



Oxytocin Acetate
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Oxytocin Acetate: Familiar Molecule, Far Less Simple Than the Hype
Oxytocin acetate is not some brand-new "social peptide," but a salt form of oxytocin — the classic cyclic nonapeptide hormone with a long-established role in uterine contractions and the milk let-down reflex. In the research context, oxytocin also drew attention as a neuromodulator linked to social behavior, stress, emotions, eating behavior, and other CNS-related processes, which is exactly why it became so heavily marketed outside medicine.
But the published data here are much less tidy than the "love hormone" label suggests: outside obstetrics, results in psychiatry, social function, anxiety, autism, and obesity remain mixed, context-dependent, and often contradictory. Even intranasal studies, which sound sleek on paper, are complicated by low and highly variable systemic bioavailability, helping explain why the literature looks less like a breakthrough and more like a puzzle.
So what makes oxytocin acetate interesting is not a fantasy of instant trust or charisma, but the fact that it sits at the crossroads of proven hormonal biology and much murkier behavioral research. For a client who values real science over romance-heavy marketing, that tension is exactly what makes it worth a closer look.
Oxytocin Acetate: A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Oxytocin occupies a singular place in the history of peptide science. It was the first peptide hormone to have its sequence determined, the first to be synthesised, and its synthesis earned a Nobel Prize in Chemistry in 1955. It is FDA-approved and used clinically in every obstetric unit in the world. And it is simultaneously at the centre of one of the most contested research programmes in modern psychiatry — a 25-year effort to harness its prosocial properties for the treatment of autism, social anxiety, PTSD, and other disorders of social function.
Single-dose experiments in healthy volunteers consistently show that intranasal oxytocin increases trust, improves emotion recognition, enhances attention to social stimuli, and reduces amygdala reactivity to threatening faces. These effects are real and well-replicated. Translating them into chronic treatment benefits for clinical populations has proved far harder — the pivotal US autism trial (SOARS-B, 272 participants, 24 weeks) was negative on its primary endpoint, and multiple other trials have produced inconsistent results.[11]
⚠️ The “cuddle hormone” popularisation has also constructed a simplistic narrative around a molecule whose effects include driving ethnocentrism, in-group favouritism, and defensive aggression toward out-groups. Oxytocin is better understood as a social salience enhancer than a simply prosocial molecule.
| At a glance | |
|---|---|
| Sequence | Cys-Tyr-Ile-Gln-Asn-Cys-Pro-Leu-Gly-NH&sub2; (cyclic; disulfide bond Cys1–Cys6) |
| Molecular weight | ~1,007 Da |
| Type | Nonapeptide; endogenous neuropeptide and peripheral hormone |
| Discovery | 1906 (uterotonic effects, Henry Dale) |
| First synthesis | 1953–1954 (du Vigneaud) — first polypeptide hormone synthesised |
| Nobel Prize | 1955 — du Vigneaud, Chemistry |
| FDA-approved uses | ✅ Pitocin/Syntocinon: labour induction, labour augmentation, postpartum haemorrhage control |
| Psychiatric/neurological uses | ⚠️ All investigational; not FDA-approved |
| Plasma half-life | 1–5 minutes |
| Receptor | OXTR — Gq-coupled GPCR; single receptor type |
| Popular names | “Love hormone”, “bonding hormone”, “cuddle hormone” — all oversimplifications |
Discovery and History: 120 Years of Oxytocin Science
The uterotonic effects of posterior pituitary extract were identified by British pharmacologist Henry Dale in 1906 when he showed that extracts of the posterior pituitary contracted the uterus of a pregnant cat.[1] By 1909, William Blair-Bell had performed the first clinical use to induce childbirth in complicated deliveries. The two posterior pituitary active principles were separated and named by Oliver Kamm and colleagues at Parke-Davis in 1928, giving us the terms “oxytocin” and “vasopressin.”
Vincent du Vigneaud at Cornell University Medical College determined oxytocin’s complete amino acid sequence in 1953 and achieved its total synthesis — the first total synthesis of a polypeptide hormone. Oxytocin contains nine amino acids (eight different amino acids) with a disulfide bond forming a link between two cysteines, in contrast to the hundreds of amino acids most other proteins contain. The 1955 Nobel Prize in Chemistry recognised this work, and synthetic oxytocin (Pitocin, Syntocinon) subsequently entered obstetric practice globally.[2] The modern social neuroscience era began with Thomas Insel’s characterisation of prairie vole bonding behaviour in the 1990s and accelerated with Kosfeld et al.’s 2005 Nature paper showing intranasal oxytocin increased trust in an investment game.[8]
Structure and Molecular Biology
Oxytocin’s structure is: Cys¹-Tyr²-Ile³-Gln&sup4;-Asn&sup5;-Cys&sup6;-Pro&sup7;-Leu&sup8;-Gly&sup9;-NH&sub2;. The critical structural feature is the disulfide bridge between Cys¹ and Cys&sup6;, forming a 6-amino acid ring with a 3-residue tail. The C-terminal amide (–NH&sub2;) is essential for biological activity.
The structure of oxytocin is very similar to that of vasopressin, differing only by two substitutions at positions 3 (Ile→Phe) and 8 (Leu→Arg).[4] Yet these molecules have fundamentally different physiological roles: oxytocin drives reproductive behaviour, pair bonding, and social cognition; vasopressin (ADH) regulates water balance and blood pressure. The structural similarity means oxytocin and vasopressin have partial cross-reactivity at each other’s receptors at higher concentrations — a pharmacological nuance that complicates interpretation of intranasal administration studies. The OXT gene on chromosome 20p13 encodes a preprohormone containing oxytocin and its neurophysin carrier, processed during axonal transport from the hypothalamic paraventricular and supraoptic nuclei to the posterior pituitary.
The Oxytocin Receptor (OXTR)
OXTR is a class A GPCR coupled primarily to Gαq/11, activating phospholipase C-β → IP&sub3; + DAG → intracellular Ca²+ release + PKC activation. OXTR can also couple to Gi in some tissue contexts. Key OXTR distribution sites: uterus (dense; drives myometrial contractions); mammary gland (milk ejection); amygdala (fear modulation and social memory); nucleus accumbens (reward and social motivation); hippocampus (social memory); hypothalamus (energy balance, satiety); brainstem/spinal cord (pain modulation); and peripheral organs including heart, kidney, and gut. The amygdala OXTR distribution is central to oxytocin’s anxiolytic and social cognition effects: oxytocin reduces amygdala activation to threatening stimuli and enhances attention to socially relevant cues.[4]
Approved (Obstetric) Uses
FDA-approved synthetic oxytocin is administered exclusively by IV infusion in clinical obstetrics. Indications: induction of labour at or near term for medical necessity; augmentation of labour not progressing adequately; oxytocin challenge test (antepartum foetal well-being assessment); control of postpartum uterine atony and haemorrhage; treatment of incomplete or inevitable abortion. Dosing (labour induction): IV infusion starting at 0.5–1 mU/min, increased every 30–60 minutes until adequate uterine contraction is established; typical therapeutic rates 6–25 mU/min.
Key safety considerations: Uterine hyperstimulation (tachysystole → foetal distress; requires continuous monitoring); antidiuretic effect at high doses (vasopressin receptor cross-activation → water retention → dilutional hyponatraemia, particularly with hypotonic IV fluids); cardiovascular (rapid IV bolus causes hypotension and reflex tachycardia; slow infusion used to avoid); receptor desensitisation with prolonged high-dose infusion, which may require second-line agents.
CNS Effects: The Social Neuroscience
The trust and prosocial effects (single dose, healthy volunteers)
Single-dose intranasal oxytocin research in healthy volunteers has produced relatively consistent findings: increased trust in investment games specifically when interacting with humans (not computers), demonstrating the effect is social rather than risk-related (Kosfeld 2005);[8] improved accuracy of facial emotion recognition, particularly for subtle or ambiguous expressions; increased fixation on the eye region of faces; and reduced amygdala BOLD response to threatening or fearful faces on fMRI — providing a neural mechanism for anxiolytic social effects. These single-dose acute effects are among the most consistently replicated findings in the social neuroscience literature.
The bidirectionality and context-dependence
⚠️ The simplistic “love hormone” narrative is contradicted by the complexity of oxytocin’s actual effects. Oxytocin promotes affiliation with individuals perceived as in-group, trustworthy, or familiar while potentially amplifying in-group/out-group distinctions. Intranasal oxytocin increased endorsement of sacrificing out-group members for in-group benefit in moral dilemmas (Hurlemann et al.). Oxytocin has been shown to increase defensive aggression toward perceived out-group threats. In competitive contexts, oxytocin amplifies schadenfreude. And in individuals with adverse childhood experiences or insecure attachment, oxytocin administration can paradoxically increase negative social cognition or anxiety rather than reducing it. Oxytocin is better described as a social salience enhancer that amplifies emotional significance toward social stimuli — both positive and negative — rather than a simply prosocial molecule.[9]
The Autism Saga: Promise, Disappointment, and Reassessment
The rationale
Several lines of evidence linked oxytocin to autism spectrum disorder (ASD): reduced circulating oxytocin levels found in some ASD children (Modahl, 1998); OXTR gene variants associated with ASD susceptibility; abnormal methylation of the OXTR gene in some ASD patients; and early small studies showing IV oxytocin infusion reduced repetitive behaviours in adults with ASD (Hollander et al., 2003). The mechanistic logic was plausible: ASD is characterised by social communication difficulties; the oxytocin system shows abnormalities in ASD; therefore supplementation might address core deficits.
The SOARS-B pivotal trial: negative result
The US NIMH-funded SOARS-B trial was the largest and most rigorously conducted oxytocin ASD trial: 272 youth with ASD, 24-week double-blind randomised treatment. Primary endpoint: Aberrant Behavior Checklist modified Social Withdrawal subscale. The trial failed its primary endpoint — no significant difference between oxytocin and placebo on ABC-mSW at weeks 12–24.[11]
A subsequent dose–response meta-analysis found that higher doses of oxytocin (48 IU/day) might be more effective for social impairments, and a 2025 machine learning re-analysis of SOARS-B found significant improvement in social-emotional reciprocity specifically — suggesting the primary outcome measure may not have captured the domain where oxytocin has its most specific effects.[12] A 2024 Nature Communications paper (Moerkerke et al.) showed that chronic oxytocin administration stimulates the oxytocinergic system in children with autism, providing mechanistic evidence of biological engagement even when primary behavioural endpoints were not met.[10]
Where the autism evidence stands now
Oxytocin does not produce broad improvement in global autism symptom burden in unselected ASD populations. It may produce specific improvements in social-emotional reciprocity in responsive subgroups. Pairing oxytocin with social skills interventions — using the oxytocin-enhanced social salience window to support social learning — is a more promising strategy than oxytocin alone. Optimal dosing and patient stratification (including baseline vasopressin levels) have not been established. The hypothesis is neither discredited nor established.
The Intranasal Bioavailability Problem
The fundamental question underlying all intranasal oxytocin research is: does intranasally administered oxytocin actually reach the brain in meaningful quantities? The olfactory mucosa provides a potential direct pathway to the CNS via olfactory neurons projecting to the olfactory bulb and via the trigeminal nerve, bypassing the blood-brain barrier. CSF studies have been mixed — some show CSF oxytocin elevation after intranasal dosing; others do not. A 2013 paper raised concerns that behavioural effects attributed to intranasal oxytocin might be mediated by peripheral sensory stimulation or placebo effects rather than direct CNS penetration. Whether sufficient quantities reach relevant brain circuits remains genuinely uncertain and is an active area of methodological debate. This uncertainty makes dose-response interpretation and inter-study comparison difficult.[9]
Clinical Evidence Summary
| Indication | Key finding | Evidence quality |
|---|---|---|
| Labour induction/augmentation | ✅ Effective; standard of care | Strong (approved) |
| Postpartum haemorrhage | ✅ Effective; standard of care | Strong (approved) |
| ASD — SOARS-B pivotal trial [11] | ❌ Negative primary endpoint (N=272, 24 weeks) | Moderate; single pivotal trial |
| ASD — meta-analysis [7] | No significant effect overall; 48 IU/day shows benefit | Moderate; inconsistent trials |
| ASD — social-emotional reciprocity [12] | Significant improvement (machine learning re-analysis, preprint) | Preliminary; not peer-reviewed |
| Social anxiety disorder | Mixed; some positive; no Phase 3 | Low-moderate |
| PTSD | Mixed; some evidence of symptom reduction | Low-moderate |
| Trust (healthy volunteers, single dose) [8] | ✅ Consistent enhancement; context-dependent | High for acute effect |
| Emotion recognition (healthy volunteers) | ✅ Consistent enhancement | Moderate-high |
Safety
Intranasal (research doses, 24–40 IU)
Generally well-tolerated in clinical trials. No serious adverse events documented at psychiatric research doses. Transient nausea, flushing, and mild drowsiness reported. No clinically significant cardiovascular effects at intranasal doses. Theoretical hyponatraemia concern at higher intranasal doses — not extensively studied. Chronic administration appears to stimulate rather than desensitise the endogenous oxytocinergic system (Moerkerke et al., Nature Communications 2024).[10]
Community use concerns
⚠️ Oxytocin can cause uterine contractions — absolute contraindication in pregnancy outside medically supervised obstetric contexts. Prostate tissue expresses OXTR; theoretical concern about stimulation in men with chronic use — no robust clinical data. Hyponatraemia risk with high-dose injection. No long-term safety data from large controlled trials exists for psychiatric applications.
Common Misconceptions
“Oxytocin is the love hormone — taking it will make you feel more love and bonded.”
Oxytocin increases social salience and emotional reactivity to social stimuli. In a supportive social context with a trusted person, this translates to enhanced warmth and bonding. In a competitive or threatening context, it can amplify in-group/out-group distinctions and even defensive aggression. “Love hormone” is a profound oversimplification that has contributed to uncritical community use.
“Intranasal oxytocin doesn’t work because it can’t cross the blood-brain barrier.”
The question is not BBB crossing (the intranasal-to-brain pathway bypasses the BBB via olfactory/trigeminal routes) but whether sufficient quantities reach relevant brain circuits. This remains genuinely uncertain and is an active methodological debate.
“The autism oxytocin trials failed, so oxytocin doesn’t work for social disorders.”
The SOARS-B failure means oxytocin doesn’t produce broad improvement across unselected ASD populations on global composite scales. It does not mean oxytocin has no effect on any social domain in any subgroup. The field is pursuing more targeted approaches: specific subpopulations, higher doses, combination with social skills interventions, and more domain-specific outcome measures.
“Pitocin and intranasal oxytocin are the same thing.”
The active molecule is identical, but context, dose, and route produce fundamentally different pharmacology. IV Pitocin operates at concentrations driving intense peripheral OXTR activation in the uterus. Intranasal oxytocin for psychiatric research uses much lower doses targeting potential CNS effects through a completely different delivery mechanism.
Frequently Asked Questions
Does oxytocin affect libido and sexual function?
Oxytocin rises during sexual arousal and peaks at orgasm. Whether exogenous administration affects sexual desire or function is not well-established in RCTs. PT-141/bremelanotide (Vyleesi), which does affect sexual desire, works through a completely different mechanism (melanocortin MC4R) — the two are not related pharmacologically despite popular confusion.
Is compounded intranasal oxytocin legal?
Compounded intranasal oxytocin occupies a regulatory grey area in the US. The FDA has approved synthetic oxytocin (Pitocin) for obstetric IV use only. Intranasal formulations are not FDA-approved for any indication. Compounding pharmacies may prepare intranasal oxytocin under 503A (patient-specific) provisions, but this requires a valid prescription from a licensed physician with a legitimate clinical rationale.
Can oxytocin help with PTSD?
Several small trials have explored intranasal oxytocin in PTSD, with mechanistic rationale: oxytocin reduces amygdala reactivity to threatening stimuli, potentially facilitating extinction of fear memories. Results have been mixed. No Phase 3 trial has established efficacy. The evidence is at the pilot/proof-of-concept stage.
Key Takeaways
- Oxytocin has one of the richest histories of any peptide in medicine — discovered 1906, sequenced and synthesised 1953 (Nobel Prize 1955), in obstetric use for over a century, and now at the centre of cutting-edge neuropsychiatry research.[2]
- ✅ The approved obstetric applications are well-established and clinically important. IV oxytocin for labour induction, augmentation, and postpartum haemorrhage control is standard of care globally, with a well-characterised risk profile.
- Single-dose prosocial effects in healthy volunteers are real but context-dependent. Oxytocin increases trust, emotion recognition, eye gaze to faces, and reduces amygdala threat responses. These acute effects are moderated by social context, relationship to target, and individual attachment history.[8]
- ⚠️ Oxytocin is not simply a “love hormone.” Its effects are bidirectional, amplifying social salience broadly — including ethnocentrism, in-group/out-group distinctions, and potentially defensive aggression. The popular narrative is a harmful oversimplification.
- ⚠️ The psychiatric treatment evidence base is genuinely incomplete and inconsistent. The SOARS-B pivotal autism trial was negative. Chronic treatment efficacy in clinical populations has not been established in Phase 3 trials for any psychiatric indication. Pairing oxytocin with social interventions and targeting responsive subgroups may be the path forward.[11]
- Intranasal bioavailability to the brain remains mechanistically contested. Whether and how much intranasally administered oxytocin reaches relevant CNS circuits in humans is a genuinely unsettled question that underlies much of the inconsistency in the research literature.
References
History and Discovery
- Dale HH. On some physiological actions of ergot. Journal of Physiology. 1906;34(3):163–206.
- Du Vigneaud V, Ressler C, Swan JM, et al. The synthesis of oxytocin. Journal of the American Chemical Society. 1954;76:3115–3121.
Pharmacology and Receptor Biology
- NIMH. Some selected history of oxytocin and vasopressin. nimh.nih.gov
- Gimpl G, Fahrenholz F. The oxytocin receptor system: structure, function, and regulation. Physiological Reviews. 2001;81:629–683.
- Young LJ, Wang Z. The neurobiology of pair bonding. Nature Neuroscience. 2004;7(10):1048–1054.
Clinical Trials and Reviews
- Espinoza D, Hollander E. Oxytocin in neurodevelopmental disorders: Autism spectrum disorder and Prader-Willi syndrome. Pharmacology & Therapeutics. 2024;264:108734. PMC12329755
- Zhang Y, Zhang X, Huang L. Optimal dose of oxytocin to improve social impairments and repetitive behaviors in autism spectrum disorders: meta-analysis and dose-response meta-analysis. Frontiers in Psychiatry. 2025;15:1477076.
- Kosfeld M, Heinrichs M, Zak PJ, Fischbacher U, Fehr E. Oxytocin increases trust in humans. Nature. 2005;435(7042):673–676.
- Bakermans-Kranenburg MJ, Van IJzendoorn MH. Sniffing around oxytocin: review and meta-analyses of trials in healthy and clinical groups with implications for pharmacotherapy. Translational Psychiatry. 2013. doi: 10.1038/tp.2013.34
- Moerkerke M, Daniels N, Tibermont L, et al. Chronic oxytocin administration stimulates the oxytocinergic system in children with autism. Nature Communications. 2024;15:58.
- Yamasue H, Okada T, Munesue T, et al. Effect of intranasal oxytocin on the core social symptoms of autism spectrum disorder: a randomized clinical trial. Molecular Psychiatry. 2020;25:1849–1858.
- Oxytocin enhances social-emotional reciprocity in autism. medRxiv. July 2025. doi: 10.1101/2025.07.20.25331870
Key Investigators
- Thomas R. Insel, MD — Former director NIMH; established the prairie vole model of oxytocin and pair bonding; first articulated the oxytocin-social cognition hypothesis in humans; instrumental in driving the clinical research programme.
- Eric Hollander, MD — Montefiore/Albert Einstein College of Medicine; conducted the first RCT of IV oxytocin in autism (2003); continues as a leading investigator of oxytocin for neurodevelopmental disorders.
- Markus Heinrichs, PhD — University of Freiburg; co-authored the Kosfeld 2005 Nature trust paper; leading investigator of single-dose intranasal oxytocin effects in healthy volunteers and clinical populations.
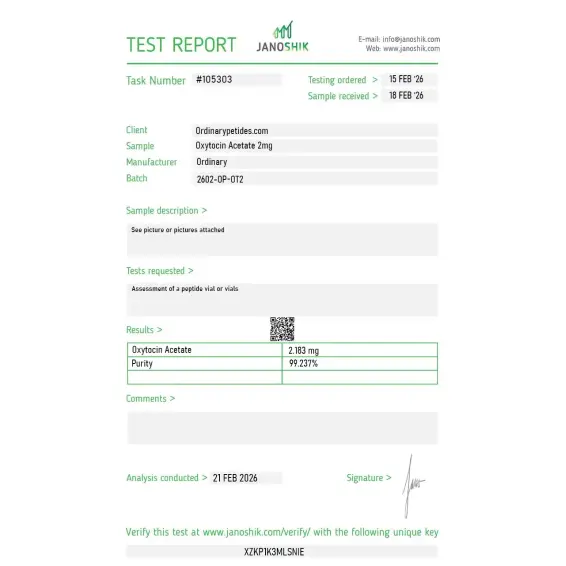
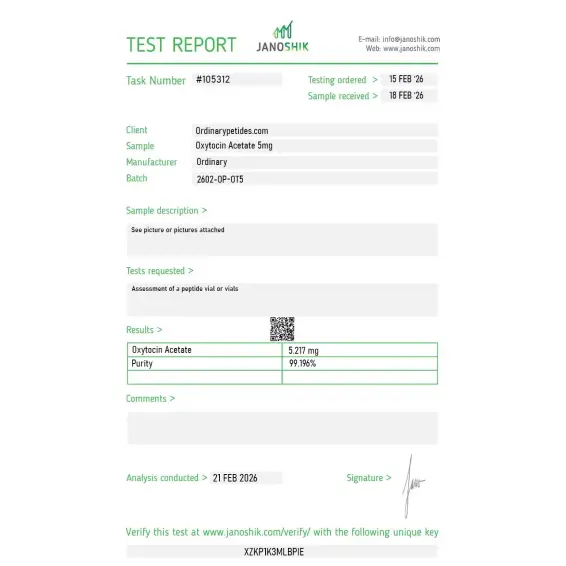
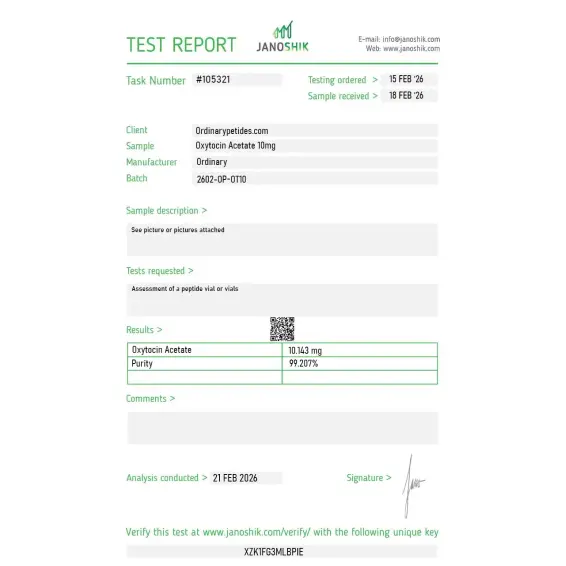
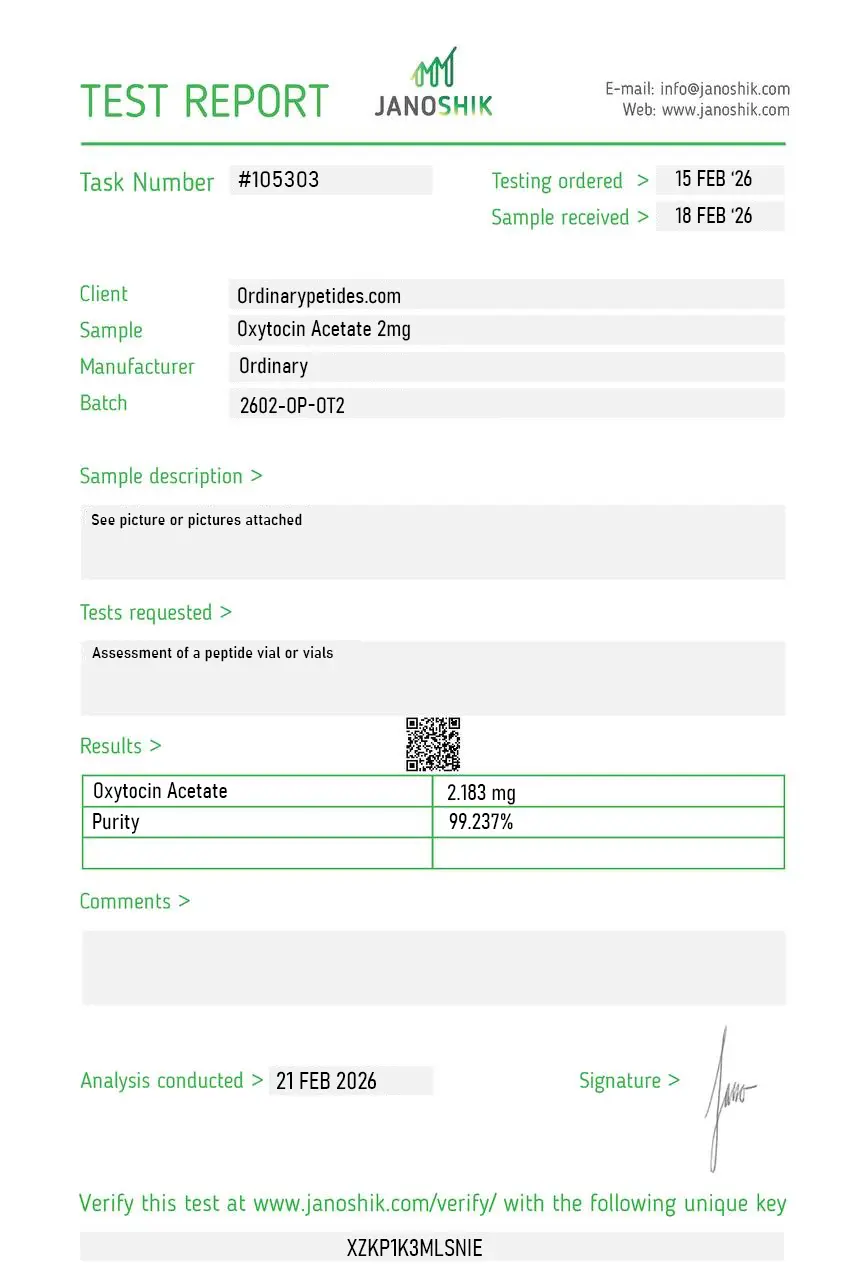
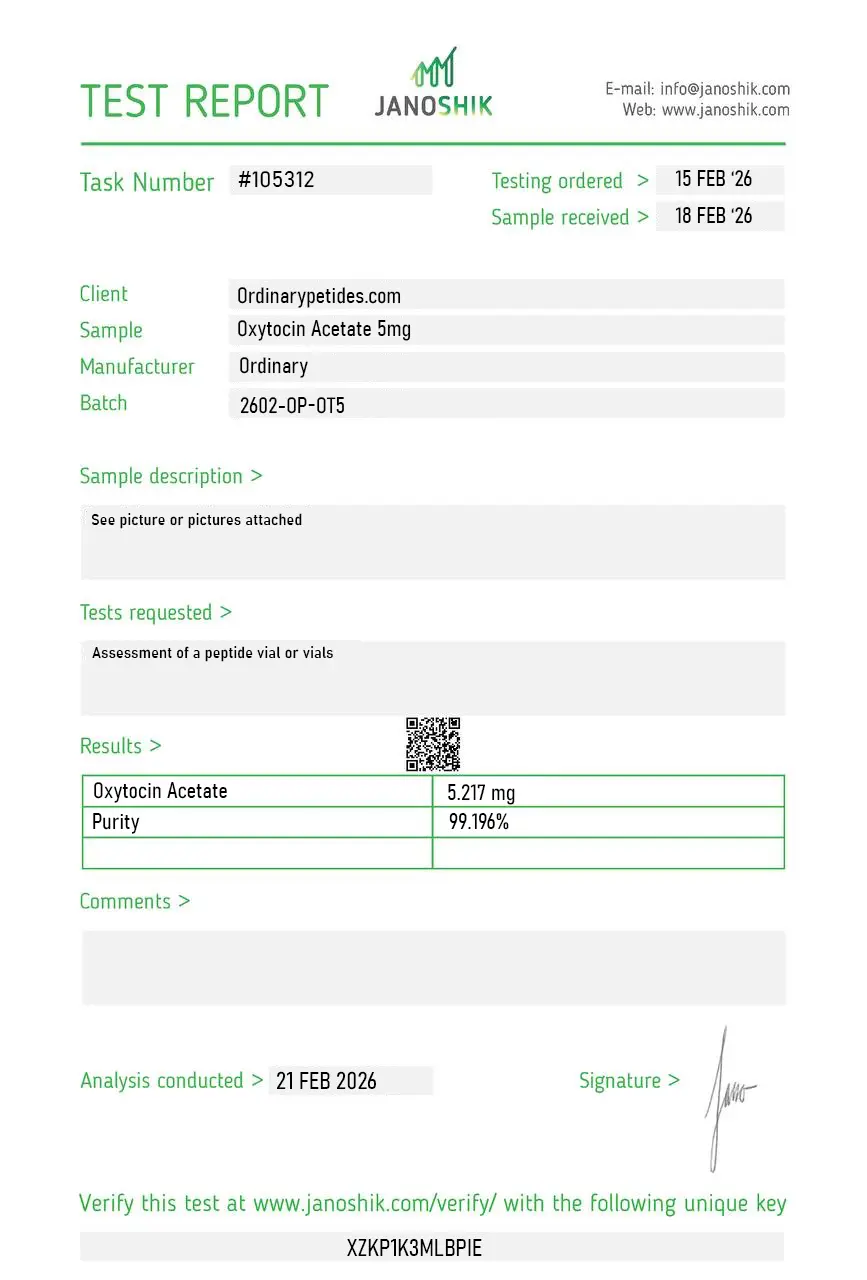
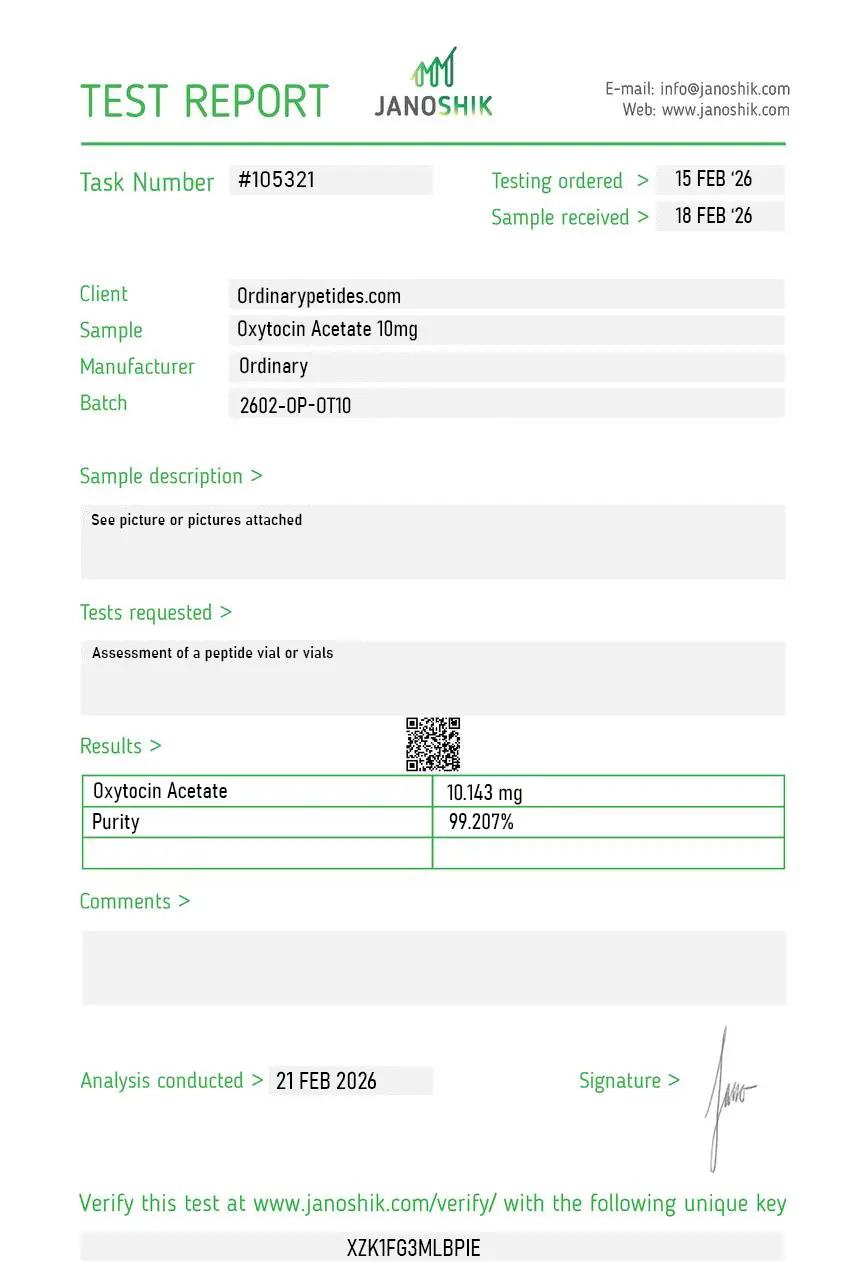
Certificate of Analysis
Independent test reports are available for Oxytocin Acetate 2mg, 5mg, and 10mg. These reports provide batch-level documentation and analytical verification information for research reference.
Based on 1 reviews
5.0
The structural twinship with vasopressin is what we actually study — oxytocin and vasopressin differ at only two positions (Ile-3/Phe-3 and Leu-8/Arg-8 respectively) yet drive entirely different physiology, and that minimal-sequence-difference yet maximal-function-divergence is one of the most elegant examples in receptor pharmacology. For probing how single-residue substitutions reshape receptor binding across the OXTR/AVPR family, oxytocin is one half of the canonical pair. The material activated OXTR cleanly with the expected modest AVPR1A cross-reactivity in our parallel readouts.
It is a salt form of oxytocin, not a new mechanism of action. The active biology is tied to the oxytocin molecule itself.It is a salt form of oxytocin, not a new mechanism of action. The active biology is tied to the oxytocin molecule itself.
Clinical obstetric oxytocin products are traditionally labeled in international units, whereas research or other commercial products may use mass in milligrams. That does not automatically make them interchangeable.
No. Scientifically, it is more accurate to consider it a hormonal peptide with proven obstetric use and researched, but not definitively established, non-obstetric effects.
In some experiments, changes in social processing or behavior are observed, but this is not a universal or guaranteed effect, and the data depend strongly on context.
More as a research object than as a routine treatment standard. The evidence base for broad practical use is still insufficiently convincing.
Oxytocin acetate is the acetate salt form of synthetic oxytocin — a naturally occurring nonapeptide (nine amino acids) produced in the paraventricular nucleus and supraoptic nucleus of the hypothalamus and stored and released by the posterior pituitary gland. Its molecular structure was determined by Vincent du Vigneaud in 1953 — work that earned the Nobel Prize in Chemistry in 1955 — and synthetic oxytocin has been in clinical medical use for over 60 years. It is often called the "love hormone" or "bonding hormone" due to its central roles in social attachment, trust, and reproductive behavior, but this colloquial framing substantially undersells the complexity and breadth of its physiology. Pharmaceutical oxytocin (Pitocin, Syntocinon) is FDA-approved and widely used in obstetric medicine. Oxytocin acetate as a research and wellness compound refers to synthetic oxytocin used outside these approved obstetric indications — primarily intranasally for neuropsychiatric and social wellness applications — where it has no current FDA approval.
Oxytocin operates through two distinct release pathways that serve different purposes. Peripheral oxytocin released from the posterior pituitary into the bloodstream drives physiological effects — stimulating uterine smooth muscle contractions during labor through Gq-coupled receptor signaling that increases intracellular calcium, contracting myoepithelial cells in mammary glands for milk ejection, and cardiovascular effects including vasodilation. Central oxytocin released directly from oxytocinergic neurons projecting throughout the brain modulates social behavior, emotional memory, trust, anxiety, stress response, and sexual function. These two pathways are partially independent — peripheral oxytocin does not readily cross the blood-brain barrier, which is why intranasal administration is preferred for central effects, as nasal delivery provides direct access to the olfactory and trigeminal pathways that bypass the blood-brain barrier and achieve higher brain concentrations than IV at equivalent doses. Oxytocin's central effects involve interactions with serotonin, dopamine, GABA, glutamate, opioids, and the HPA axis, and it extensively interacts with vasopressin at overlapping receptors — a complexity that makes its pharmacology in humans considerably more nuanced than its popular reputation suggests.
IV and intramuscular oxytocin (Pitocin, Syntocinon) is FDA-approved for labor induction and augmentation, postpartum hemorrhage prevention and treatment, and management of incomplete abortion. These are well-established, heavily used obstetric applications administered under hospital monitoring due to the potency and precision required.
Over 27,000 published papers on oxytocin as of 2020 reflect an extraordinarily broad research base. The most extensively studied non-obstetric areas include social bonding and trust — intranasal oxytocin reliably increases trust in economic game paradigms, improves interpersonal closeness, and enhances positive social cues in controlled studies. Anxiety and stress reduction through cortisol suppression and HPA axis modulation has been consistently demonstrated in short-term studies. Autism spectrum disorder research has been the most clinically prominent area — multiple trials have examined oxytocin's effects on social functioning in ASD, with some showing improvements in social responsiveness and emotional recognition, though results are mixed and no regulatory approval has been achieved for this indication. Psychiatric applications including schizophrenia, PTSD, borderline personality disorder, and addiction have all been subjects of clinical trials. Sexual function — oxytocin reliably enhances arousal and orgasm intensity in both men and women in controlled studies. Appetite regulation and weight management through MC4R and hypothalamic pathway interactions has been explored. Pain modulation through central sensitization pathways has been documented. Anti-inflammatory and antioxidant effects, particularly relevant to trauma and stress, have been established preclinically.
Intranasal spray is the most common route for research and wellness applications — typically 10 to 40 IU per dose administered 20 to 60 minutes before the intended effect, using a dedicated nasal spray device. Subcutaneous injection is also used in wellness clinic settings. Sublingual troches, topical gel, and vaginal cream formulations have been compounded. Brain concentrations after nasal application are substantially higher than after equivalent IV doses, making intranasal the preferred route for central neurological effects. The very short plasma half-life of approximately 1 to 6 minutes means effects are acute and require timely administration relative to the intended application.
For intranasal use at research doses the side effect profile is generally mild. Headache, nasal irritation and congestion, transient drowsiness, mild dizziness, nausea, and occasional mood shifts including irritability or blunted affect are the most commonly reported effects. Blood pressure reduction through peripheral vasodilation can occur and requires monitoring in sensitive populations. For IV obstetric doses more serious risks apply — uterine hyperstimulation causing fetal distress, dilutional hyponatremia from antidiuretic properties at high doses, reflex tachycardia and hypotension, and rare anaphylaxis. A concern specific to men receiving chronic low-dose oxytocin is potential prostate tissue stimulation — robust clinical data is limited but some clinicians advise against daily chronic use in men for this reason. The complexity of oxytocin-vasopressin receptor cross-reactivity means context-dependent and individually variable responses are common — the same dose can produce trust-enhancing effects in some individuals and heightened anxiety or in-group favoritism in others.
Pregnant women outside labor management settings should not use it given the risk of premature uterine contractions. People with established cardiovascular conditions including arrhythmias or unstable blood pressure should be cautious given cardiovascular effects. Those prone to severe anxiety, panic attacks, or mood disorders should use it only under clinical supervision given the potential for paradoxical emotional reactions. People with hyponatremia or conditions predisposing to low sodium should avoid it. Known allergy to oxytocin or formulation components is a contraindication. Men with prostate conditions should discuss risks with their physician. For all non-obstetric applications it should be understood that while the research base is substantial, no regulatory approval exists for these uses and the evidence for efficacy in most conditions remains inconclusive despite the volume of published studies.





