
PEG MGF
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
PEG MGF: More Hype Than Clarity
PEG MGF is not a "smart recovery peptide," but a pegylated synthetic construct that grew out of the already confusing MGF/IGF-1Ec concept. In the research context, interest in it emerged because MGF-related peptides were linked in preclinical models to muscle adaptation, cell proliferation, and recovery processes after loading and injury.
But the real catch is that PEG MGF is no longer simply an idea about a local IGF-1 signal — it is a chemically modified variant that moves even further away from natural physiology. In the published human data, there is no convincing clinical evidence base, and the FDA specifically highlights the absence of human exposure data as well as concerns about immunogenicity, impurities, and characterization of the substance itself.
That is why PEG MGF is interesting not as a ready-made solution, but as a controversial research object in which the scientific intrigue is clearly greater than the level of proof. For the client, this is the kind of case where the real interest comes not from the promise of "recovering faster," but from the complex biological story itself — one that is still not fully pieced together.
PEG-MGF (PEGylated Mechano Growth Factor): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
PEG-MGF is a chemically modified derivative of Mechano Growth Factor (MGF) — the same 24-amino acid C-terminal E-domain peptide of the IGF-1Ec splice variant — to which one or more polyethylene glycol (PEG) chains have been covalently attached. The modification was created to solve a fundamental pharmacological problem: the unmodified peptide has a plasma half-life measured in minutes, making it essentially unusable as a subcutaneously administered therapeutic. PEGylation extends this from minutes to somewhere in the range of several hours to potentially 24–72 hours, transforming a practically impractical research tool into a compound with genuine systemic bioavailability.
The critical caveat, which this article makes explicit: the biological evidence cited for PEG-MGF — muscle satellite cell activation, cardiac protection, neuroprotection — is almost entirely from experiments using the native MGF E-peptide, not the PEGylated form. Whether PEGylation preserves the E-peptide’s biological activity, alters receptor binding kinetics, or changes the net biological effect are questions that have not been systematically answered in the peer-reviewed literature. Furthermore, the commercially available “PEG-MGF” contains two additional modifications beyond PEGylation (D-arginine substitutions and a histidine substitution at position 23), making it a triply-modified compound that is further still from the canonical sequence studied in the preclinical literature.
| At a glance | |
|---|---|
| Parent compound | MGF E-peptide (24 amino acid C-terminal E-domain of IGF-1Ec); see MGF article in this series |
| Modification | Covalent conjugation of polyethylene glycol (PEG) to the N-terminal tyrosine |
| Commercial sequence | PEG-Suc-YQPPSTNKNTKSQ[D-Arg][D-Arg]KGSTFEEHK-NH&sub2; |
| Modifications from canonical sequence | PEGylation + D-Arg×2 (positions 13–14) + R23H |
| Native MGF E-peptide half-life | ~5–7 minutes in plasma |
| PEG-MGF claimed half-life | Several hours (conservative) to 48–72 hours (commercial claims; not peer-reviewed) |
| Biological evidence | ⚠️ Almost entirely from native E-peptide studies, not PEG-MGF specifically |
| Foundational replication status | ⚠️ GSK/AstraZeneca failed to reproduce satellite cell activation in primary human muscle cells (see MGF article) |
| Human clinical trials | ❌ None |
| WADA | ❌ Prohibited — S2 (Peptide Hormones, Growth Factors, Related Substances) |
What PEGylation Is and Why It Matters
The PEG chemistry
Polyethylene glycol (PEG) is a synthetic, water-soluble polymer of repeating ethylene oxide units: –(CH&sub2;–CH&sub2;–O)n–. It is biologically inert, non-immunogenic in most individuals, approved as a food additive and pharmaceutical excipient, and widely used in medicine. PEGylation — the covalent attachment of PEG chains to a molecule — is one of the most successful strategies in biopharmaceutical engineering, having been applied to interferon, erythropoietin, asparaginase, and numerous other biologics. For the MGF E-peptide, PEGylation is attached at the N-terminal tyrosine hydroxyl group through a succinimidyl (Suc) linker: PEG-Suc-[E-peptide]. The PEG chain size used commercially varies but typically ranges from 2–20 kDa.[5]
How PEGylation extends half-life
Two mechanisms operate simultaneously. First, increased hydrodynamic radius: a peptide conjugated to a 20 kDa PEG chain has an apparent hydrodynamic radius far exceeding the renal glomerular filtration threshold (~8 nm). The freely soluble 2.8 kDa MGF E-peptide is rapidly filtered by the kidney; the PEG-conjugated form is not. Second, steric protection from proteolysis: PEG chains create a dense hydration shell (“PEG cloud”) around the peptide that physically blocks access by proteolytic enzymes. Together these mechanisms extend a 5–7-minute plasma half-life to hours or longer.
The half-life controversy
Commercial claims for PEG-MGF half-life range widely: some sources claim 48–72 hours based on comparisons with similar PEGylated biologics; more conservative preclinical data suggests several hours. Available pharmacokinetic data (AUC 292 hr·µg/L, Cmax 37 µg/L after single SC dose) suggests hours rather than days of meaningful exposure at the Cmax level. The honest answer is that PEG-MGF half-life has not been rigorously characterised in peer-reviewed human pharmacokinetic studies. Commercially circulated figures are extrapolations from similar PEGylated compounds or from preclinical data that may not reflect the specific formulation’s PEG size and conjugation chemistry.
The Commercial Sequence: What Is Actually Being Sold
The “PEG-MGF” available in the research chemical market is not simply the canonical 24-amino acid MGF E-peptide with PEG attached. The commercial product has three modifications from the canonical native human MGF E-peptide: N-terminal PEG conjugation (the pharmacokinetic modification); D-arginine substitutions at positions 13 and 14 (protease resistance); and a histidine substitution at position 23 — R23H (similar to the “Goldspink MGF” or “consensus MGF” sequence more closely resembling the rodent form). Geoffrey Goldspink held patent WO 2006/097764 A1 on the stabilised MGF analogue design.[10]
The practical significance: the studies cited in support of PEG-MGF’s biological effects used the canonical 24-amino acid native sequence (YQPPSTNKNTKSQRRKGSTFEEHK), not the D-Arg/R23H/PEG-modified commercial sequence. Whether the commercially sold compound produces equivalent, superior, or inferior effects to the studied native sequence is unknown.
Pharmacokinetic Rationale: Why PEGylation Was Necessary
Native MGF E-peptide has a plasma half-life of approximately 5–7 minutes, eliminated through renal filtration and proteolytic degradation. Peak plasma concentration after SC injection occurs at approximately 30 minutes, and plasma levels are negligible by 60–90 minutes. Tissue penetration from the systemic compartment requires sustained plasma concentrations over time — a single SC injection of native MGF cannot provide the multi-hour exposure window needed for satellite cell activation (which requires receptor engagement over hours, not minutes). The endogenous MGF expression window after muscle damage spans 0–24 hours at the mRNA level, with peak expression at 2–6 hours. PEG-MGF’s extended half-life is explicitly designed to approximate this endogenous exposure window. This pharmacokinetic rationale is internally coherent. Its limitation is that it assumes the synthetic E-peptide produces biological effects that warrant this extended exposure — an assumption the GSK/AstraZeneca replication failure substantially qualifies.[3]
BBB penetration: a key disadvantage relative to native MGF
The increased hydrodynamic radius that protects PEG-MGF from renal clearance and proteolysis also impairs its transit across the blood-brain barrier and blood-CSF barrier. This creates a pharmacokinetic irony: the neuroprotection evidence (Dluzniewska et al. 2005), which is among the more reproduced and credible MGF E-peptide findings, may be specifically less accessible to systemically administered PEG-MGF than to either native E-peptide or locally delivered unPEGylated peptide.[9]
The Anti-PEG Antibody Problem
⚠️ This class effect of PEGylated therapeutics receives insufficient attention in the community context. Anti-PEG antibodies (APAs) are detectable in 25–40% of the general population due to ubiquitous PEG exposure from consumer products. Accelerated blood clearance (ABC phenomenon): in individuals with pre-existing or induced APAs, subsequent doses of PEGylated compounds are cleared 50–90% faster than the initial dose — potentially rendering chronic dosing ineffective. The ABC phenomenon has been documented with PEGylated liposomes, PEGylated proteins, and other PEGylated therapeutics. Whether it occurs with PEG-MGF at research doses is unknown, but the theoretical consequence — that the claimed pharmacokinetic advantage of PEGylation may diminish or disappear with repeated dosing — is a real concern that is not acknowledged in community-oriented discussions of PEG-MGF.[6]
Evidence: What Is Attributed to PEG-MGF vs. What Came From Native MGF Studies
Most websites and commercial sources describe the following evidence as applying to “PEG-MGF.” In almost every case, the underlying studies used the native MGF E-peptide, not the PEGylated commercial compound.
Satellite cell activation and muscle repair
Yang and Goldspink (2002) demonstrated satellite cell activation using native E-peptide on C2C12 myoblasts. Kandalla et al. (2011) showed effects in young adult human satellite cells. Tinworth et al. (2014, GSK/AstraZeneca) found no effect at 500 ng/mL in primary human skeletal muscle myoblasts. Whether PEGylated E-peptide with D-Arg substitutions produces equivalent responses is not demonstrated in peer-reviewed literature.[1][3][4]
Cardioprotection
Carpenter et al. (2008) showed that intracoronary delivery of native MGF E-peptide reduced loss of cardiac function after myocardial infarction in a sheep model. Peña et al. (2015) demonstrated that microrod-delivered native E-peptide reduced cardiomyocyte apoptosis in a rodent MI model. These used localised delivery of native E-peptide — not systemic subcutaneous PEG-MGF.[7][8]
Neuroprotection
Dluzniewska et al. (2005) demonstrated potent neuroprotection by native E-peptide in neuronal culture excitotoxicity and in vivo rat brain ischaemia models, through IGF-1R-independent mechanisms — among the more robustly reproduced MGF findings. The BBB limitation of PEG-MGF is a specific obstacle to applying this finding to systemically administered PEG-MGF.[9]
Bone healing
Deng et al. (2011, International Orthopaedics) showed that native MGF E-peptide promotes osteoblast proliferation and accelerates bone defect healing in rabbits. Applicability to PEG-MGF requires assuming equivalent pharmacodynamics with the PEGylated, D-Arg-substituted commercial sequence.
Evidence Summary
| Domain | Source compound | Model | Finding | Applicability to commercial PEG-MGF |
|---|---|---|---|---|
| Satellite cell activation | Native E-peptide | C2C12 cells (Goldspink lab) | Positive | Not confirmed; replication failure in primary human cells (GSK/AZ) |
| Satellite cell (primary human) | Native E-peptide | Primary human (young adult) | Positive (age-dependent) | Not confirmed with PEG form |
| Satellite cell (primary human) | Native E-peptide | Primary human (pharmaceutical industry) | ❌ Negative at 500 ng/mL | Applies to E-peptide; PEG form not tested |
| Cardioprotection | Native E-peptide (local delivery) | Sheep MI model | Positive | Localised delivery only; PEG-MGF untested |
| Neuroprotection | Native E-peptide | Rodent ischaemia | Positive (most reproducible MGF finding) | PEG-MGF has reduced BBB penetration |
| Bone healing | Native E-peptide | Rabbit | Positive | Different compound; extrapolation uncertain |
| Muscle hypertrophy | Full-length IGF-1Ec (gene delivery) | Rodent | Positive | Gene delivery ≠ synthetic E-peptide injection |
| Human clinical trials | Any MGF form | None | No data | No data |
Comparison: Native MGF vs. PEG-MGF vs. Goldspink MGF
| Feature | Native E-peptide (canonical) | Goldspink MGF (stabilised) | Commercial PEG-MGF |
|---|---|---|---|
| Sequence | YQPPSTNKNTKSQRRKGSTFEEHK | YQPPSTNKNTKSQR[D-R]K[H23]GSTFEEHK | PEG-Suc-YQPPSTNKNTKSQ[D-R][D-R]K[H23]GSTFEEHK |
| Modifications from native | None | D-Arg×1, R23H | PEGylation + D-Arg×2 + R23H |
| Half-life | ~5–7 minutes | Extended (hours) | Extended (hours to days; unverified) |
| BBB penetration | Some | Reduced | Significantly reduced |
| Peer-reviewed biological studies | Yes — most MGF literature | Limited | Essentially none as standalone compound |
| WADA prohibited | ❌ Yes | ❌ Yes | ❌ Yes |
Regulatory and Anti-Doping Status
WADA prohibited MGF-class peptides in 2005 and explicitly includes PEGylated forms under S2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics). Detection methods for PEG-MGF are technically more challenging than for native MGF because the PEG moiety alters mass spectrometric fragmentation patterns, and the commercial D-Arg-substituted sequence differs from the canonical human sequence, complicating sequence-based detection. Anti-PEG antibody assays could theoretically detect exposure but are not specific to MGF.
Safety Considerations
No formal toxicological characterisation of the synthetic MGF E-peptide has been published in peer-reviewed literature. Preclinical studies report no serious adverse events at therapeutic doses in rodent and ovine models. PEGylation-specific concerns include anti-PEG antibodies and accelerated blood clearance (discussed above); PEG accumulation (2–20 kDa PEG sizes are generally considered safe based on the pharmaceutical literature); and growth factor concerns common to all compounds that drive cell proliferation (potential promotion of occult malignancy, off-target tissue hypertrophy, disruption of endogenous IGF-1 axis regulation). Commercial PEG-MGF with D-Arg substitutions and R23H is a novel chemical entity relative to the studied native sequence — its metabolic fate, off-target receptor binding profile, and immunogenicity have not been characterised.[6] No human pharmacokinetic, pharmacodynamic, or safety studies of PEG-MGF have been published.
Common Misconceptions
“The studies on MGF prove PEG-MGF works.”
The relevant biological studies used the native 24-amino acid E-peptide — not the PEGylated, D-Arg-substituted commercial compound. Whether these findings transfer to the commercial PEG-MGF product is an assumption, not an established fact.
“The extended half-life means PEG-MGF is strictly superior to native MGF.”
Extended half-life is only beneficial if the compound is biologically active over that extended period. If the E-peptide mechanism is questioned (as the GSK/AZ replication failure suggests), an extended half-life prolongs exposure to a compound of uncertain efficacy. The BBB limitation is a genuine disadvantage for neuroprotective applications specifically.
“PEG reduces immunogenicity, so PEG-MGF is safer.”
⚠️ PEGylation reduces immune response to the peptide itself, but can generate immune responses against the PEG moiety. The accelerated blood clearance phenomenon from anti-PEG antibodies is a real pharmacological concern that may specifically undermine the extended half-life that justifies PEG-MGF’s development.
“Twice-weekly injection protocol is based on the pharmacokinetics.”
Standard community protocols (200–400 µg twice weekly) are not derived from human pharmacokinetic data — no such data exists. They are empirically derived from community experience, extrapolated from animal data, and adjusted based on perceived cost-benefit. They have no scientific validation.
Frequently Asked Questions
Is PEG-MGF just MGF with a longer half-life?
Not exactly. Commercial PEG-MGF is the MGF E-peptide with PEGylation plus D-arginine substitutions plus a histidine substitution at position 23. It is a distinct chemical entity from the native E-peptide studied in most preclinical work. The pharmacokinetic advantage is real in principle; whether the biological activity of the modified compound equals that of the native peptide is not established.
Does the GSK/AstraZeneca replication failure mean PEG-MGF doesn’t work?
Not definitively. Tinworth et al. found no effect of the native E-peptide in primary human myoblasts at up to 500 ng/mL.[3] This challenges the foundational claim that the E-peptide has autonomous biological activity in muscle cells independent of the full-length IGF-1 domain. It does not rule out biological activity in other cell types (neurons, cardiac cells, MSCs) or through mechanisms not captured in proliferation assays. It does substantially qualify confidence in the primary claimed benefit.
Why is PEG-MGF so popular in bodybuilding if the evidence is uncertain?
The muscle satellite cell activation hypothesis is biologically compelling and mechanistically plausible, even if the replication failure introduces genuine doubt. The peptide is cheap to synthesise, easy to obtain, and the claimed effects align with what athletes desire. Community use has been occurring since the early 2000s — preceding the GSK/AZ replication failure paper by a decade. The research chemical market does not require the evidence bar that pharmaceutical development demands.
Key Takeaways
- PEGylation solves a genuine pharmacological problem. Native MGF E-peptide has a 5–7 minute plasma half-life that makes subcutaneous administration impractical. PEGylation extends this to hours or longer, enabling systemic administration. This rationale is scientifically coherent.
- ⚠️ The biological evidence is for native MGF E-peptide, not PEG-MGF. Almost every study cited in support of PEG-MGF’s effects used the canonical 24-amino acid unmodified sequence, not the PEGylated, D-Arg-substituted commercial compound. These findings do not automatically transfer.
- ⚠️ The foundational satellite cell mechanism is contested. The GSK/AstraZeneca replication failure (2014) found no effect of native E-peptide in primary human muscle cells at 500 ng/mL.[3] The neuroprotection findings are more reproducible but PEG-MGF has reduced CNS penetration due to the PEG moiety.
- ⚠️ Anti-PEG antibodies and accelerated blood clearance are real and underacknowledged risks. Repeated PEG-MGF administration can induce APAs that reduce efficacy and may cause hypersensitivity. The long-term pharmacokinetic profile of PEG-MGF with repeated dosing is not characterised.[6]
- ⚠️ No human clinical trials exist. Not a single published pharmacokinetic, pharmacodynamic, or safety study in humans exists for any PEG-MGF formulation. All human-relevant claims are extrapolated from preclinical data using related but not identical compounds.
- Commercial PEG-MGF is a triply-modified novel entity relative to the studied canonical sequence. PEGylation + two D-Arg substitutions + R23H creates a compound whose characterisation in the peer-reviewed biological assays that produced the cited evidence is absent.
References
Foundational MGF Biology (see also the MGF article in this series)
- Yang SY, Goldspink GE. Different roles of the IGF-I Ec peptide (MGF) and mature IGF-I in myoblast proliferation and differentiation. FEBS Letters. 2002;522(1-3):156–160.
- Hill M, Goldspink G. Expression and splicing of the IGF gene in rodent muscle associated with satellite cell activation following tissue damage. Journal of Physiology. 2003;549(Pt 2):409–418.
- Tinworth CP, et al. Mechano-growth factor peptide, the COOH terminus of unprocessed IGF-1, has no apparent effect on myoblasts or primary muscle stem cells. American Journal of Physiology — Endocrinology and Metabolism. 2014. doi: 10.1152/ajpendo.00408.2013
- Kandalla PK, Goldspink G, Butler-Browne G, Mouly V. MGF-E peptide activates human muscle progenitor cells and induces an increase in their fusion potential at different ages. Mechanisms of Ageing and Development. 2011;132(4):154–162.
PEGylation and Class Effects
- Veronese FM, Pasut G. PEGylation, successful approach to drug delivery. Drug Discovery Today. 2005;10(21):1451–1458.
- Chen BM, Cheng TL, Roffler SR. Polyethylene glycol immunogenicity: theoretical, clinical, and practical aspects of anti-polyethylene glycol antibodies. ACS Nano. 2021;15(9):14022–14048.
Cardioprotection (native E-peptide)
- Carpenter V, Matthews K, Devlin G, et al. Mechano-growth factor reduces loss of cardiac function in acute myocardial infarction. Heart, Lung and Circulation. 2008;17:33–39.
- Peña JR, Pinney JR, Ayala P, Desai TA, Goldspink PH. Localized delivery of mechano-growth factor E-domain peptide via polymeric microstructures improves cardiac function following myocardial infarction. Biomaterials. 2015;46:26–34. PMC4328136
Neuroprotection (native E-peptide)
- Dluzniewska J, Sarnowska A, Beresewicz M, et al. A strong neuroprotective effect of the autonomous C-terminal peptide of IGF-1 Ec (MGF) in brain ischaemia. FASEB Journal. 2005;19(13):1896–1898. PMID: 16144956
Patent and Review
- Goldspink G. Modified IGF-I peptides. International Patent WO 2006/097764 A1.
- Zabłocka B, Goldspink PH, Goldspink G, Górecki DC. Mechano-Growth Factor: an important cog or a loose screw in the repair machinery? Frontiers in Endocrinology. 2012;3:131. PMC3485521
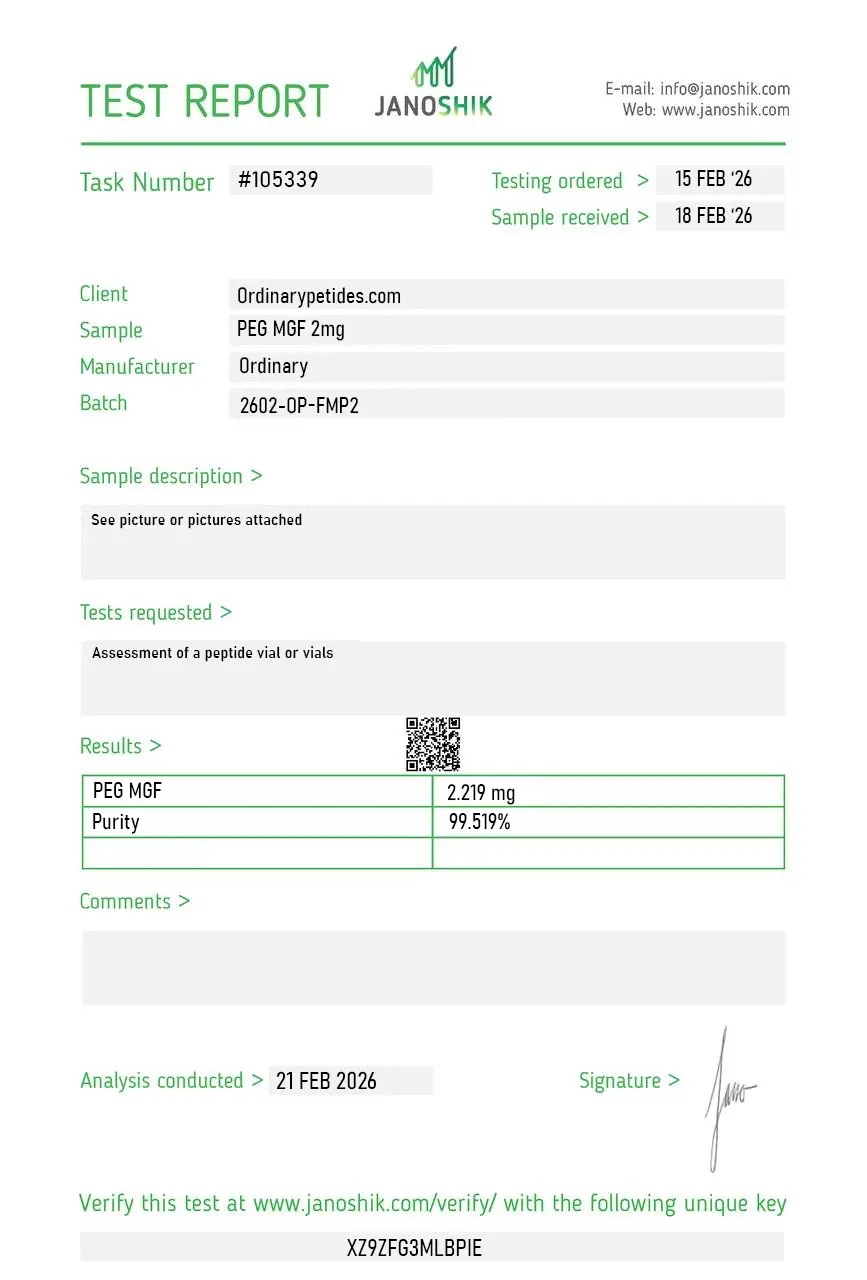
Certificate of Analysis
An independent test report is available for PEG-MGF 2mg. This report provides batch-level documentation and analytical verification information for research reference.
Based on 1 reviews
5.0
We use PEG-MGF in immunogenicity-screening work — PEG itself can elicit anti-PEG antibodies in some preparations, and that immune response can compromise efficacy on repeat exposure regardless of the underlying peptide's biology. For studying anti-PEG immunogenicity as a class-wide concern across PEGylated therapeutics, PEG-MGF is a reasonable model conjugate. The material gave consistent results in our anti-PEG-antibody detection assays.
No, not in the usual sense. It is a synthetic peptide derivative associated with the MGF/IGF-1Ec concept, not a standard endogenous hormonal drug.
No. PEG MGF is a modified, pegylated version of a synthetic MGF peptide.
Based on available data, no. The FDA does not identify a human exposure base for it and emphasizes the lack of safety information.
That is a popular interpretation of a preclinical idea, not a proven clinical fact in humans.
Yes. MGF belongs to prohibited growth factors under WADA rules.
PEG-MGF (Polyethylene Glycol Mechano Growth Factor) is a chemically modified version of the synthetic MGF E-domain peptide (MGF-Ct24E) in which one or more polyethylene glycol (PEG) chains are covalently attached to the peptide backbone. PEGylation is a well-established pharmaceutical engineering technique used to extend the circulating half-life of biologically active molecules — the same technology applied to PEGylated forms of interferon, erythropoietin, and numerous other approved drugs. In the case of MGF the motivation is straightforward and critical: native MGF has an extremely short serum half-life of only a few minutes in biological fluids, making it pharmacokinetically impractical as an injectable therapeutic. PEGylation dramatically extends this, creating a longer-acting form capable of producing sustained circulating levels after less frequent injection. It is not FDA-approved, cannot be legally compounded in the United States, and is banned by WADA.
The PEG chain works by creating a large hydrophilic shell around the peptide that dramatically increases its hydrodynamic radius in solution. This larger molecular size slows renal filtration, which primarily clears small peptides, extending circulation time from minutes to days. The PEG chain also shields the peptide from proteolytic enzymes that would otherwise rapidly degrade it in serum. The result is a compound that, instead of requiring multiple daily injections to maintain any meaningful plasma presence, can be injected once or twice weekly while maintaining relevant circulating levels. This pharmacokinetic improvement was one of the explicit scientific goals of PEG-MGF development — published research directly compared native MGF and PEG-MGF stability in serum and documented the dramatic improvement in half-life with PEGylation.
Beyond pharmacokinetics there is a meaningful mechanistic distinction. Standard MGF E-domain peptide, with its very short half-life, acts as an acute local signal — when produced endogenously in mechanically stressed muscle it creates a brief, localized pulse that activates satellite cells in the immediate vicinity of the damaged tissue. This local-acting character may be part of why it evolved with such rapid clearance. PEG-MGF, by contrast, circulates systemically for extended periods after injection. This means its effects are not limited to a local injection site but can theoretically reach satellite cells throughout the body — a fundamentally different distribution pattern from the endogenous molecule. Whether this systemic, sustained activation of satellite cells produces the same qualitatively beneficial effects as the brief, local endogenous signal — or whether it disrupts the carefully timed pulsatile signaling that may be important for normal muscle regeneration — is not established in human data.
The most commonly cited research applications for PEG-MGF mirror those of standard MGF but with the advantage of practical dosing frequency. Muscle repair and hypertrophy — activation of satellite cells to expand the myonuclear pool available for muscle fiber growth and repair. Age-related sarcopenia — since MGF expression declines with age and PEG-MGF could theoretically restore this signaling in aged muscle, it has been studied in the context of combating age-related muscle loss. Neuroprotection — the same E-domain neuroprotective effects documented for standard MGF in ischemia models apply to PEG-MGF, with the extended circulation potentially enhancing CNS exposure. Cardiac protection — the MGF E-domain's documented cardioprotective effects in myocardial infarction models are of interest in a form that can be delivered less invasively. Connective tissue repair including tendon and bone healing studies in animal models. The same fundamental scientific controversy about whether the E-domain itself is the bioactive species — or whether observed effects reflect IGF-1 receptor activity from the mature IGF-1 produced when the prohormone is processed — applies to PEG-MGF equally.
PEG-MGF is given by subcutaneous injection, typically once or twice weekly — a major practical advantage over native MGF which would theoretically require daily or more frequent dosing. Research protocols and anecdotal wellness protocols cite doses ranging from 200 to 400 mcg per injection. It is supplied as a lyophilized powder reconstituted with bacteriostatic water. It is commonly used in cycles of 4 to 6 weeks. It is sometimes stacked with IGF-1 LR3, CJC-1295, or other growth factor peptides in performance and recovery protocols, on the premise that MGF's satellite cell activation is complementary to IGF-1's differentiation-driving effects — though no human combination data supports this.
PEG-MGF shares the side effect profile of standard MGF with some additional PEGylation-specific considerations. Injection site reactions including redness, swelling, and pain are the most commonly reported effects. Transient fatigue and temporary increases in muscle fullness or density are noted. The theoretical risks inherent to any IGF-1 axis compound — potential effects on cell proliferation and the general oncological caution — apply. A specific PEGylation concern in some pharmaceutical contexts is anti-PEG antibody formation — the immune system can mount an antibody response to the PEG chain after repeated exposure, which can reduce the compound's efficacy over time and in rare cases cause hypersensitivity reactions. This is a documented phenomenon with PEGylated pharmaceutical drugs and is a relevant consideration for PEG-MGF as well. Long-term human safety data does not exist.
People with active cancer or a history of cancer should not use it given the cell proliferation mechanism. Competitive athletes are prohibited from use under WADA — both MGF and PEG-MGF are listed under prohibited growth factors. Pregnant or breastfeeding women should not use it. People with a history of hypersensitivity reactions to PEGylated compounds should exercise particular caution given the anti-PEG antibody concern. The same fundamental caveat as standard MGF applies — the mechanistic basis for its claimed effects in humans remains scientifically contested in the published literature, and anyone considering it should understand they are operating beyond the established evidence base.





