging clinical applications of GnRH agonists. Nobelprize.org. 1977; updated biographical essay.
- Debiopharm. Decapeptyl product history: first triptorelin synthesis 1973; first sustained-release GnRH agonist formulation in the world. Corporate history, 2024.
Structure and Pharmacology
- Engel JB, Schally AV. Drug insight: clinical use of agonists and antagonists of luteinizing-hormone-releasing hormone. Nature Clinical Practice Endocrinology & Metabolism. 2007;3(4):291–300.
Clinical Evidence — Prostate Cancer
- Heyns CF, Simonin MP, Grosgurin P, Schall R, Porchet HC. Comparative efficacy of triptorelin pamoate and leuprolide acetate in men with advanced prostate cancer. BJU International. 2003;92:226–231.
- CHAARTED trial: ADT combination therapy with docetaxel in metastatic hormone-sensitive prostate cancer. New England Journal of Medicine. 2015.
- STAMPEDE trial: multiple ADT combination therapy analyses in prostate cancer. Multiple NEJM and Lancet publications, 2015–2022.
Clinical Evidence — CPP
- Carel JC, Blumberg J, Seymour C, et al. Three-month sustained-release triptorelin (11.25 mg) in the treatment of central precocious puberty. European Journal of Endocrinology. 2006;154:119–124.
Clinical Evidence — Gender Dysphoria
- Schagen SE, Cohen-Kettenis PT, Delemarre-van de Waal HA, Hannema SE. Efficacy and safety of GnRHa treatment to suppress puberty in gender dysphoric adolescents. Journal of Sexual Medicine. 2016;13:1125–1132. PMID 27318023
Pharmacokinetics and PLGA Technology
- Effectiveness, pharmacokinetics, and safety of triptorelin acetate microspheres in patients with locally advanced and metastatic prostate cancer. PMC11672368. 2024.
Key Investigators
- Andrew V. Schally, PhD (1926–2024) — Tulane University; co-Nobel Laureate 1977; discoverer of GnRH; synthesiser of triptorelin (1973); pioneer of GnRH agonist clinical application in prostate cancer (1982). One of the most important endocrine pharmacologists of the 20th century.
- Fernand Labrie, MD, PhD — Laval University; major contributor to GnRH agonist development and the concept of maximal androgen blockade.
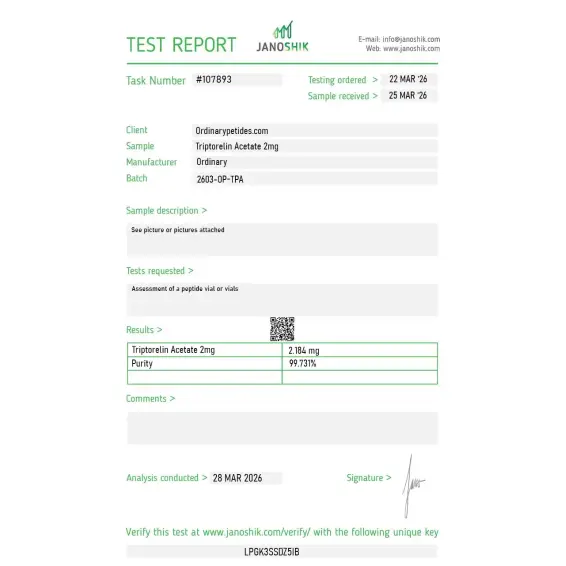
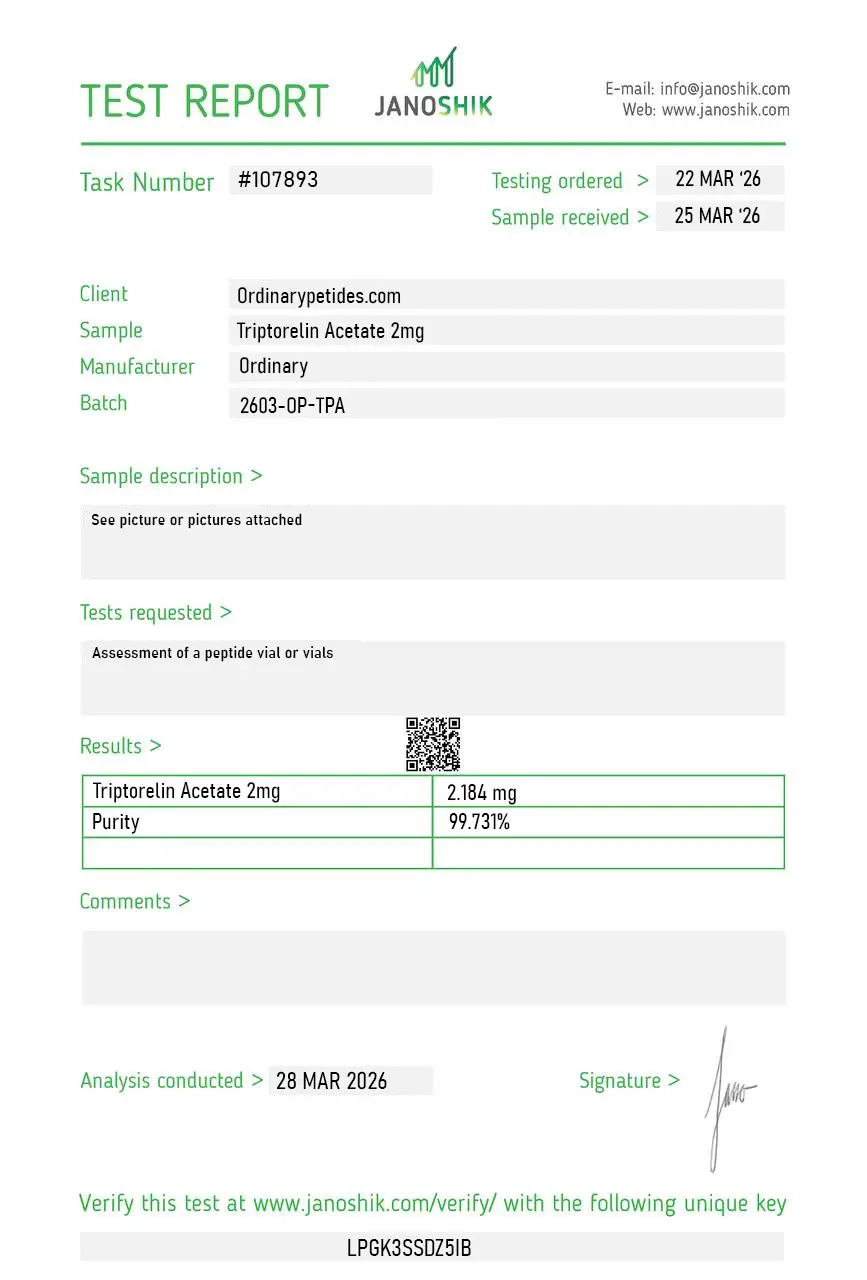
Certificate of Analysis
An independent test report is available for Triptorelin Acetate 2mg. This report provides batch-level documentation and analytical verification information for research reference.
Asked support whether their material is the acetate or pamoate salt — the acetate dissolves quickly in standard buffer while the pamoate (depot pharmaceutical form) has very different solubility behavior and isn't right for cell-culture work. They confirmed acetate within an hour. Saved me a potential expensive mistake on the wrong salt form.
Following the salt-form question I asked previously — would still suggest the listing explicitly state "acetate salt" prominently rather than burying it in technical details, since pamoate versions exist in the pharmaceutical depot formulations and the buying decision is more consequential than buyers may realize. Acetate is what arrived, which is what I wanted.





