

MGF
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
MGF: More Than a "Muscle Peptide"
MGF sounds like a straight-up muscle peptide, but the reality is much messier — and more interesting: it is a term tied to the IGF-1 system, usually linked to a splice variant such as IGF-1Ec, not a simple standalone molecule in a vial. In the research context, MGF-related biology has been associated with the early response to mechanical load, tissue stress, and regeneration, which is exactly why it caught so much attention in muscle and repair studies.
But here is the twist: the "MGF" sold online is often a short synthetic E-domain peptide or PEG-MGF, and published reviews stress that this is not the same thing as the natural endogenous variant. In preclinical work, MGF-related models showed intriguing signals across muscle, cartilage, bone, ligaments, and other tissues, yet the data were mixed, and some studies did not confirm the big muscle-growth narrative around the short peptide.
That makes MGF compelling not as a clean, proven shortcut, but as a complex research topic where the biology is real and the marketing is often way too confident. For a client who wants something genuinely thought-provoking to explore, MGF stands out precisely because the science is fascinating — and refuses to fit into a lazy hype slogan.
MGF (Mechano Growth Factor / IGF-1Ec): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
MGF occupies a peculiar place in the peptide pharmacology landscape. It is simultaneously one of the most biologically compelling and scientifically contested peptides in the muscle biology literature — a compound with strong preclinical evidence for satellite cell activation, neuroprotection, cardiac repair, and tendon healing, yet with a serious replication failure at its pharmacological core: researchers at GSK and AstraZeneca were unable to reproduce the foundational finding that the synthetic 24-amino acid MGF E-peptide stimulates muscle cell proliferation.[4]
The story begins in the mid-1990s at University College London. Geoffrey Goldspink and colleagues identified that mechanical stress on skeletal muscle triggers preferential splicing of the IGF-1 gene toward a specific isoform — IGF-1Ec in humans — before the more familiar circulating form (IGF-1Ea) is upregulated. They isolated a 24-amino acid synthetic peptide corresponding to the unique C-terminal E-domain and demonstrated that this peptide activates quiescent muscle satellite cells and promotes their proliferation while delaying terminal differentiation.[2][3] The pharmaceutical industry took notice; WADA prohibited MGF class peptides in 2005 before any human trials had been designed; and the sports doping community adopted it even earlier.
| At a glance | |
|---|---|
| Full names | Mechano Growth Factor; IGF-1Ec (humans); IGF-1Eb (rodents) |
| E-peptide sequence | YQPPSTNKNTKSQRRKGSTFEEHK (24 amino acids, human) |
| Molecular weight | ~2,867 Da (E-peptide); full-length IGF-1Ec is larger |
| Gene | IGF1 (chromosome 12q23.2); exons 4–6 splicing |
| Discovery | 1996, Geoffrey Goldspink and colleagues, University College London |
| Proposed mechanism | Satellite cell activation → proliferation; delay of terminal differentiation |
| Key controversy | ⚠️ Foundational muscle cell proliferation finding not reproduced by GSK/AstraZeneca |
| WADA status | ❌ Prohibited since 2005 — S2 (Peptide Hormones, Growth Factors) |
| FDA status | ❌ Not approved; not in clinical trials |
| Human evidence | ❌ None — no human clinical trials completed |
Biology: The IGF-1 Gene and Alternative Splicing
The IGF1 gene on chromosome 12q23.2 contains six exons expressed through multiple tissue- and stimulus-specific promoters. Alternative splicing at the 3’ end generates distinct propeptide isoforms differing only in their C-terminal “E-domain” extension. IGF-1Ea is the dominant liver-derived circulating form. IGF-1Ec (humans) — MGF — includes exon 5, causing a reading frameshift that produces a unique 24-amino acid C-terminal E-domain. All isoforms share the identical 70-amino acid mature IGF-1 domain that binds the IGF-1 receptor; what makes MGF distinct is entirely its C-terminal E-domain extension, present in the uncleaved propeptide and cleaved away during post-translational processing.
The mechano-sensitive response
The temporal sequence of isoform expression after muscle damage or exercise is well-established: within hours of mechanical stress, MGF (IGF-1Ec) mRNA expression rises acutely — the first IGF-1 splice variant to respond. Research has shown that after injury to skeletal muscle, the IGF-IEb/Ec mRNA splice variant is up-regulated initially, followed by up-regulation of IGF-IEa at later time points. Up-regulation of IGF-IEb mRNA correlates with markers of satellite cell and myoblast proliferation, whereas up-regulation of IGF-IEa mRNA is correlated with differentiation to mature myofibers.[10] This temporal correlation with satellite cell activation is the biological basis for the “MGF hypothesis.”
Age-related decline in MGF response
MGF expression in response to exercise declines with age. Hameed et al. (2003) showed that both young and elderly men upregulate MGF mRNA after resistance exercise, but the response is blunted in older individuals.[5] This age-dependence is consistent with sarcopenia biology and represents the therapeutic logic for MGF as a potential sarcopenia intervention — supplementing the blunted endogenous MGF response in older muscle.
The Proposed Mechanism: The MGF Hypothesis
The MGF hypothesis proposes that after muscle injury, the IGF1 gene is first spliced toward the Ec (MGF) variant. The MGF peptide is responsible for activating quiescent satellite cells to enter the cell cycle and develop into mononucleated myoblasts, while also promoting myoblast proliferation and inhibiting premature differentiation. Levels of MGF must then decrease for differentiation to occur. During the myoblast proliferative stage, splicing increasingly shifts toward the Ea variant, which promotes further myoblast proliferation and potentiates differentiation into multinucleated myotubes.[10]
A critical unresolved issue is what receptor the MGF E-peptide acts through — if it acts autonomously at all. Several studies report E-peptide effects not blocked by IGF-1 receptor antibodies, suggesting a distinct receptor. However, no analogous peptide product of the IGF1 gene has been identified in or isolated from cultured cells, their conditioned medium, or in vivo biological fluids — raising the foundational question of whether the free 24-amino acid E-peptide actually exists endogenously as a circulating signal.
The Replication Crisis at the Heart of MGF Biology
The original findings (Yang and Goldspink, 2002; Hill and Goldspink, 2003)
The foundational papers from the Goldspink laboratory at UCL reported that the synthetic 24-amino acid MGF E-peptide stimulates proliferation of C2C12 mouse myoblasts and delays their terminal differentiation through an IGF-1 receptor-independent mechanism. These findings were widely cited and became the basis for subsequent satellite cell studies, ALS research, cardiac work, and the entire community use rationale.[2][3]
The replication failure (Tinworth et al., 2014 — GSK/AstraZeneca)
In 2014, researchers at GlaxoSmithKline and AstraZeneca published a systematic attempt to reproduce the MGF E-peptide myoblast findings under rigorous conditions. Concentrations of peptide up to 500 ng/mL failed to increase the proliferation of C2C12 cells or primary human skeletal muscle myoblasts. In contrast, all cell types exhibited a proliferative response to mature IGF-1 or full-length IGF-1Ec. The researchers also tested signalling pathways directly: whereas control mature IGF-1 stimulated Akt, ERK, and p70 S6K phosphorylation, neither form of MGF peptide increased phosphorylation of any marker. These results call into question whether there is a physiological role for MGF E-peptide.[4]
Interpreting the discrepancy
Several explanations have been proposed. Peptide stability: Synthetic MGF E-peptide is rapidly degraded in biological media within minutes; early positive experiments may have used freshly prepared peptide at effective concentrations before degradation. Cell line vs. primary cells: Some positive results used C2C12 cell lines, which behave differently from primary human satellite cells; Tinworth et al. tested both and found no effect in either. Full-length isoform vs. E-peptide: The full-length IGF-1Ec did produce robust proliferative responses in the GSK/AZ experiments — only the isolated E-peptide fragment did not. This suggests the biological activity of the intact splice variant is real, mediated through the shared IGF-1 domain acting on the IGF-1 receptor, but the autonomous E-peptide hypothesis may be incorrect.[10]
The pharmacological rationale for administering the synthetic MGF E-peptide — whether truncated native, D-Arg stabilised, or PEGylated — as a muscle growth agent rests on a hypothesis that has not been validated by independent pharmaceutical-grade replication. The endogenous mRNA and full-length protein are real and biologically important. Whether the 24-amino acid synthetic fragment that community users inject replicates this biology is genuinely uncertain.
Evidence by Application Domain
Muscle hypertrophy and satellite cell activation
In vitro (Goldspink lab): Multiple papers from UCL demonstrate MGF E-peptide stimulation of C2C12 proliferation and muscle hypertrophy. These remain the primary foundational studies but have not been independently reproduced in primary human satellite cells by pharmaceutical-grade investigators. In vivo (rodent): Gene delivery of full-length IGF-1Ec (AAV-MGF) to rodent muscle consistently produces hypertrophy, satellite cell expansion, and functional improvement in both healthy and dystrophic models. These use full-length isoform gene delivery — not synthetic E-peptide — and are more reproducible and credible than the E-peptide cell culture data.[3] Age-related sarcopenia: The MGF E-peptide increases the proliferative lifespan of satellite cells isolated from young but not old adult muscle — suggesting an age-dependent response threshold that would limit utility in the primary target population for sarcopenia treatment.[6]
Neuroprotection
The neuroprotection evidence is arguably more compelling than the muscle data — no equivalent pharmaceutical replication failure has been published. Dluzniewska et al. (2005, FASEB Journal) demonstrated that the MGF E-peptide produced potent neuroprotective effects in both in vitro neuronal cultures exposed to excitotoxicity and in vivo rat brain ischaemia models, independent of the IGF-1 receptor — suggesting a genuine autonomous E-peptide mechanism in neurons. MGF but not IGF-1Ea was found overexpressed in the regenerating regions following global adult brain ischaemia.[7] The neuroprotection findings have been reproduced across multiple species and ischaemic models. If MGF has a clinical future, neuroprotection may be a more defensible development pathway than muscle hypertrophy.
Cardioprotection
Carpenter et al. (2008) demonstrated that MGF reduced loss of cardiac function in an acute myocardial infarction model. Localised delivery through injectable microrods (Peña et al., 2015) demonstrated sustained MGF E-peptide release that reduced cardiomyocyte apoptosis and improved cardiac function in a post-infarction rodent model.[8][9] This localised delivery approach — which avoids systemic exposure and plasma degradation — may represent a more viable therapeutic strategy than systemic peptide injection. The MGF E-peptide also appears to stimulate pro-angiogenic activities in human vascular endothelial cells and increase mesenchymal stem cell migration to injury sites.
ALS and neuromuscular disease
Gene delivery of MGF increased progenitor cells in ALS, dystrophic, and normal muscle in rodent models, with significantly more motor neurons surviving in MGF-treated animals compared to those receiving full-length IGF-1 constructs alone. These are gene delivery experiments using full-length isoform expression — not systemic synthetic E-peptide injection. The therapeutic benefit in neuromotor disease is plausible but requires a long development pathway that has not been initiated.
Evidence summary
| Application | Model | Form used | Finding | Evidence quality |
|---|---|---|---|---|
| Satellite cell activation | In vitro, cell lines | E-peptide | Positive (Goldspink lab) | Low; not reproduced by industry |
| Satellite cell activation | In vitro, primary human cells | E-peptide | ❌ Negative (GSK/AZ) | Moderate; rigorously controlled |
| Muscle hypertrophy | In vivo rodent | Gene delivery (full-length) | Positive | Moderate; gene therapy, not peptide |
| Satellite cells, old adult | Primary human | E-peptide | ❌ No effect (Kandalla 2011) | Moderate; therapeutically relevant failure |
| Neuroprotection | In vitro + rodent | E-peptide | Positive, IGF-1R independent | Moderate; not reproduced in humans |
| Cardioprotection | Rodent MI model | E-peptide (local delivery) | Positive | Moderate; preclinical only |
| Human clinical trials | None | — | No data | N/A |
The Cancer Question
⚠️ Preferential expression of IGF-1Ec/MGF transcript has been found in cancerous human prostate tissue compared to normal tissue. The E-peptide activates mesenchymal stem cell migration toward tumours — a mechanism that could promote tumour repair and progression. In prostate cancer cell lines, IL-6 from the immune environment activates JAK/STAT3 signalling that upregulates IGF-1Ec expression and E-peptide secretion.[10]
The satellite cell proliferation mechanism — if it actually works — is the same mitogenic stimulation that could support tumour growth in cancer contexts. Whether exogenously administered MGF would promote occult or existing malignancies is unknown and untested. The IGF axis more broadly is well-established in cancer biology: MGF, as a pro-proliferative component of the IGF-1 family expressed preferentially in cancer tissue, carries a plausible oncological risk that no human safety study has characterised.
MGF Variants: What Is Actually Available
| Form | Description | Half-life | Notes |
|---|---|---|---|
| Truncated native MGF (24aa) | Exact human E-domain sequence; YQPPSTNKNTKSQRRKGSTFEEHK | Minutes in plasma | Rapidly degraded; requires frequent injection; least characterised |
| Goldspink MGF (R23H, D-Arg) | D-Arg substitutions at positions 13–16; His at position 23 | Significantly extended | Patent WO 2006/097764; designed for stability; somewhat analogous to rodent sequence |
| PEG-MGF | Polyethylene glycol conjugated to N-terminal Tyr | Several hours | Extended systemic exposure; anti-PEG antibodies may develop with repeated dosing |
The PEGylation rationale is pharmacokinetically sound: MGF’s endogenous expression window spans hours, but plasma-administered E-peptide is gone within minutes without modification. PEG-MGF provides exposure that more closely matches the endogenous temporal window. Whether this extended exposure translates to biological benefit in humans is unknown — no human trials of any MGF variant have been conducted. PEGylated peptides can also induce anti-PEG antibodies with repeated dosing, potentially reducing efficacy and causing hypersensitivity.
Regulatory and Commercial Status
| Jurisdiction | Status |
|---|---|
| FDA | ❌ Not approved; no IND filed; no clinical trials |
| EMA | ❌ Not approved |
| WADA | ❌ Prohibited since 2005 — S2 (Peptide Hormones) |
| Pharmaceutical development | No company has advanced MGF to Phase 1 clinical trials as of April 2026 |
Common Misconceptions
“MGF is just a local form of IGF-1 — same effects.”
MGF shares the 70-amino acid IGF-1 domain with all IGF-1 isoforms but has a distinct C-terminal E-domain proposed to have autonomous biological activity. The endogenous isoform is real and biologically relevant. Whether the synthetic 24-amino acid E-peptide replicates its activity is contested.
“The replication failure is just a methodological disagreement.”
The GSK/AstraZeneca team used rigorously controlled conditions — multiple cell types, primary human satellite cells, multiple concentrations up to 500 ng/mL, multiple endpoints including downstream signalling markers. Their finding that full-length IGF-1Ec and mature IGF-1 produced the expected responses while only the E-peptide fragment failed is methodologically meaningful, not a minor discrepancy.[4]
“WADA banned it so it must work.”
WADA banned MGF based on preclinical promise and doping potential — the same basis on which WADA has prohibited other compounds that later failed in clinical development. Prohibition reflects risk management by a sports regulatory body, not clinical validation of efficacy.
Frequently Asked Questions
Is there any human evidence for MGF?
No. Not a single completed human clinical trial has been published for any MGF variant. All human-relevant evidence is inferential: measurement of endogenous MGF mRNA expression in human muscle biopsies after exercise (which confirms the endogenous biology but says nothing about exogenous administration), and in vitro studies using human primary cells that show inconsistent effects depending on age and experimental conditions.
Why hasn’t pharmaceutical development advanced further?
The replication failure is the most likely explanation. Pharmaceutical companies require target validation before entering clinical development. If the foundational in vitro finding — satellite cell proliferation in response to the E-peptide — cannot be reproduced in primary human cells by independent rigorous methods, the target validation required for an IND filing is not present. The cardiac and neuroprotection signals are potentially more robust, but those require different clinical indication strategies (localised device-based delivery rather than systemic injection) that have not been commercially prioritised.[4]
What is PEG-MGF and is it safer than regular MGF?
PEG-MGF is the E-peptide conjugated to polyethylene glycol at the N-terminal tyrosine residue, reducing renal clearance and proteolytic degradation and extending plasma half-life from minutes to several hours. Safety: PEGylated proteins can induce anti-PEG antibodies with repeated dosing (the “accelerated blood clearance” phenomenon), potentially reducing efficacy and causing hypersensitivity reactions. No human safety data exists for PEG-MGF specifically.
Key Takeaways
- MGF is real biology. The IGF-1Ec splice variant is expressed in human muscle in response to exercise and damage, preceding IGF-1Ea expression by hours, in a pattern consistent with early satellite cell activation. Its age-dependent blunting is consistent with sarcopenia biology. The endogenous mRNA and full-length protein are not in question.
- ⚠️ The synthetic E-peptide is the contested part. Whether the 24-amino acid C-terminal fragment — divorced from the mature IGF-1 domain — has autonomous biological activity sufficient to activate satellite cells is genuinely unclear. The Goldspink lab says yes; GSK/AstraZeneca independently found no effect. This is the central unresolved scientific question.[4]
- ⚠️ No human clinical trials have been conducted for any MGF variant. All translational extrapolation from rodent gene therapy, cell culture, and endogenous expression data to human subcutaneous peptide injection is inferential and unvalidated.
- The evidence for neuroprotection and cardiac repair is more robust than the muscle evidence — it involves different mechanistic endpoints, has been reproduced across systems, and shows IGF-1R-independent effects consistent with a genuine E-peptide mechanism. If MGF has a therapeutic future, it may be in these applications via localised delivery.[7][9]
- ⚠️ The cancer concern is real and uncharacterised. MGF/IGF-1Ec is overexpressed in prostate cancer and other malignancies. The E-peptide can mobilise mesenchymal stem cells toward tumour environments. No human safety study has characterised oncological risk from exogenous MGF administration.
- Community use precedes the science by decades. The evidence base has, if anything, become less certain since widespread use began in the early 2000s — as rigorous replication work raised questions about the foundational mechanism. This is the opposite of the usual trajectory where evidence accumulates over time to support clinical use.
References
Discovery and Foundational Biology
- Goldspink G, et al. Alternative splicing of the insulin-like growth factor-1 gene in skeletal muscle in response to exercise and stretch. Molecular and Cellular Endocrinology. 1996.
- Yang SY, Goldspink GE. Different roles of the IGF-I Ec peptide (MGF) and mature IGF-I in myoblast proliferation and differentiation. FEBS Letters. 2002;522(1-3):156–160.
- Hill M, Goldspink G. Expression and splicing of the IGF gene in rodent muscle associated with satellite cell activation following tissue damage. Journal of Physiology. 2003;549(Pt 2):409–418.
Replication Failure
- Tinworth CP, et al. Mechano-growth factor peptide, the COOH terminus of unprocessed IGF-1, has no apparent effect on myoblasts or primary muscle stem cells. American Journal of Physiology — Endocrinology and Metabolism. 2014. doi: 10.1152/ajpendo.00408.2013
Age-Related Evidence
- Hameed M, Orrell RW, Cobbold M, et al. Expression of IGF-I splice variants in young and old human skeletal muscle after high resistance exercise. Journal of Physiology. 2003;547:247–254.
- Kandalla PK, Goldspink G, Butler-Browne G, Mouly V. MGF-E, derived from an isoform of IGF-1, activates human muscle progenitor cells and induces an increase in their fusion potential at different ages. Mechanisms of Ageing and Development. 2011;132(4):154–162. PMID: 21354439
Neuroprotection
- Dluzniewska J, et al. A strong neuroprotective effect of the autonomous C-terminal peptide of IGF-1 Ec (MGF) in brain ischaemia. FASEB Journal. 2005;19(13):1896–1898. PMID: 16144956
Cardioprotection
- Carpenter V, et al. Mechano-growth factor reduces loss of cardiac function in acute myocardial infarction. Heart, Lung and Circulation. 2008;17:33.
- Peña JR, et al. Localized delivery of mechano-growth factor E-domain peptide via polymeric microstructures improves cardiac function following myocardial infarction. Biomaterials. 2015;46:26–34. PMC4328136
Review Articles
- Zabłocka B, Goldspink PH, Goldspink G, Górecki DC. Mechano-Growth Factor: an important cog or a loose screw in the repair machinery? Frontiers in Endocrinology. 2012;3:131. PMC3485521
- Matheny RW Jr, et al. Minireview: Mechano-growth factor — a putative product of IGF-I gene expression involved in tissue repair and regeneration. Endocrinology. 2010. PMID: 20130113
Doping and Detection
- Thomas A, et al. Mass spectrometric characterisation of a biotechnologically produced full-length mechano growth factor relevant for doping controls. Analytica Chimica Acta. 2014. PMID: 25466910
- Esposito S, et al. Characterisation and identification of a C-terminal amidated mechano growth factor analogue in black market products. Rapid Communications in Mass Spectrometry. 2012. PMID: 22328223
- Goldspink G. Research on mechano growth factor: its potential for optimising physical training as well as misuse in doping. British Journal of Sports Medicine. 2005;39:787. PMC1725070
Key Investigator
- Geoffrey Goldspink, PhD (1935–2019) — University College London, Royal Free Hospital; discovered the mechano-sensitive IGF-1 splicing response in skeletal muscle; coined the term “Mechano Growth Factor”; published the foundational E-peptide satellite cell biology; held patent WO 2006/097764 on stabilised MGF analogues.
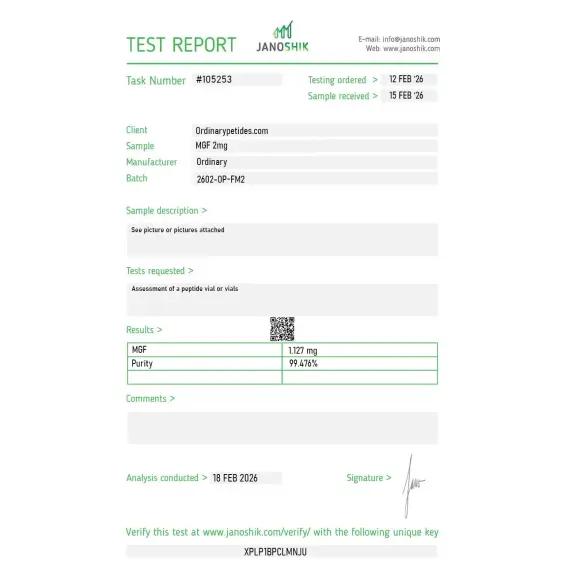
Certificate of Analysis
An independent test report is available for MGF 2mg. This report provides batch-level documentation and analytical verification information for research reference.

For the IGF-1Ec splice context the certificate should clarify that this is the cleaved E-peptide rather than the full IGF-1Ec precursor — they're confused in the literature, and a buyer ordering "MGF" could receive either depending on the vendor's definition. The cleaved 24-residue E-peptide is what produces the mechano-signaling effects in most published work, not the uncleaved splice variant. Material was the cleaved form when we verified, but the precursor-versus-cleaved distinction belongs unambiguous on the listing.
The local-autocrine nature is the entire research point — native MGF is the short-lived E-peptide that diffuses only briefly from the cell that produced it, signaling locally before degradation, which is exactly opposite the systemic-circulation logic of most peptide hormones. For studying paracrine and autocrine signaling kinetics where the short half-life IS the experimental condition rather than a flaw, native MGF is the right tool. The material behaved with the expected rapid signaling-and-clearance profile in our myoblast culture.
It is more accurate to say that MGF is a term associated with a splice variant within the IGF-1 system. The short synthetic MGF peptide popular on the market is not automatically the same thing as the body's natural product. (PubMed)
In a number of models — yes, the expression of the MGF-associated variant increases after mechanical stress, training, or tissue damage.
No, there is no convincing clinical evidence base for that claim.
Mechano Growth Factor (MGF), also known as IGF-1Ec, is an alternatively spliced isoform of the insulin-like growth factor-1 (IGF-1) gene. In humans, mechanical stress or damage to muscle tissue triggers the IGF-1 gene to splice via a 49-base pair insert in exon 5, producing a reading frame shift that generates a distinct C-terminal E-domain sequence — the defining feature of MGF that separates it from the liver-type IGF-1Ea isoform. MGF is produced locally within mechanically stressed tissue — primarily skeletal muscle — rather than systemically from the liver like mature IGF-1. It was first identified and characterized in the 1990s by Professor Geoffrey Goldspink at University College London. As a research peptide, "MGF" typically refers to the synthetic 24-amino acid C-terminal E-domain peptide (MGF-Ct24E or MGF-24aa-E), which is the biologically active fragment studied in isolation. PEG-MGF refers to a polyethylene glycol-modified version designed to extend the very short natural half-life of the peptide for research use.
No, MGF is included on the WADA prohibited list.
MGF is typically supplied as a lyophilized (freeze‑dried) powder intended for laboratory or research use, which helps preserve peptide stability.
MGF should be stored sealed and cooled (typically at or below −20 °C) to protect the peptide from degradation. Suppliers often recommend protecting it from moisture and light.
Products labeled for research containing MGF are generally marked for laboratory research use only and are not intended for human or veterinary therapeutic use, unless explicitly approved in your jurisdiction.
Research indicates that the endogenous MGF peptide is produced in muscle tissue after exercise or injury and is involved in local cellular responses related to muscle repair and adaptation. However, the scientific understanding of its role in skeletal muscle biology continues to be explored and is not fully established.
MGF and mature IGF-1 share the same N-terminal mature peptide sequence — both produce IGF-1 receptor signaling — but MGF's unique C-terminal E-domain appears to operate through distinct, IGF-1 receptor-independent pathways as well. The E-domain peptide activates satellite cells — the resident muscle stem cells responsible for muscle repair and growth — keeping them in a proliferative, non-differentiating state and expanding the pool of myonuclei available for muscle fiber repair and hypertrophy. This is mechanistically distinct from mature IGF-1, which drives differentiation. The E-domain peptide activates MAPK-ERK1/2 signaling rather than the PI3K/Akt pathway more associated with mature IGF-1, and has been shown to activate Nrf2 through PKC, increasing heme oxygenase-1 expression for neuroprotection. Critically, the E-domain peptide has been demonstrated in published studies to have 1.4-fold greater proliferative activity in osteoblasts than mature IGF-1, and its effects on satellite cell activation appear distinct from and complementary to the differentiation-driving effects of mature IGF-1.
MGF research presents a genuinely complex and contested picture that is unusually honest to acknowledge. Supporting evidence from Goldspink's group and others includes intramuscular cDNA injection producing 25% increase in fiber cross-sectional area within two weeks in animals, E-domain peptide activating human muscle progenitor cells across age groups in published cell culture studies, cardiac protection in sheep myocardial infarction models, neuroprotection in brain ischemia models, bone defect healing in rabbit models, cartilage repair activity in chondrocyte models, and tendon healing promotion. However a strongly negative 2013 paper by Fornaro et al — representing pharmaceutical company muscle research groups — found that synthetic MGF E-domain peptide failed to stimulate proliferation in C2C12 muscle cells, human myoblasts, or mouse satellite cells, while mature IGF-1 did stimulate proliferation. A published editorial titled "The Fall of Mechano Growth Factor?" critically examined confirmation bias in MGF research and concluded the field had not adequately distinguished between the effects of the E-domain itself versus the mature IGF-1 produced when the full prohormone is processed. The biological question of whether the E-domain functions as an independent active peptide in vivo — as distinct from simply being a processing intermediate en route to mature IGF-1 — remains genuinely unresolved.
Despite the mechanistic uncertainty, published preclinical research has explored MGF in skeletal muscle repair and hypertrophy, age-related sarcopenia — where MGF expression declines with aging in both animals and humans, potentially contributing to muscle loss — cardiac protection following myocardial infarction, neuroprotection in ischemia and Parkinson's disease models, bone healing, cartilage repair in osteoarthritis models, tendon healing, and Duchenne muscular dystrophy where MGF increased progenitor cell numbers. The cardiovascular research is particularly notable — intracoronary MGF E-domain peptide outperformed mature IGF-1 in improving hemodynamic function after myocardial infarction in sheep.
In research contexts MGF is given by intramuscular or subcutaneous injection. Its natural half-life in vivo is extremely short — minutes — making sustained systemic effects from injectable peptide pharmacologically challenging. PEG-MGF addresses this by attaching a polyethylene glycol chain that significantly extends circulation time, allowing once or twice weekly dosing. Research protocols typically cite 200 to 400 mcg per injection for the standard form with more frequent dosing, or similar doses for PEG-MGF on a less frequent schedule. It is not FDA-approved and cannot be legally compounded in the United States. It is banned by WADA.
MGF has a generally mild reported side effect profile in research contexts, reflecting its endogenous origin as a locally produced tissue repair signal. The most commonly reported effects are injection site redness, swelling, and discomfort. Temporary fatigue and transient changes in muscle fullness have been noted. The primary theoretical concerns mirror those of IGF-1 class compounds — IGF-1 receptor pathway activation carries the general oncological concern that promoting cell proliferation could potentially benefit malignant cells in addition to normal ones, though MGF's distinct MAPK-ERK1/2 mechanism and local rather than systemic activity profile are argued to reduce this risk compared to systemic IGF-1 therapies.
People with active cancer or cancer history should not use it given the cell proliferation-promoting mechanism. Competitive athletes are prohibited from its use under WADA. Pregnant or breastfeeding women should not use it. Anyone considering it should understand the fundamental scientific uncertainty about whether the synthetic E-domain peptide actually produces the postulated effects in vivo in humans — this is not a compound with a clear, replicated, mechanistically confirmed human evidence base comparable even to the modest data supporting BPC-157.





