

Melanotan 2 (MT2)
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Melanotan 2: Bold Signal, Complex Biology
Melanotan 2 is a synthetic cyclic analog of α-MSH that drew attention not because it does one simple thing, but because in early studies it showed a surprisingly broad activity profile. In published human observations, MT2 was associated with skin darkening, and in early clinical research it also showed erectogenic effects, while preclinical work linked it to appetite-related melanocortin pathways.
But this is exactly where the molecule gets interesting — and tricky: MT2 is not a narrow "tanning peptide," but a nonselective melanocortin agonist with effects that reach far beyond pigmentation. In the research context, that same broad activity came with a mixed tolerability picture, including nausea, yawning, reduced appetite, and other adverse effects.
So MT2 stands out less as a polished solution and more as a vivid, pharmacologically loud research compound that clearly does something — just not only what the label on the internet promises. For anyone exploring melanocortin biology, that makes MT2 hard to ignore and even harder to oversimplify.
Melanotan 2 (MT-2): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Melanotan 2 is the compound born from one of the more memorable accidents in peptide research history. In the early 1990s, a University of Arizona researcher testing a new cyclic α-MSH analogue on himself administered twice the intended dose and experienced an eight-hour erection alongside intense nausea and vomiting. The sexual effects were not a quirk — nine of the first ten male volunteers in formal trials experienced spontaneous erections. The compound was supposed to be a tanning agent. It turned out to be simultaneously a tanning agent, a pro-sexual compound, an appetite suppressant, and, depending on dose, a trigger of significant adverse effects.[1]
That accident ultimately bifurcated into two approved drugs: MT-1 (afamelanotide, Scenesse) went down the tanning pathway and achieved FDA approval for erythropoietic protoporphyria in 2019. The sexual effects pathway led to bremelanotide (PT-141, Vyleesi), which achieved FDA approval in 2019 for hypoactive sexual desire disorder. MT-2 itself was never submitted for FDA approval, never reached Phase 3 trials, and has been available as an unregulated research chemical for three decades.
The core problem with MT-2 is its receptor non-selectivity: it activates MC1R (tanning), MC3R (sexual motivation, appetite), MC4R (erections, appetite suppression, CNS), and MC5R simultaneously. Its cyclic structure makes it lipophilic enough to cross the blood-brain barrier. And its MC1R stimulation — the same pathway that produces the desirable tanning — is biologically linked to melanocyte proliferation and, through published case reports, to melanoma.
| At a glance | |
|---|---|
| Common names | Melanotan 2; MT-2; MT-II |
| Chemical name | Ac-Nle-cyclo[Asp-His-D-Phe-Arg-Trp-Lys]-NH&sub2; |
| Molecular weight | ~920.1 Da |
| Structure | Cyclic heptapeptide; lactam bridge between Asp and Lys side chains; C-terminal amide |
| Receptor targets | MC1R, MC3R, MC4R, MC5R (non-selective) |
| Crosses blood-brain barrier | Yes — sufficient lipophilicity from cyclic structure |
| FDA approval | ❌ None; no NDA ever submitted |
| WADA | ❌ Prohibited at all times (S4) |
| Descendant approved drugs | Bremelanotide/Vyleesi (Palatin, FDA-approved 2019, HSDD) |
| Key safety concern | ⚠️ Melanoma (5+ case reports; causation unproven; biologically plausible); rhabdomyolysis; priapism |
Discovery: The Accident That Redirected Melanocortin Pharmacology
In the 1980s, the University of Arizona laboratory of Victor Hruby set out to create a compound that could tan fair skin without UV exposure. The team synthesised multiple analogues of α-MSH, modifying the parent sequence to improve potency and stability. MT-2’s cyclic structure was created by forming a lactam bridge between the side chains of aspartic acid and lysine, constraining the peptide backbone into a conformation that dramatically increased receptor binding affinity and proteolytic stability. This constraint also had an unanticipated pharmacological consequence: by eliminating the receptor discrimination that the linear MT-1 structure partially maintained, the cyclic form activated multiple melanocortin receptor subtypes with near-equal potency.
Very early in the research process, Mac Hadley conducted a self-experiment and mistakenly injected himself with twice the intended dose, experiencing an eight-hour erection along with nausea and vomiting. During the first human trials of MT-2 in the early 1990s, nine of the first ten male subjects who received MT-2 by subcutaneous injection experienced spontaneous erections.[3] The sexual effects were mediated by MC4R receptors in the hypothalamus — a receptor subtype that MT-1’s linear structure does not sufficiently engage at therapeutic doses because the linear peptide does not meaningfully cross the blood-brain barrier.
The development bifurcation
The discovery immediately bifurcated MT-2’s development path. The tanning programme was licensed to Epitan/Clinuvel in Australia; regulatory agencies did not support a cosmetic indication for a systemically injected peptide, and the programme pivoted to EPP treatment using the MC1R-selective linear analogue (MT-1/afamelanotide, FDA-approved 2019). The sexual dysfunction programme was licensed to Palatin Technologies, who synthesised bremelanotide (PT-141), a likely metabolite of MT-2 differing only at the C-terminus (amide replaced by free acid) and with partially different receptor selectivity. Palatin ceased development of MT-2 in 2000 and developed bremelanotide independently. The parties settled intellectual property litigation in 2008, with Palatin retaining bremelanotide and returning rights to MT-2 to Competitive Technologies for $800,000. MT-2 itself was never submitted for approval and entered the unregulated research chemical market.[11]
Structure and Chemistry
MT-2’s full sequence: Ac-Nle-cyclo[Asp-His-D-Phe-Arg-Trp-Lys]-NH&sub2;. The “cyclo” notation indicates that aspartic acid and lysine side chains are linked by a covalent lactam bridge, forming a macrocyclic peptide ring. The cyclic constraint increases receptor binding affinity by pre-organising the peptide into the active conformation; improves proteolytic stability; increases lipophilicity sufficient for blood-brain barrier penetration; and eliminates the modest receptor selectivity that the linear MT-1 structure maintains. The N-terminus carries acetylated norleucine and the C-terminus carries an amide (–NH&sub2;) — the latter distinguishes MT-2 from bremelanotide, which has a free carboxylic acid (–OH) at the C-terminus, altering receptor binding kinetics and partially reducing MC1R activity relative to MC4R.
Mechanism of Action
Receptor profile: the non-selectivity problem
| Receptor | Primary location | MT-2 effect | Clinical manifestation |
|---|---|---|---|
| MC1R | Skin melanocytes, keratinocytes | Eumelanin synthesis via cAMP→tyrosinase | Skin darkening; mole darkening; ⚠️ melanoma risk |
| MC3R | Hypothalamus, peripheral tissues | Energy balance; sexual motivation | Appetite suppression; sexual drive |
| MC4R | Hypothalamus, brainstem, spinal cord | Appetite suppression; sexual arousal; erection | Spontaneous erections; appetite suppression; nausea |
| MC5R | Exocrine glands | Sebaceous/lacrimal secretion | Poorly characterised clinically |
Unlike MT-1, which has approximately 10-fold selectivity for MC1R over other receptors, MT-2 has no significant selectivity and crosses into the CNS freely. This means MT-2’s “tanning dose” simultaneously activates hypothalamic circuits governing appetite and sexual arousal. The system demonstrates significant complexity through promiscuous G-protein coupling: MC3R, MC4R, and MC5R can couple to Gi (inhibiting adenylyl cyclase) and Gq proteins, creating tissue-specific signalling patterns that explain MT-2’s diverse effects. This same complexity makes predicting dose-response relationships at the individual level unreliable.
The melanoma mechanism: why MC1R stimulation is a genuine concern
MC1R activates melanocytes through the cAMP/MITF pathway. MITF drives transcription not only of pigmentation enzymes but also of melanocyte proliferation and survival genes. At supraphysiological levels, sustained MC1R activation increases melanocyte mitotic activity — the same cells from which melanoma arises. The key difference from the MT-1 safety argument: afamelanotide is delivered as a controlled slow-release implant with plasma levels falling to undetectable by day 10 of a 60-day cycle. MT-2 as used in the community is injected repeatedly — daily or multiple times per week — producing repeated pulses of supraphysiological MC1R activation with no pharmacokinetic control. The exposure profile is categorically different even if the molecule is pharmacologically similar at the receptor.
Human Clinical Evidence
MT-2 has approximately 20 human studies in the published literature, of which perhaps 3–5 qualify as randomised controlled trials. All are small (N=10–30), short in duration, and were conducted as proof-of-concept rather than pivotal trials. No Phase 3 programme was ever initiated and no NDA was ever submitted.
Tanning efficacy: The original University of Arizona Phase 1 trials confirmed dose-dependent melanin increase across Fitzpatrick skin types, including in individuals who were previously unable to tan. The tanning pharmacological effect is not disputed.[1] Erectile dysfunction: A series of small RCTs from the University of Arizona/Palatin research collaboration tested MT-2 for erectile dysfunction and confirmed centrally mediated (hypothalamic MC4R) erections in men with psychogenic and organic ED, with spontaneous erections occurring without sexual stimulation in a majority of subjects, and dose-limiting nausea in a significant proportion.[3] Once Palatin pivoted to bremelanotide, MT-2 ED research was abandoned.
| Domain | Evidence type | Finding |
|---|---|---|
| Tanning | Phase 1 RCT | Significant dose-dependent melanin increase ✅ |
| Erectile dysfunction | Small RCTs (3–5 studies) | Improved erections; spontaneous erections; dose-limiting nausea ✅ |
| Appetite suppression | Observational; community reports; no RCT | Consistent with MC4R mechanism; not formally quantified |
| Melanoma | Case reports (5+ documented) | ⚠️ Causation not established; biologically plausible |
| Rhabdomyolysis | Case report (ICU admission) | ⚠️ Confirmed by mass spectrometry; dose 6× starting dose |
| Priapism | Case report | ⚠️ Overdose context; urological emergency |
Safety: The Case Report Literature
Acute adverse effects
The acute adverse effect profile of MT-2 is consistent and dose-related: nausea (peaks 30–90 minutes post-injection; centrally mediated via area postrema MC4R; tachyphylaxis develops with continued use); facial flushing; spontaneous erections in men at tanning doses — not an isolated effect but a routine pharmacological consequence; appetite suppression; yawning; fatigue. These effects are direct pharmacological consequences of a non-selective melanocortin agonist that crosses the blood-brain barrier and cannot be avoided by dose selection alone.
Serious documented adverse events
⚠️ Rhabdomyolysis and renal dysfunction (Nelson et al., 2012):[5] A 39-year-old male injected 6 mg of internet-purchased MT-2 — six times the recommended starting dose. In the emergency department, vital signs included BP 151/85 mmHg, HR 130 bpm. Physical examination demonstrated restlessness, anxiety, mydriasis, diaphoresis, tachycardia, and diffuse muscle tremors. Urinalysis demonstrated 3+ blood with red cell casts. Mass spectrometry confirmed the substance as MT-2. CPK peaked at 17,773 IU/L. The patient was admitted to the ICU and received intravenous fluids with sodium bicarbonate for rhabdomyolysis. The sympathomimetic excess in this case is consistent with supraphysiological central melanocortin activation overwhelming sympathetic regulation.
⚠️ Priapism (Devlin et al., 2013):[6] Overdose-associated priapism — a urological emergency requiring immediate intervention.
Melanoma case reports
⚠️ There have been at least five published reports of melanoma in MT-2 users. A 20-year-old woman with Fitzpatrick skin type II and a history of tanning bed use was diagnosed with melanoma on her left gluteal region three months after a three-week course of self-administered MT-2 treatment. In a separate report, a 23-year-old White woman with red hair and familial melanoma history had three melanoma lesions identified on the back, abdomen, and right arm following three years of self-administered MT-2 treatment; genetic testing revealed heterozygous MC1R and CDKN2A variants (a high-risk melanoma-associated gene).[7] A 2012 case documented melanoma in situ four weeks after initiation of MT-2 use from a regulated compounding pharmacy — explicitly excluding poor product quality as the explanation. A 2025 case report documented oral mucosal melanoma associated with chronic MT-2 nasal spray use.[9]
The melanoma causation question: where the evidence actually stands
All melanoma cases involved individuals with additional risk factors (fair skin, UV exposure, family history). The epidemiological challenge is severe: MT-2 is used primarily by fair-skinned individuals seeking to tan, who then use their new tan to justify more UV exposure — dramatically confounding risk attribution. A 2013 scientific review found no conclusive evidence of melanoma causation; a 2021 review concluded increased risk in MT-2 users probably reflects more UV exposure.
The mechanistic argument for genuine concern: MC1R activation increases melanocyte proliferation and survival signalling; sustained supraphysiological MC1R activation has no physiological precedent; the melanoma in situ case from a regulated compounding source occurred within four weeks before significant UV accumulation; multiple cases involve injection-site lesions; CDKN2A heterozygosity in one case suggests genetic susceptibility interacting with MC1R stimulation. The responsible summary: causation is not proven; confounding by UV is a legitimate alternative explanation for most cases; the biological mechanism is plausible; the cases are real; and no safe dose threshold exists.[10]
Regulatory and Legal Status
| Jurisdiction | Status |
|---|---|
| USA (FDA) | ❌ Not approved; no NDA ever submitted; FDA warning letters issued to companies selling for human use |
| Europe (EMA) | ❌ Not approved |
| Australia / New Zealand | Controlled substance; requires prescription; enforcement activity ongoing |
| UK (MHRA) | Unlicensed medicine; illegal to sell for human use; MHRA enforcement actions |
| WADA | ❌ Prohibited at all times — S4 (Hormone and Metabolic Modulators) |
MT-2 vs. Its Approved Derivatives
| Feature | MT-2 | Afamelanotide (Scenesse, MT-1) | Bremelanotide (Vyleesi, PT-141) |
|---|---|---|---|
| Structure | Cyclic heptapeptide | Linear tridecapeptide | Cyclic heptapeptide (MT-2 metabolite) |
| C-terminus | –NH&sub2; (amide) | –NH&sub2; (amide) | –OH (free acid) |
| Receptor profile | MC1R, MC3R, MC4R, MC5R | MC1R selective | MC3R, MC4R selective |
| Crosses BBB | Yes | No (therapeutic doses) | Yes |
| Tanning | Yes (strong) | Yes (primary effect) | Mild (side effect) |
| Erection/sexual arousal | Yes (prominent) | ❌ No | Yes (primary effect) |
| FDA approved | ❌ No | ✅ Yes (EPP, 2019) | ✅ Yes (HSDD, 2019) |
| Phase 3 trials | ❌ No | ✅ Yes (NEJM 2015) | ✅ Yes |
| Melanoma signal | ⚠️ 5+ case reports; unresolved | ✅ Not detected (8-year observational) | Not characterised |
Common Misconceptions
“MT-2 is basically the same as MT-1 — just a different number.”
They are structurally distinct — linear vs. cyclic, tridecapeptide vs. heptapeptide — and pharmacologically opposite in receptor selectivity. MT-1 does not meaningfully cross the blood-brain barrier at clinical doses; MT-2 does. MT-1 lacks MC4R-mediated CNS effects; MT-2’s MC4R activation is its defining feature. This is not a numbering difference; it is a different compound with a different safety and efficacy profile.
“The melanoma risk is just theoretical.”
⚠️ Five or more published case reports have described melanoma in MT-2 users. These are documented patients with melanoma who had been using MT-2. Causation is not proven and UV confounding is a legitimate alternative explanation, but “theoretical” misrepresents the medical literature. It is an unresolved concern with actual cases.
“MT-2 is safe because MC1R activation didn’t cause melanoma in the Scenesse trials.”
The Scenesse exposure profile (controlled slow-release implant, undetectable plasma levels by day 10 of a 60-day cycle) is categorically different from community MT-2 use (daily injections sustaining continuous supraphysiological MC1R stimulation). The same molecule at different exposure profiles is not the same pharmacological situation.
“Bremelanotide is just an approved version of MT-2.”
Bremelanotide is structurally derived from MT-2 (a single C-terminus modification) but has a different receptor selectivity profile emphasising MC3R/MC4R over MC1R, underwent a full Phase 3 clinical development programme, and received FDA approval for a specific indication. The structural similarity is real; the clinical and regulatory equivalence is not.[11]
Frequently Asked Questions
Is there any way to use MT-2 that avoids the melanoma concern?
No safe dose threshold has been established. The melanoma mechanism is a property of the peptide’s primary pharmacology, not a dose-dependent off-target effect. Individuals with personal or family history of melanoma, dysplastic nevi, fair skin (Fitzpatrick I–II), or MC1R polymorphisms are at particularly elevated theoretical risk.
Why did nine of the first ten male volunteers get erections?
MC4R receptors in the paraventricular nucleus of the hypothalamus coordinate erectile function through a central nervous system pathway. MT-2, by crossing the blood-brain barrier and activating these receptors, produces erections through a mechanism entirely separate from peripheral vascular biology — which is why PDE5 inhibitors (which work peripherally) and MT-2 (which works centrally) are additive and potentially interact to produce dangerous hypotension.[3]
If bremelanotide is approved for sexual dysfunction, can I use MT-2 for the same purpose?
No. Bremelanotide (Vyleesi) is FDA-approved, manufactured to pharmaceutical standards, has Phase 3 trial safety data, and is prescribed by physicians for a defined indication with monitoring for adverse effects. MT-2 from the research chemical market adds the melanoma signal that bremelanotide’s development programme was partly designed to avoid, and is not a substitute.[12]
Key Takeaways
- MT-2 is a non-selective melanocortin agonist that simultaneously activates MC1R, MC3R, MC4R, and MC5R. Its cyclic structure enables BBB penetration. The non-selectivity is not a side-effect problem — it is the fundamental pharmacological character of the compound.
- The discovery of its sexual effects in 1990s clinical testing was accidental — a self-experiment involving twice the intended dose. Nine of ten male volunteers experienced spontaneous erections. That accident was pharmacologically real and reproducible and ultimately produced bremelanotide (Vyleesi), an FDA-approved drug for HSDD.[3]
- MT-2 was never submitted for regulatory approval and both pharmacological effects it produces — tanning and sexual function — were separately developed into approved drugs (Scenesse and Vyleesi respectively). MT-2 itself sits in the unregulated research chemical market, where it has remained for 30 years.
- ⚠️ The melanoma signal is documented, not theoretical. At least five published case reports describe melanoma in MT-2 users. Causation is not proven; UV confounding is a legitimate alternative explanation. None of this makes the signal “theoretical.” No safe dose threshold exists.[7]
- ⚠️ Community MT-2 dosing produces a fundamentally different pharmacological exposure than the controlled clinical trials that informed the Scenesse safety data. Repeated daily injections sustaining continuous supraphysiological MC1R stimulation are not equivalent to Scenesse’s intermittent, decaying implant profile. Extrapolating Scenesse’s safety record to community MT-2 use is pharmacologically incorrect.
- ⚠️ The “Barbie drug” media framing trivialises a compound whose known serious adverse events include ICU-admission rhabdomyolysis, priapism, documented melanoma cases, and the uncontrolled variable of unregulated product quality in the supply chain.[5]
References
Structural and Discovery
- Dorr RT, Lines R, Levine N, et al. Evaluation of Melanotan-II, a superpotent cyclic melanotropic peptide in a pilot phase-I clinical study. Life Sciences. 1996;58(20):1777–1784.
- Hadley ME, Dorr RT. Melanocortin peptide therapeutics: historical milestones, clinical studies and commercialization. Peptides. 2006;27(4):921–930.
Clinical ED and Sexual Function
- Wessells H, Levine N, Hadley ME, et al. Melanocortin receptor agonists, penile erection, and sexual motivation: human studies with melanotan II. International Journal of Impotence Research. 2000;12(Suppl 4):S74–S79.
- Diamond LE, Earle DC, Heiman JR, et al. An effect on the subjective sexual response in premenopausal women with sexual arousal disorder by bremelanotide (PT-141). Journal of Sexual Medicine. 2006;3(4):628–638.
Safety — Serious Adverse Events
- Nelson ME, Bryant SM, Aks SE. Melanotan II injection resulting in systemic toxicity and rhabdomyolysis. Clinical Toxicology (Philadelphia). 2012;50(10):1169–1173. PMID: 23121206
- Devlin J, Pomerleau A, Foote J. Melanotan II overdose associated with priapism. Clinical Toxicology (Philadelphia). 2013;51(4):383. PMID: 23537392
Melanoma Case Reports
- Brennan R, Wells JSG, Van Hout MC. Melanoma and melanotan II — a review. Journal of Substance Use. 2014. PMID: 24355990
- Melanoma associated with the use of melanotan-II (melanoma in situ, regulated compounding source). ResearchGate. 2013.
- Oral mucosal melanoma case associated with MT-2 nasal spray. Case report. 2025.
Review
- Böhm M, et al. An overview of benefits and risks of chronic melanocortin-1 receptor activation. Journal of the European Academy of Dermatology and Venereology. 2025;39:39–51. PMC11664455
Bremelanotide Development
- Bremelanotide. Wikipedia. en.wikipedia.org/wiki/Bremelanotide
- FDA approval of bremelanotide (Vyleesi) for HSDD. June 2019. fda.gov
Certificate of Analysis
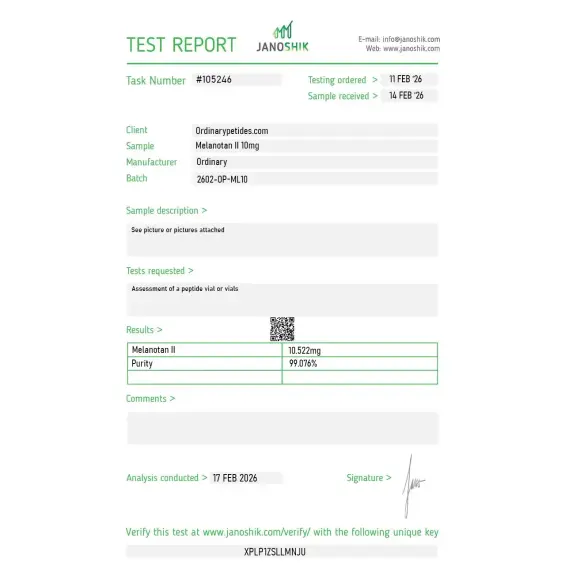
An independent test report is available for Melanotan II 10mg. This report provides batch-level documentation and analytical verification information for research reference.

Based on 1 reviews
5.0
The Asp-5-to-Lys-10 lactam bridge is what gives MT-II its locked active conformation and is worth understanding mechanistically when ordering — the cyclization through side chains rather than termini is a specific design choice that constrains the peptide into a β-turn mimicking α-MSH's bound conformation. For studying side-chain-cyclization as a peptide-engineering strategy across cyclic-peptide research, MT-II is a clean worked example of the approach. The material delivered the expected locked-conformation receptor activation in our binding assays.
Melanotan 2 (MT-II) is a synthetic cyclic heptapeptide analog of alpha-melanocyte stimulating hormone (α-MSH), developed at the University of Arizona in the 1980s as a successor to Melanotan 1 (afamelanotide). Where MT-1 is a linear 13-amino acid peptide, MT-2 is a shorter cyclic 7-amino acid structure — a lactam bridge connects the epsilon-amino group of lysine to the gamma-carboxy group of aspartic acid, creating a ring that makes it more metabolically stable and potent than its linear predecessor. Unlike MT-1 / afamelanotide which was developed into an approved pharmaceutical drug (Scenesse) for erythropoietic protoporphyria, MT-2's pharmaceutical development was abandoned in the early 2000s and it has never received approval from the FDA, EMA, TGA, or any other major regulatory authority. It is not approved for any indication, is not legally available without a prescription in most jurisdictions, and carries a significantly more complex and concerning safety profile than MT-1.
Melanotan II mimics α‑MSH and binds to melanocortin receptors (such as MC‑1R), which play roles in melanin (pigment) production in the skin. This interaction stimulates melanogenesis, which can make the skin appear darker.
Scientific literature and public health sources describe several effects associated with Melanotan II: increased skin pigmentation (tanning), changes in appetite, and stimulation of melanocortin receptors that can influence sexual function.
No. Melanotan II is not approved for medical or cosmetic use in many jurisdictions, and health agencies warn that it is unlicensed and largely untested for safety, quality, or effectiveness.
In laboratory settings, Melanotan II is typically supplied as a lyophilized (freeze‑dried) peptide powder intended for research applications such as receptor studies. It is not supplied as an approved drug formulation.
Research suppliers commonly recommend storing lyophilized Melanotan II desiccated and cold (e.g., −20 °C or colder) and protecting it from light and moisture to maintain integrity. Reconstituted solutions are usually kept refrigerated and used within a limited time.
Health agencies and research sources report potential side effects including nausea, flushing, reduced appetite, changes in mole pigmentation, and spontaneous erections in males. There are also concerns about irregular pigmentation changes and potential cancer risks, especially with unregulated use.
No. Major health authorities warn that Melanotan II products are often unregulated, untested, and potentially unsafe, and they advise against their use outside controlled research or clinical contexts.
This is the single most important distinction between the two compounds. MT-1 (afamelanotide) binds selectively and primarily to MC1R — the peripheral melanocortin receptor on skin melanocytes that drives pigmentation. MT-2 is a non-selective agonist that binds all five melanocortin receptors — MC1R, MC3R, MC4R, and MC5R — with significant potency at each. This non-selectivity is the source of both MT-2's additional effects and its greater risk profile. MC4R activation in the brain drives sexual arousal and appetite suppression. MC3R activation influences energy balance and metabolism. MC5R activation affects exocrine gland function. Because MT-2 crosses the blood-brain barrier — unlike MT-1 which does not readily do so — its central MC4R and MC3R effects are pronounced and reliable, producing an array of systemic effects that MT-1 does not.
MT-2's effects fall into several categories driven by its multi-receptor activity. Through MC1R activation it produces eumelanin synthesis and skin darkening — deeper and faster than natural UV-induced tanning — but typically requires some UV exposure to reach its maximum tanning effect. Through MC4R activation in the hypothalamus it reliably produces sexual arousal, spontaneous erections in men, and increased libido in both sexes — effects that were accidentally discovered when a researcher self-administered double the intended dose during tanning experiments. Published double-blind, placebo-controlled clinical trials in men with both psychogenic and organic erectile dysfunction showed that 8 to 9 of 10 subjects developed erections after MT-2 administration at 0.025 mg/kg, with mean erection duration of 38 to 64 minutes. Through MC4R and MC3R activation it also produces appetite suppression, yawning, stretching, and fatigue — effects users sometimes describe as a desirable side effect package but which represent pharmacological indicators of widespread central melanocortin system activation.
Palatin Technologies licensed MT-2 from the University of Arizona for development as an erectile dysfunction drug. During development Palatin identified bremelanotide — now FDA-approved as Vyleesi for hypoactive sexual desire disorder in women — as a likely metabolite of MT-2 with a more favorable safety profile. Palatin abandoned MT-2 and focused on bremelanotide instead. Clinuvel abandoned its cosmetic tanning development of MT-2 due to regulatory restrictions. The result is that MT-2 itself has no active pharmaceutical sponsor and no regulatory approval pathway, while its pharmacologically related descendant bremelanotide is now an approved drug.
The side effect profile is substantially broader and more concerning than MT-1. Nausea, vomiting, and stomach cramps are the most consistently reported effects — occurring in a majority of users particularly at initiation and at higher doses. Facial flushing, fatigue, yawning, and spontaneous stretching are characteristic and frequent. Appetite suppression can be significant. In men spontaneous erections unrelated to sexual stimulus occur reliably. Darkening of existing moles and freckles is universal. New mole formation and changes in mole morphology — including dysplastic changes — have been documented in multiple case reports. Melanoma has been reported in several individuals following MT-2 use — a 42-year-old woman developed melanoma on an abdominal nevus three months after one week of self-administered MT-2, and a 66-year-old man developed melanoma-in-situ after four weeks of use. While the causal relationship remains debated — and both had significant UV exposure histories — the association is a serious clinical concern. Blood pressure elevation has been reported. The risks from unregulated product impurities, contamination, and shared needle use add substantial additional infection risk.
MT-2 has no approved therapeutic indication anywhere in the world. Regulatory agencies including the FDA, EMA, TGA, and MHRA have all issued warnings against its use. It is illegal to sell without a prescription in the UK, EU, Australia, and most other jurisdictions. In the United States it exists in a grey zone — not scheduled as a controlled substance but not approved or legally compoundable. The TGA in Australia has seized large quantities of illegally imported MT-2. Products marketed online as "Melanotan 2," "MT-2," or the "Barbie drug" are completely unregulated, manufactured without quality control, and pose risks from unknown impurities, incorrect dosing, and contamination in addition to the pharmacological risks of the compound itself.
Anyone with a personal or family history of melanoma or atypical nevi should absolutely not use it — the mole change and melanoma case reports make this a firm contraindication. People with fair skin are at highest risk given the combination of increased UV sensitivity and the documented nevi changes. Anyone using tanning beds while taking MT-2 faces compounded melanoma risk. People with cardiovascular conditions should be aware of blood pressure effects. Women should not use it during pregnancy or breastfeeding. The honest clinical assessment is that unlike MT-1 / afamelanotide — which has a genuine approved medical purpose and a pharmaceutical-grade safety record — MT-2 has no approved indication, no legitimate pharmaceutical-grade product available to consumers, a documented association with melanoma in case reports, and no regulatory pathway to approval. Its descendant bremelanotide (Vyleesi) is the appropriate FDA-approved option for those seeking a melanocortin-based treatment for sexual dysfunction.





