


TB 500
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
TB-500: A Synthetic Fragment of Thymosin Beta-4 for the Study of Tissue Regeneration
TB-500 is a synthetic fragment of the natural protein thymosin beta-4, which plays a key role in the process of wound healing and tissue regeneration. This peptide is actively investigated for its capacity to accelerate wound healing, improve cellular migration, and reduce inflammation.
In preclinical models, TB-500 demonstrates positive results in the healing of skin wounds, the improvement of cardiac regeneration following myocardial infarction, and the stimulation of new blood vessel growth. However, clinical data in humans remain limited, and studies conducted with its involvement have not yet confirmed its efficacy at the human level.
It is important to bear in mind that TB-500 lacks official approval for use in humans and is prohibited in sport — facts that underscore the necessity of caution in its application.
TB-500 (Thymosin Beta-4 Fragment): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
TB-500 is arguably the compound in this series with the largest gap between its community reputation and its actual evidence base. It is one of the most widely discussed peptides in the athletic recovery and biohacking market, credited with healing tendons, muscles, and joints with remarkable speed. The pharmacological rationale is not absurd — it derives from a genuinely important endogenous protein with well-documented roles in wound healing. But the claim that injectable TB-500 produces these benefits in humans is substantially ahead of the available clinical evidence.
TB-500 is a synthetic version of a 7-amino acid fragment (residues 17-23) of thymosin beta-4 (Tβ4), a naturally occurring 43-amino acid protein found in virtually all human cells except red blood cells. Tβ4 is a critical regulator of actin dynamics — it sequesters monomeric G-actin, controlling the pool available for polymerisation into actin filaments. This regulation of cytoskeletal dynamics underpins cell migration, essential for wound healing and tissue remodelling.
⚠️ The human clinical evidence for the Tβ4/TB-500 class includes Phase 2 trials in venous stasis ulcers (N=73) and dry eye. These trials used full-length Tβ4, not the TB-500 fragment. TB-500 itself has no published direct human clinical trial data.[9]
| At a glance | |
|---|---|
| TB-500 sequence | Ac-Lys-Lys-Thr-Glu-Thr-Gln (Ac-LKKTETQ); amino acids 17–23 of Tβ4 |
| N-terminal modification | N-terminal acetylation (Ac-) |
| Parent protein | Thymosin beta-4 (Tβ4): full 43-amino acid endogenous protein |
| Molecular weight (TB-500) | ~799 Da |
| Natural occurrence | TB-500 (the specific fragment) does not occur naturally; Tβ4 does |
| Primary mechanism | G-actin sequestration → regulates actin polymerisation → facilitates cell migration |
| FDA status | ⚠️ Not approved; Category 2 (2023) — prohibited for compounding |
| WADA status | ❌ Prohibited at all times — S2, non-specified substance (standard 4-year ban) |
The Parent Protein: Thymosin Beta-4 (Tβ4)
Thymosin beta-4 was first purified from bovine thymus in 1981 (Low et al., PNAS). Despite the name, it is not thymus-specific — Tβ4 is the most abundant intracellular protein in most mammalian cells, present in high concentrations in all tissue types except erythrocytes, with highest levels in platelets, leukocytes, plasma, and wound fluid.
Tβ4 is a 43-amino acid protein with three functional domains: an N-terminal domain (residues 1-4); a central actin-binding domain (residues ~17-26, the LKKTETQ sequence that TB-500 replicates); and a C-terminal domain (residues ~28-43) contributing secondary functions. Tβ4 is highly evolutionarily conserved — the protein sequence is essentially identical across mammals, suggesting fundamental biological importance.
Primary functions: G-actin sequestration (binds monomeric G-actin with high affinity ~0.5 µM, creating a regulated pool for rapid cytoskeletal remodelling); cell migration facilitation (rate-limiting factor for migration speed of keratinocytes, fibroblasts, endothelial cells, and cardiac progenitor cells); integrin-linked kinase (ILK) activation (activates downstream Akt signalling promoting cell survival and proliferation); angiogenesis promotion; anti-inflammatory cytokine downregulation; and cardiac development and regeneration. External administration of Tβ4 promotes cardiac cell migration and survival, and systemic injection is capable of transforming the adult epicardium to an embryonically active state at uninjured areas of the heart.[5]
TB-500: The Synthetic Fragment
TB-500 is a synthetic 7-amino acid fragment corresponding to residues 17-23 of Tβ4, with an N-terminal acetylation modification: N-Acetyl-Lys-Lys-Thr-Glu-Thr-Gln (Ac-LKKTETQ). This fragment spans the core actin-binding domain of Tβ4. The N-terminal acetylation protects the N-terminus from aminopeptidase degradation, mimics the constitutive post-translational modification state of Tβ4 in cells, and enhances biological activity relative to the non-acetylated fragment.
TB-500 vs. Tβ4: the distinction matters
| Feature | Thymosin Beta-4 (Tβ4) | TB-500 |
|---|---|---|
| Length | 43 amino acids | 7 amino acids |
| Origin | Endogenous (all cells) | Synthetic fragment |
| Natural occurrence | Yes | No — the specific fragment is synthetic |
| ILK activation | Yes (full protein) | Limited/partial |
| Cardiac progenitor effects | Documented | Not specifically documented |
| Human Phase 2 trials | ✅ Yes (wound healing, dry eye) | ❌ No direct human trials |
Nearly all published human clinical research used full-length Tβ4, not TB-500. Community claims that cite Tβ4 human trial evidence as support for TB-500 are conflating two distinct molecules.
Mechanism of Action
G-actin sequestration and cell migration
TB-500 (Ac-LKKTETQ) binds monomeric G-actin through electrostatic interactions (the Lys-Lys residues) and hydrophobic contacts at the actin-binding groove, preventing spontaneous nucleation or elongation of actin filaments (F-actin). The sequestered G-actin creates a reservoir of readily mobilisable actin. When cells receive migration signals (growth factors, injury cues), actin rapidly polymerises from this pool, enabling fast lamellipodia extension and directional migration. This enhances wound healing through faster re-epithelialisation (keratinocytes), connective tissue repair (fibroblasts), and angiogenesis (endothelial cells). Additional mechanisms include upregulation of matrix metalloproteinases that degrade damaged extracellular matrix and zyxin upregulation enhancing cytoskeleton organisation.
The active metabolite question (2024 finding)
⚠️ A 2024 study in Journal of Chromatography B (Rahaman et al.) found that TB-500 is rapidly metabolised in vivo to Ac-LKKTE (the pentapeptide minus the C-terminal glutamine), and that the wound healing activity in vitro was attributable to this metabolite rather than the parent TB-500 compound.[8] If wound healing activity resides in the Ac-LKKTE metabolite, then TB-500 functions as a prodrug. This has implications for dosing calculations, stability requirements, and possibly direct use of Ac-LKKTE. The finding is preliminary and needs replication.
Preclinical Evidence
Dermal wound healing (Malinda et al., Journal of Investigative Dermatology, 1999): The seminal wound healing paper. Addition of Tβ4 topically or intraperitoneally increased re-epithelialisation by 42% over saline controls at 4 days and by as much as 61% at 7 days post-wounding. Treated wounds contracted at least 11% more than controls by day 7. Increased collagen deposition and angiogenesis were observed. Tβ4 stimulated keratinocyte migration 2–3 fold in Boyden chamber assays.[1]
Diabetic and aged wound healing (Philp et al., 2003): Tβ4 accelerated healing in db/db diabetic mice and aged mice — both of which have severely impaired wound healing — with both topical and systemic Tβ4.[2] Cardiac regeneration (Bock-Marquette et al., Nature, 2004): Tβ4 activates ILK in cardiomyocytes, promoting cardiac cell migration and survival, and reduced cardiomyocyte death following myocardial infarction in mice.[5] Hair growth (Philp et al., FASEB Journal, 2004): Tβ4 activates hair follicle stem cells, increasing hair growth — one of the more robustly documented preclinical effects. Multiple preclinical studies also show improved tendon healing and neurological recovery in animal models.
Human Clinical Evidence
Venous stasis ulcers (Phase 2, N=73): A European double-blind, placebo-controlled study found that 0.03% topical Tβ4 led to complete healing in approximately 25% of patients within 3 months, typically in small to moderate venous stasis ulcers. In pressure and stasis ulcers, Tβ4 accelerated healing by nearly one month in some patients, but overall healing rates were not conclusively superior to control. Both studies had significant methodological constraints and small sample sizes.[9]
Dry eye syndrome: A 9-patient study using Tβ4 eye drops found 35% reduction in eye discomfort, 59% improvement in dry eye testing parameters, and increased tear production after 56 days.[3] Cardiac progenitor cells (Zhu et al., 2016): 26 patients with STEMI received autologous endothelial progenitor cells pre-treated with Tβ4 before transplantation ex vivo; safety confirmed, outcomes preliminary.[10]
| Trial | N | Molecule | Finding |
|---|---|---|---|
| Venous stasis ulcers (Phase 2) [9] | 73 | Full Tβ4 | ~25% complete healing at 3 months; mixed primary endpoint |
| Dry eye [3] | 9 | Full Tβ4 | Positive signal; insufficient to establish efficacy |
| Cardiac progenitor cells [10] | 26 | Ex vivo Tβ4 | Safety confirmed; preliminary efficacy |
| TB-500 direct human trials | 0 | TB-500 fragment | ❌ None published |
Regulatory Status
⚠️ FDA (Category 2, 2023): TB-500 is prohibited for compounding by licensed 503A and 503B pharmacies. The FDA determined there is insufficient evidence of safety and efficacy to permit its compounding under the interim policy framework. As of April 2026, TB-500’s Category 2 status has not been reversed.[12]
⚠️ WADA (prohibited at all times, non-specified substance): TB-500 and related derivatives including thymosin beta-4 are prohibited at all times for athletes as non-Specified Substances. A non-specified substance classification means no exceptional circumstances defence is available and the standard 4-year sanction applies. A Canadian Centre for Ethics in Sport case sanctioned an athlete for using BPC-157 and TB-500 with a four-year ineligibility period.[11]
Equine doping history: TB-500 gained its initial public profile through use in thoroughbred horse racing in Australia in the early 2010s. Racing authorities developed LC-MS/MS detection methods (Ho et al., Journal of Chromatography A, 2012), and the compound was banned from equine competition before WADA’s human athlete listing.[7] US Department of Defense: Formally adopted WADA Prohibited List categories S0–S5, prohibiting TB-500 for military personnel.
Safety Profile
TB-500’s safety profile in human clinical research is primarily derived from full-length Tβ4 trials: acceptable safety profile; well-tolerated topically and intravenously; no serious adverse events attributed to Tβ4 in clinical trial populations. The most common community-reported adverse event is mild injection site reactions.
⚠️ What is not known: Long-term safety of repeated subcutaneous TB-500 injection in humans (no formal study); systemic pharmacokinetics after SC injection in humans (not formally characterised); drug-drug interactions (not studied); and safety in patients with active malignancy. Theoretical cancer concern: Tβ4’s cell migration enhancement could theoretically promote tumour invasion/metastasis at supraphysiological concentrations; not clinically studied. The endogenous ubiquity of Tβ4 provides some reassurance, but administering supraphysiological concentrations is pharmacological intervention with unstudied consequences.
Common Misconceptions
“TB-500 is natural because Tβ4 is in my body.”
TB-500 is the synthetic 7-amino acid fragment Ac-LKKTETQ — it does not naturally occur. Tβ4 is endogenous; TB-500 is synthetic. Administering supraphysiological concentrations of any molecule that normally operates at physiological concentrations is pharmacological intervention, not “natural” support.
“The Tβ4 human trials prove TB-500 works.”
⚠️ The Phase 2 trials used full-length Tβ4 (43 amino acids), not TB-500 (7 amino acids). These are different molecules with partly overlapping but not identical biological activities. Evidence for one is not directly transferable to the other. TB-500 has no published direct human clinical trial data.
“TB-500 repairs tendons and ligaments faster than anything else.”
This claim derives from preclinical animal data and community anecdote. No controlled human study has demonstrated superior tendon or ligament repair with TB-500 compared to standard of care or any comparator. The preclinical data is real; the extrapolation to human tendons at community doses is speculative.
Frequently Asked Questions
Is there a meaningful difference between TB-500 and Tβ4?
Probably yes. Full-length Tβ4 has activities beyond actin sequestration — particularly ILK activation, cardiac progenitor effects, and immunomodulatory effects that require structural domains not present in the 7-amino acid fragment. TB-500 is essentially a selective actin-sequestering fragment. Whether this fragment is sufficient to produce the full wound-healing and tissue-repair profile of the intact protein is not established.
What is the significance of the 2024 active metabolite finding?
If wound healing activity resides in the Ac-LKKTE metabolite (Rahaman et al., 2024), then TB-500 is a prodrug for this smaller pentapeptide. This has implications for dosing (you need enough TB-500 to generate sufficient Ac-LKKTE) and possibly for direct use of Ac-LKKTE instead of TB-500. The finding is preliminary and needs replication.[8]
Why does the community typically combine TB-500 with BPC-157?
BPC-157 (pentadecapeptide from gastric juice) and TB-500 have partially complementary proposed mechanisms — BPC-157 primarily through tendon-specific fibroblast growth factor upregulation and NO pathway activation; TB-500 through actin dynamics and cell migration. The evidence for the combination is no stronger than for either compound individually in humans.
Key Takeaways
- TB-500 is a synthetic fragment of a genuinely important endogenous protein. Tβ4 is a real, biologically critical molecule with well-established roles in wound healing, actin regulation, and tissue repair. The pharmacological rationale is not fabricated.[1]
- ⚠️ The evidence base is almost entirely preclinical. The compelling wound healing data from rodent models, the keratinocyte migration studies, the cardiac regeneration data — all are animal or in vitro findings. The human clinical data used full-length Tβ4, not TB-500.
- ⚠️ TB-500 itself has no published direct human clinical trials. Everything claimed for TB-500 in humans is extrapolated from Tβ4 research or derived from anecdote.
- ⚠️ The regulatory and anti-doping consequences are among the most serious in this series. Category 2 (FDA, no compounding permitted) + WADA non-specified substance (4-year ban standard) + US DoD prohibition. For any athlete or military-affiliated individual, the consequences of TB-500 use are severe.[11][12]
- The 2024 active metabolite finding raises questions about what actually produces TB-500’s effects. If Ac-LKKTE is the biologically active species, community dosing protocols built around TB-500 amounts may need reconsideration.[8]
References
Foundational Tβ4 Biology
- Malinda KM, Sidhu GS, Mani H, et al. Thymosin β4 accelerates wound healing. Journal of Investigative Dermatology. 1999;113(3):364–368. PMID 10469335
- Philp D, Badamchian M, Scheremeta B, et al. Thymosin β4 and a synthetic peptide containing its actin-binding domain promote dermal wound repair in db/db diabetic mice and in aged mice. Wound Repair and Regeneration. 2003;11(1):19–24.
- Sosne G, Qiu P, Kurpakus-Wheater M. Thymosin beta-4: a novel corneal wound healing and anti-inflammatory agent. Clinical Ophthalmology. 2007;1(3):201–207. PMC2701135
- Goldstein AL, Hannappel E, Sosne G, Kleinman HK. Thymosin β4: a multi-functional regenerative peptide. Basic properties and clinical applications. Expert Opinion on Biological Therapy. 2012;12(1):37–51.
Cardiac Biology
- Bock-Marquette I, Saxena A, White MD, DiMaio JM, Srivastava D. Thymosin β4 activates integrin-linked kinase and promotes cardiac cell migration, survival and cardiac repair. Nature. 2004;432:466–472.
- Maar K, Hetenyi R, Maar S, et al. Utilising developmentally essential secreted peptides such as thymosin beta-4 to remind the adult organs of their embryonic state. Cells. 2021;10(6):1343. PMC8228050
TB-500 Specific (Veterinary/Doping)
- Ho EN, Kwok WH, Lau MY, et al. Doping control analysis of TB-500, a synthetic version of an active region of thymosin β4, in equine urine and plasma by liquid chromatography–mass spectrometry. Journal of Chromatography A. 2012;1265:57–69.
- Rahaman KA, et al. Simultaneous quantification of TB-500 and its metabolites in in-vitro experiments and rats by UHPLC-Q-Exactive orbitrap MS/MS and their screening by wound healing activities in-vitro. Journal of Chromatography B. 2024;1235:124033.
Human Clinical Data
- Venous stasis ulcer Phase 2 trial (N=73): 0.03% topical Tβ4; European multicentre. Referenced in multiple reviews.
- Zhu J, Song J, Yu L, et al. Safety and efficacy of autologous thymosin β4 pre-treated endothelial progenitor cell transplantation in patients with acute ST-segment elevation myocardial infarction: a pilot study. Cytotherapy. 2016;18(8):1037–1042.
Regulatory
- WADA Prohibited List 2025. S2: Peptide hormones, growth factors, related substances and mimetics. wada-ama.org
- FDA Category 2 bulk drug substances interim policy: TB-500 designation 2023.
Key Investigators
- Allan L. Goldstein, PhD — George Washington University; co-discoverer and primary champion of the thymosin peptide family; laboratory characterised thymosin beta-4’s structure and biological activities throughout the 1980s–2010s.
- Hynda K. Kleinman, PhD — National Institutes of Health (NIDCR); co-developer of much of the wound healing evidence base for Tβ4.
- Gabriel Sosne, PhD, MD — Wayne State University (Ophthalmology); developed the corneal application of Tβ4; ran the dry eye clinical studies.
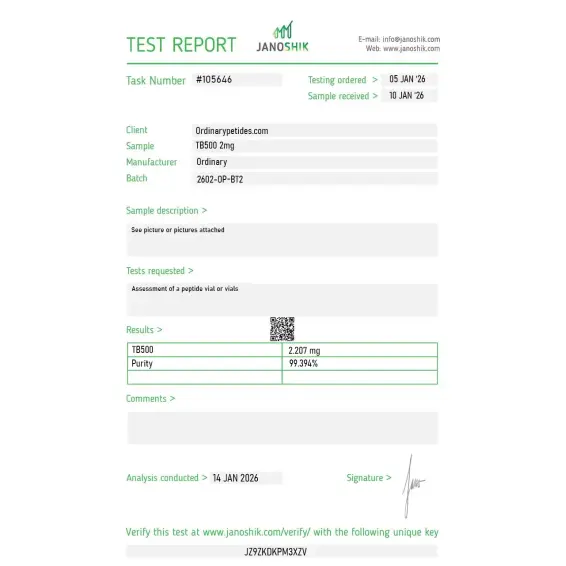
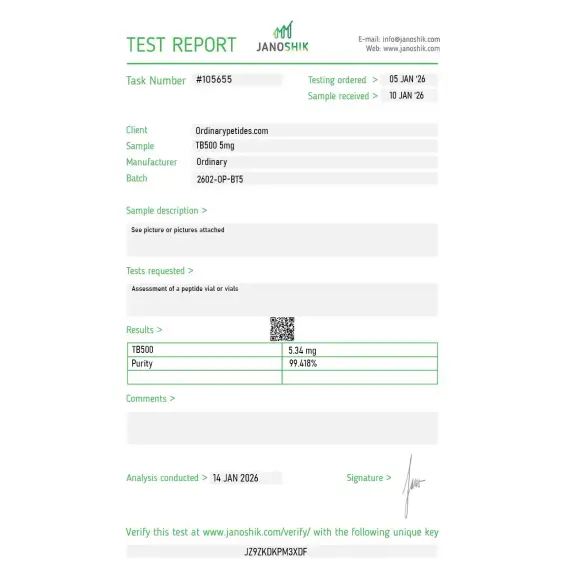
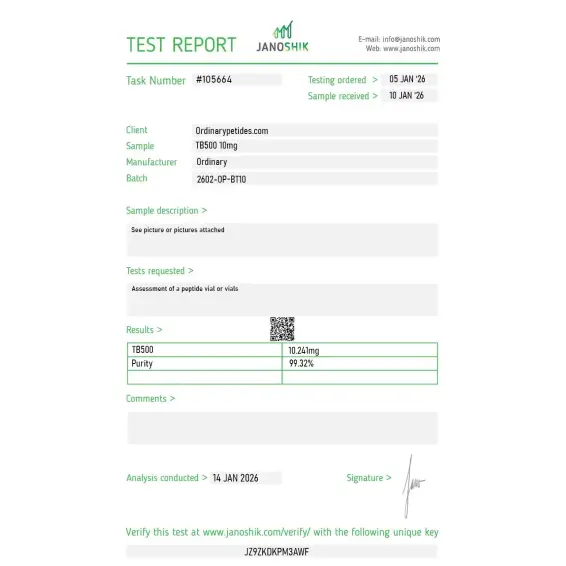
Certificate of Analysis
Independent test reports are available for TB-500 2mg, 5mg, and 10mg. These reports provide batch-level documentation and analytical verification information for research reference.
Reorder.
The supplier ships in glass vials, which is fine for storage but creates a small practical problem — Tβ4 adsorbs measurably to glass at low concentrations during reconstitution, more than polypropylene would, and we ended up doing a glass-to-low-bind-tube transfer immediately after reconstitution. Not unique to this vendor, but a note about glass-adsorption-at-trace-concentrations on the listing would help newer researchers. Material itself was fine once handled correctly.
We use Tβ4 in zebrafish regeneration model work — characterizing how exogenous thymosin β-4 modulates fin regeneration kinetics in live embryos, which is a different application from the mammalian cell culture most catalog descriptions emphasize. The vertebrate-regeneration model is a substantial separate research thread. Material gave consistent uptake and downstream effects across our embryo treatment cohorts.
What surprised me positively was the lyophilization quality — Tβ4 at 43 residues with multiple polar residues can lyophilize to a fluffy mass that's hard to fully recover from a vial, but this material was lyophilized to a tighter cake that came out cleanly with bacteriostatic water. That handling reality matters for accurate concentration when you're measuring out single-use aliquots, and the freeze-drying process here was clearly optimized rather than generic.
Tβ4 is a natural peptide of 43 amino acids. TB-500 is a synthetic fragment of 7 amino acids. The activity of the fragment may not fully reproduce the effects of the full-length protein.
Clinical data on the use of TB-500 for recovery after injury are absent. Its efficacy requires further research. Data on the use of TB-500 for recovery after injury in humans are absent, and any claims regarding its efficacy in this context are based on limited or anecdotal evidence.
Yes. Thymosin-β4 and its derivatives are included on the WADA Prohibited List under the category of growth factors, as confirmed by official regulatory sources. The prohibition applies year-round.
For the full-length form of Tβ4, mild reactions at the site of administration were most frequently noted in clinical studies. For the fragment TB-500, no controlled safety data exist; theoretical risks include immune reactions and unpredictable systemic effects.
At present, there are no legal pathways for the medical use of this compound outside official clinical trials. Peptides sold with the label "for research purposes" lack official approval for medical use.
As of the preparation of this material (2026), no controlled studies on the efficacy of TB-500 for muscle recovery in humans are registered in public clinical trial databases. Data have been obtained exclusively in preclinical models using the full-length form of Tβ4.
The full-length form of thymosin beta-4 has shown signals of efficacy in accelerating wound healing in preclinical studies and small clinical samples. For the fragment TB-500, comparable data are absent.
Since clinical studies on the efficacy of TB-500 in humans have not been conducted, reliable data on the timing of effects do not exist.
Data on peptide interactions in humans are absent. Without clinical research, such combinations cannot be recommended.
Data on the long-term safety of TB-500 are absent. Theoretical risks with prolonged use include antibody production and unpredictable immune reactions.
For specific conditions (wounds, injuries, inflammatory processes), methods with proven efficacy exist:
- Physiotherapy: ultrasound, laser therapy, electrical stimulation—confirmed methods for accelerating healing;
- Nutritional support: adequate intake of protein, vitamin C, zinc—essential nutrients for tissue recovery;
- Pharmacotherapy as prescribed by a physician: topical antiseptics, anti-inflammatory agents;
- Rehabilitation programmes: graded exercise, kinesiotherapy—a proven approach to functional recovery.
Discuss options suitable for your specific situation with a qualified specialist.
The topic's popularity is linked to growing interest in peptide therapy and activity within biohacker communities. However, popularity ≠ proven efficacy.
TB-500 is the research and commercial name for the synthetic peptide fragment corresponding to amino acids 17 through 23 of Thymosin Beta-4 (Tβ4) — a naturally occurring 43-amino acid protein found in virtually every nucleated cell in the human body and present at high concentrations in platelets, wound fluid, and regenerating tissue. TB-500's active sequence is Ac-LKKTETQ, derived from the actin-binding domain of the full Tβ4 molecule. Thymosin Beta-4 was first identified in the thymus — hence its original classification — but is now understood to be ubiquitously expressed and to function primarily as a G-actin sequestering protein critical to cytoskeletal dynamics and cell migration. TB-500 as a synthetic fragment was developed to isolate and concentrate the regenerative, anti-inflammatory, and tissue-repair properties of the full Tβ4 molecule in a shorter, more stable, and more economical form. It is not FDA-approved for any therapeutic indication, is classified as an FDA Category 2 bulk drug substance meaning it cannot be legally compounded in the United States, and is banned by WADA under the S0 non-approved substances category.
TB-500's primary mechanism centers on actin regulation and cell motility. G-actin is the monomeric form of actin — the structural protein that polymerizes into filaments governing cell shape, movement, and division. TB-500 binds to G-actin through the same domain as the full Tβ4 molecule, sequestering actin monomers and regulating the dynamic equilibrium between globular and filamentous actin at the leading edges of migrating cells. This actin sequestration drives several downstream effects simultaneously. It promotes cell migration — particularly of endothelial cells, keratinocytes, and fibroblasts — toward sites of injury, accelerating the cellular infiltration phase of tissue repair. It upregulates matrix metalloproteinases that remodel extracellular matrix during healing. It promotes angiogenesis — the growth of new blood vessels — through upregulation of VEGF and other angiogenic signals, restoring vascular supply to damaged tissue. It modulates inflammatory signaling, reducing pro-inflammatory cytokine production and shifting the immune environment toward resolution and repair. It has been shown to activate progenitor and stem cell populations in multiple tissue types. In cardiac models specifically, the full Tβ4 molecule has documented ability to reactivate quiescent cardiac progenitor cells — a finding of substantial interest given the heart's notoriously limited regenerative capacity.
The TB-500 versus BPC-157 distinction was covered in the duo entry but deserves direct comparison here. BPC-157 is a gastric pentadecapeptide fragment with its primary mechanism through the NO-cGMP pathway, VEGFR2 activation, and growth factor receptor upregulation — it is particularly associated with tendon, ligament, and gut healing and has been studied in animal models of a wide range of tissues. TB-500 acts through actin regulation and cell migration — it is particularly associated with muscle fiber repair, wound healing, cardiac protection, and conditions where cell motility is the rate-limiting step in recovery. Their mechanisms are complementary rather than overlapping, which is the scientific rationale for their frequent combined use as a healing stack. TB-500 is generally considered more systemic in its effects — its cell migration properties are not tissue-specific — while BPC-157's effects are more potent in the GI tract and tendon/ligament specifically.
The research base for Thymosin Beta-4 is substantially larger than for the synthetic TB-500 fragment specifically, with the full molecule studied in multiple Phase 1 and Phase 2 human clinical trials for cardiac repair and wound healing. For cardiac repair, intracoronary and intravenous Tβ4 administration in acute myocardial infarction patients has been evaluated in Phase 2 trials — results showed favorable safety profiles and signals of benefit in cardiac progenitor cell activation, though larger efficacy trials have not been completed. For wound healing in epidermolysis bullosa and dry eye disease, topical Tβ4 has shown efficacy signals in Phase 2 settings. The synthetic TB-500 fragment has been studied primarily in animal models — demonstrating accelerated muscle fiber repair and regeneration, improved healing of skin wounds, corneal repair, cardiac protection after ischemia, and anti-inflammatory activity in multiple tissue types.
TB-500 is given by subcutaneous or intramuscular injection — it is not orally bioavailable. Research and wellness protocols typically involve a loading phase of 4 to 8 mg per week divided across two injections for 4 to 6 weeks, followed by a maintenance phase of 2 to 4 mg biweekly or monthly. It is supplied as lyophilized powder reconstituted with bacteriostatic water. Its systemic distribution after injection is considered one of its advantages over more locally acting repair peptides — it can theoretically reach distant sites of injury following subcutaneous administration.
TB-500 has a generally favorable safety profile in available research — consistent with its endogenous origin as a fragment of a ubiquitously expressed protein. The most commonly reported effects are mild injection site reactions including pain, redness, and swelling. Transient fatigue and mild dizziness immediately following injection are occasionally reported. Temporary flushing has been noted. The primary theoretical safety concern is the same as with BPC-157 — its pro-angiogenic mechanism through VEGF upregulation raises a theoretical oncological concern, as tumor angiogenesis is a well-established mechanism of cancer progression. Whether physiological and supraphysiological systemic TB-500 administration provides meaningful pro-tumor stimulus in humans is not established, but it warrants the same precautionary approach applied to any compound that promotes angiogenesis.
People with active cancer or a history of cancer should not use it given the pro-angiogenic mechanism. Competitive athletes are prohibited from use under WADA's S0 non-approved substances ban. Pregnant or breastfeeding women should not use it. It cannot be legally compounded in the United States as an FDA Category 2 substance — any US-sourced TB-500 from a compounding pharmacy is operating outside the law, and products from research vendors carry no pharmaceutical quality assurance. Anyone considering TB-500 should understand that while the full Tβ4 molecule has genuine Phase 2 human clinical trial data, the synthetic TB-500 fragment's evidence base is predominantly animal research.





