


Peptide Duo BPC 157 / TB-500
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
BPC-157 + TB-500: A Promising Research Combination Behind the Hype
Peptide Duo BPC-157 / TB-500 is better understood not as a "magic recovery stack," but as an intriguing research combination whose reputation currently runs ahead of its clinical foundation. In the research context, BPC-157 draws attention because of its broad preclinical history, where it has been linked to tissue healing and vascular adaptation, while TB-500 is discussed as part of the thymosin beta-4 derivative line, associated with interest in cell migration and tissue plasticity. On paper, such a pairing looks elegant — one tied to a more local pro-healing narrative, the other to a more systemic recovery logic — and that is exactly why it remains so attractive in forums and among peptide-stack enthusiasts.
But the most interesting part here is the honesty of the story: there do not appear to be published high-quality studies specifically on the BPC-157 + TB-500 combination, and TB-500 itself is further complicated by frequent confusion with full-length thymosin beta-4. For a careful reader or client, that is not a disadvantage but a filter against myths: this is not a "finished solution," but an experimental idea with a strong research aura and weak clinical support. For those who are interested not in fairy tales but in compounds that genuinely deserve a closer look, this duo is compelling precisely because of its controversy, its context, and its unanswered questions.
BPC-157 / TB-500 Combination: A Scientific Review of the “Wolverine Stack”
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
BPC-157 and TB-500 are two of the most widely discussed research peptides in the sports medicine, biohacking, and regenerative wellness world. Their combination — often marketed as the “Wolverine Stack” — has become one of the most popular peptide protocols in use outside of formal clinical settings.
The premise sounds logical: BPC-157 and TB-500 have different but potentially complementary mechanisms in tissue repair. BPC-157 focuses primarily on local healing, angiogenesis, and gut cytoprotection; TB-500 works systemically through actin regulation and cell migration. Stacking them together might, in theory, cover more of the healing cascade than either compound alone. The problem is that this premise is built almost entirely on animal data for each compound separately, theoretical synergy reasoning, and anecdotal reports — not on controlled human trials, and certainly not on controlled human trials of the combination.
| At a glance — BPC-157 | |
|---|---|
| Full name | Body Protection Compound 157 |
| Sequence | GEPPPGKPADDAGLV (15 amino acids) |
| Origin | Derived from human gastric juice protein |
| Mechanism | VEGF/eNOS/NO signalling; GH receptor upregulation; FAK-paxillin; no known receptor |
| FDA status | Category 2 — cannot be compounded; 2023 |
| WADA status | Prohibited (S2 category) |
| Human trial data | Fewer than 30 people across 3 non-randomised pilot reports |
| At a glance — TB-500 | |
|---|---|
| Full name | TB-500 (synthetic Ac-LKKTETQ fragment of thymosin beta-4) |
| Sequence | Ac-Leu-Lys-Lys-Thr-Glu-Thr-Gln (7 amino acids, acetylated) |
| Parent molecule | Thymosin beta-4 (Tβ4) — naturally occurring 43-amino acid peptide |
| Mechanism | Actin sequestration; cell migration; angiogenesis; Notch signalling |
| FDA status | Not approved; not on compounding lists; research chemical only |
| WADA status | Prohibited (S2 and S0) — non-Specified Substance |
| Human trial data | Essentially none for TB-500 specifically; limited for parent Tβ4 |
| At a glance — Combination | |
|---|---|
| Popular name | “Wolverine Stack” |
| Human combination trial data | None published |
| Synergy claim basis | Theoretical complementary mechanisms from separate animal studies |
| Regulatory status | Both prohibited; BPC-157 cannot be compounded; no approved combination product exists |
Part 1 — BPC-157
What It Is
BPC-157 (Body Protection Compound 157) is a synthetic 15-amino acid pentadecapeptide derived from a sequence found in human gastric juice protein. It was first described in the early 1990s by Predrag Sikiric and colleagues at the University of Zagreb Medical School, where the vast majority of BPC-157 research has since originated. The peptide is notable for its stability in gastric acid — unusual for a peptide of its size — which allows oral activity in animal models. It has no identified endogenous receptor, which makes its mechanism harder to characterise systematically.
Mechanism of Action
VEGF / angiogenesis: BPC-157 upregulates VEGFR2 and stimulates angiogenesis at injury sites in early post-injury periods, then allows the response to resolve — consistent with coordinated tissue repair rather than chronic neovascularisation.[5]
Nitric oxide system: BPC-157 activates the VEGFR2-Akt-eNOS signalling pathway and the Src-Caveolin-1-eNOS pathway, promoting NO production, vasodilation, and vascular healing.
FAK-paxillin pathway: BPC-157 has been linked to activation of focal adhesion kinase (FAK) — paxillin signalling, which drives cell migration and extracellular matrix reorganisation.
Growth hormone receptor upregulation: Independent research from Taiwan (Chang et al.) showed that BPC-157 upregulates growth hormone receptor expression in tendon fibroblasts, potentially linking its tissue-healing effects to the GH-IGF-1 axis.
ERK1/2 and Egr-1 activation: These pathways are involved in wound healing, collagen synthesis, and cell proliferation.
Preclinical Evidence
The breadth of BPC-157’s preclinical data is substantial — and the concentration of that data in one research group is a genuine limitation. Over 80% of more than 190 published papers list Predrag Sikiric as first or senior author. Independent replication exists but is uneven.[1]
| Application | Independent replication | Confidence level |
|---|---|---|
| Gastrointestinal protection (ulcers, colitis) | Some independent work | Moderate |
| Tendon healing (Achilles, quadriceps) | Partial — Chang group, Taiwan | Moderate |
| Muscle healing | Largely Zagreb group | Low-moderate |
| Bone / ligament healing | Largely Zagreb group | Low |
| CNS / neuroprotection | Almost entirely Zagreb group | Low |
| Cardiovascular protection | Largely Zagreb group | Low |
Human Evidence for BPC-157
Of 544 articles from 1993 to 2024, after duplicates were removed, 36 studies were included in a systematic review — 35 preclinical studies and 1 clinical study.[1] Beyond that, there are two additional small human reports: a pilot study in 12 interstitial cystitis patients,[3] and an IV safety study in 2 healthy adults.[4] A formal Phase I trial in 42 volunteers initiated in 2015 was never published. Total documented human exposure across all published reports: fewer than 30 people. No randomised controlled trial has been conducted.
Regulatory Status — BPC-157
BPC-157 was placed on the FDA’s Category 2 bulk drug substance list in 2023, citing “significant safety concerns.”[7] This prevents US compounding pharmacies from legally preparing it. It is also prohibited by WADA (S2 — Peptide Hormones, Growth Factors, and Related Substances)[13] and was the subject of a real-world anti-doping sanction: a Canadian athlete received a four-year ban in part for TB-500 and BPC-157 use under the 2024 WADA Prohibited List.
Part 2 — TB-500
What It Is — and What It Isn’t
This distinction matters enormously and is consistently blurred in popular coverage.
Thymosin beta-4 (Tβ4): A naturally occurring 43-amino acid peptide present in virtually all human tissues, with highest concentrations in platelets, white blood cells, plasma, and wound fluid. It plays a fundamental role in actin dynamics, cell migration, wound healing, and tissue repair.[10]
TB-500: A synthetic heptapeptide (Ac-LKKTETQ) that corresponds to amino acids 17–23 of thymosin beta-4 — the region responsible for actin binding. TB-500 is a short synthetic fragment, not the full Tβ4 protein. A fragment does not automatically have the same effects or safety profile as the whole. A 2024 study suggested that TB-500 may not even be the primary active form — its healing activity might derive from metabolites produced during degradation.[11]
Mechanism of Action
Actin sequestration (primary mechanism): Thymosin beta-4 is the cell’s primary G-actin sequestration protein. It binds G-actin in a 1:1 ratio, preventing spontaneous polymerisation into F-actin filaments. By regulating the available G-actin pool, it controls cytoskeletal dynamics — essential for cell migration, lamellipodia formation, and wound healing. TB-500 is designed to replicate this activity via the LKKTETQ actin-binding domain.[8]
Cell migration: By modulating actin dynamics, TB-500 facilitates the movement of fibroblasts, endothelial cells, and progenitor cells to sites of injury.
Angiogenesis: TB-500 promotes new blood vessel formation, likely through the Notch signalling pathway.
Anti-inflammatory and anti-fibrotic effects: Reduction of inflammatory cytokines at injury sites; thymosin beta-4 has been shown to prevent myofibroblast differentiation, potentially reducing scar formation.[9]
Preclinical Evidence
Research on thymosin beta-4 specifically (not TB-500 as a fragment) is more diverse and independently replicated than BPC-157 research, particularly for cardiac and wound healing applications. The most clinically advanced application is the RGN-259 ophthalmic formulation for dry eye disease, which progressed to Phase 2/3 trials — the most advanced human development of any thymosin beta-4 preparation, though the ophthalmic route differs substantially from systemic injection.[9]
Human Evidence for TB-500
There are zero human clinical trials on TB-500 specifically. Its safety in humans is completely unknown. For the parent Tβ4, limited human data exists: a randomised, placebo-controlled, single and multiple dose study of intravenous thymosin beta-4 in healthy volunteers established a reasonable short-term safety profile. A Phase 2 trial in cardiac patients was completed but never published — a troubling parallel to the BPC-157 situation.
Regulatory Status — TB-500
TB-500 is not FDA-approved. Unlike BPC-157, it has not been specifically placed on a Category 2 compounding restriction list — primarily because it was never widely used in compounding pharmacies to begin with, having circulated mainly as a research chemical. TB-500 is prohibited at all times under WADA’s prohibited list as a non-Specified Substance.[13] The non-Specified classification means no Therapeutic Use Exemption (TUE) is available — sanctions for detected use are typically the maximum four-year ban.
Part 3 — The Combination: What Is and Isn’t Known
The Mechanistic Rationale (What Makes It Plausible)
The argument for combining BPC-157 and TB-500 is based on complementary biology. The two compounds operate through distinct primary mechanisms:
| Mechanism | BPC-157 | TB-500 | Combined hypothesis |
|---|---|---|---|
| Angiogenesis | Via VEGF/VEGFR2 upregulation | Via Notch signalling pathway | Dual pathway = more robust vascular response |
| Cell migration | Via FAK-paxillin signalling | Via actin sequestration / G-actin regulation | Complementary — different entry points to same process |
| Anti-inflammatory | Via NO system and cytokine modulation | Via Tβ4-related cytokine suppression | Potentially additive |
| Collagen synthesis / fibroblast activity | Via GH receptor upregulation | Via actin-driven cell migration recruiting fibroblasts | Different rate-limiting steps |
| Healing cascade phase | Promotes local repair and growth factor response | Promotes systemic cell recruitment and migration | Theoretically covers more of the healing timeline |
What “Synergy” Actually Requires to Be Proven
The word “synergy” has a specific scientific meaning: a combined effect greater than the sum of individual effects, not just additive effects, and certainly not just “complementary mechanisms.” To establish synergy for this combination would require controlled animal studies with four arms (BPC-157 alone, TB-500 alone, combination, and placebo); predefined objective endpoints; statistical analysis confirming super-additive effects; independent replication; and eventually, human clinical trial data. None of these conditions have been met.
What Exists as Human Evidence for the Combination
One retrospective chart review — the Lee and Padgett 2021 knee injection study — included patients who received either BPC-157 alone or BPC-157 combined with thymosin beta-4.[2] This study cannot distinguish whether the combination performed differently from BPC-157 alone, as results were pooled across both treatment groups and the study had no control group, no standardised outcome measures, and no blinding. It is the only published human data involving the combination, and it provides no information about whether adding TB-500 to BPC-157 produces any benefit beyond BPC-157 alone.
What “Wolverine Stack” Marketing Claims vs. What the Evidence Shows
| Claim commonly made | What the evidence actually shows |
|---|---|
| “Synergistic healing acceleration” | No synergy has been demonstrated in controlled studies. Complementary mechanisms are plausible, not proven |
| “BPC-157 heals locally; TB-500 works systemically” | The local/systemic distinction is a reasonable framing of mechanistic differences, but has not been tested directly in combination protocols |
| “Used together they cover the entire healing cascade” | Mechanistically plausible; clinically unvalidated |
| “Faster and more complete recovery vs. either alone” | No comparative human data exists |
| “Proven in clinical studies” | False. Neither compound has published RCT data. The combination has no independent controlled trial data whatsoever |
| “Safe for regular use” | Safety profile in humans, individually or combined, is essentially undocumented for chronic use |
Safety Considerations for Both Compounds
BPC-157 Safety
In preclinical studies, BPC-157 has generally been well-tolerated. The primary published human reports (~30 people total) noted no adverse events. However, the cancelled 2015 Phase I trial (42 volunteers, results never published) is an unexplained gap; long-term safety, including tumour-related risks from chronic VEGF upregulation, has not been evaluated in controlled carcinogenicity studies; no drug interaction data exists; and products available outside supervised clinical settings are manufactured without pharmaceutical-grade quality controls.[7]
TB-500 Safety
No published human safety studies specifically for TB-500 exist. TB-500 is not approved by the FDA for medical use in humans.[12] The full Tβ4 protein has a reasonable short-term IV safety profile in small studies; whether the fragment shares this profile is assumed but not confirmed. Thymosin beta-4 plays a role in cell proliferation — similar theoretical cancer-related risks as with BPC-157 apply. Long-term effects are undocumented.
Safety Concerns Specific to the Combination
Additive or multiplicative VEGF upregulation: Both compounds promote angiogenesis through different pathways. Whether simultaneous activation results in uncontrolled neovascularisation or increased oncological risk is entirely unknown. Unknown pharmacokinetic interactions: whether the two compounds affect each other’s metabolism, distribution, or elimination has not been studied. Quality control of combination products: pre-blended commercial “Wolverine Stack” products available online are unregulated, and their actual peptide content, purity, and sterility cannot be assumed.
Regulatory and Legal Status Summary
| Compound | FDA | WADA | Compounding (US) | Research chemical |
|---|---|---|---|---|
| BPC-157 | Not approved; Category 2 (2023) [7] | Prohibited — S2 [13] | Cannot be legally compounded | Sold online; unregulated |
| TB-500 | Not approved | Prohibited — S2 / S0 (non-Specified) [13] | Not on compounding lists | Sold online; unregulated |
| BPC-157 + TB-500 combined | Not approved; same restrictions apply | Both prohibited | Same as BPC-157 alone | Sold online as blends; unregulated |
What Is Confirmed and What Remains Unknown
| Confirmed | Not established |
|---|---|
| BPC-157 and TB-500 have distinct primary mechanisms | Whether the combination produces superior outcomes vs. either alone |
| Both promote angiogenesis and tissue repair in animal models [5][8] | Safety of the combination in humans |
| Complementary mechanistic pathways exist (theoretically) | Whether “synergy” occurs in any pharmacological sense |
| Both are prohibited by WADA [13] | Long-term effects of either compound individually in humans |
| BPC-157 cannot be legally compounded in the US [7] | Optimal dosing, frequency, and duration for any application |
| TB-500 has no published human trial data [12] | Whether the combination increases oncological or other risks |
| BPC-157 has ~30 humans studied, no RCTs [1] | What the 2015 BPC-157 Phase I trial found |
Common Misconceptions About the Combination
“They’re natural compounds, so stacking them is safe.”
BPC-157 is synthetic. TB-500 is a synthetic fragment of a naturally occurring peptide. “Natural” does not equal safe, and “natural-derived” certainly does not mean the combination has been safety-tested.
“The synergy is well-established in research.”
It is not. Complementary mechanisms are proposed based on separate animal studies. No controlled experiment has directly tested the combination against single-compound arms in either animals or humans.
“Athletes use it, so it must work.”
Athlete use is driven by anecdotal reports, marketing, and the rational-sounding mechanistic narrative — not by clinical trial evidence. Athlete use also comes with a significant anti-doping risk. The combination is prohibited under WADA’s list,[13] and a real athlete received a four-year ban for using these exact compounds.
“Clinics prescribe it, so it’s been validated.”
Clinics prescribing or dispensing unapproved research chemicals operate outside the evidence-based standard of care. Prescription or availability through a clinic does not confer regulatory approval or clinical validation.
“Case reports prove it works.”
Anecdotal outcomes reflect many confounding variables: placebo effect, natural recovery, concurrent physical therapy, rest, nutrition, and publication of positive-only results. They are not proof of efficacy.
Frequently Asked Questions
Is combining BPC-157 and TB-500 legal?
Both are prohibited in competitive sport under WADA.[13] BPC-157 cannot be legally compounded by US pharmacies.[7] TB-500 is not on any approved drug or supplement list. Their combination has no approved status anywhere. Possession and personal use of research chemicals occupies a grey legal area in most jurisdictions, but use in sport is unambiguously prohibited.
Has the “Wolverine Stack” ever been tested in a clinical trial?
No. No published clinical trial has directly tested the combination. The only human data involving both compounds is a small, uncontrolled retrospective case series that pooled results across patients receiving either BPC-157 alone or BPC-157 plus TB4.[2]
Why do so many people report positive results?
Tissue injuries heal naturally. Peptide protocols are often combined with physical therapy, rest, nutrition, and other recovery strategies. Placebo effects are real and meaningful, especially for pain outcomes. None of this proves the compounds are ineffective — but it makes anecdotal reports unreliable as evidence.
What is the biggest scientific gap for this combination?
The complete absence of any controlled combination study, in animals or humans. Even a well-designed rodent study comparing BPC-157 alone, TB-500 alone, the combination, and placebo in a standardised injury model would represent a meaningful advance. That basic experiment has not been published.
Is there any ongoing research on the combination?
Not publicly registered in major clinical trial databases as of April 2026.
Key Takeaways
- The mechanistic rationale for combining BPC-157 and TB-500 is scientifically coherent — both compounds address tissue healing through different molecular entry points, and complementary mechanisms are a legitimate basis for hypothesis generation.
- The jump from “complementary mechanisms” to “proven synergy” is not supported by evidence. No controlled study — in animals or humans — has directly compared the combination versus individual compounds.
- Human evidence for each compound individually is extremely thin — fewer than 30 people for BPC-157,[1] essentially zero for TB-500 specifically. Human evidence for the combination is non-existent in any controlled sense.
- Both compounds are prohibited in competitive sport with meaningful sanctions.[13] A recent real-world case resulted in a four-year ban for use of this exact combination.
- BPC-157 cannot be legally compounded in the US.[7] Compounding pharmacies that offer it are operating outside the law.
- The “Wolverine Stack” narrative is primarily a marketing construct. The name, the framing, and the specific claims of superior synergistic healing are driven by commercial interest, biohacker culture, and anecdotal reporting — not by the weight of the scientific literature.
References
BPC-157
- Vasireddi N, Hahamyan H, Salata MJ, et al. Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review. American Journal of Sports Medicine. 2025. PMID: 40756949. PMC12313605
- Lee E, Padgett B. Intra-articular injection of BPC 157 for multiple types of knee pain. Alternative Therapies in Health and Medicine. 2021;27.
- Lee E, et al. Intravesicular BPC-157 for interstitial cystitis. Alternative Therapies in Health and Medicine. 2024.
- Lee E, Burgess S. Safety of Intravenous Infusion of BPC157 in Humans: A Pilot Study. Alternative Therapies in Health and Medicine. 2025. PMID: 40131143
- Brcic L, et al. Modulatory effect of gastric pentadecapeptide BPC 157 on angiogenesis in muscle and tendon healing. Journal of Physiology and Pharmacology. 2009;60(Suppl 7):191–196. PMID: 20388964
- Józwiak M, et al. Multifunctionality and Possible Medical Application of the BPC 157 Peptide. Pharmaceuticals. 2025;18(2):185.
- FDA. Certain Bulk Drug Substances for Use in Compounding that May Present Significant Safety Risks. Category 2 designation, 2023. fda.gov
TB-500 / Thymosin Beta-4
- Philp D, Badamchian M, Scheremeta B, et al. Thymosin beta 4 and a synthetic peptide containing its actin-binding domain promote dermal wound repair in db/db diabetic mice and in aged mice. Wound Repair and Regeneration. 2003;11(1):19–24.
- Goldstein AL, Hannappel E, Sosne G, Kleinman HK. Thymosin β4: a multi-functional regenerative peptide. Basic properties and clinical applications. Expert Opinion on Biological Therapy. 2012;12(1):37–51.
- Crockford D, Turjman N, Allan C, et al. Thymosin beta4: structure, function, and biological properties supporting current and future clinical applications. Annals of the New York Academy of Sciences. 2010;1194(1):179–189.
- TB-500 and metabolites study. Simultaneous quantification of TB-500 and its metabolites in in-vitro experiments and rats by UHPLC-Q-Exactive orbitrap MS/MS. ScienceDirect. 2024.
- BSCG. TB-500 — Status, Risks, and Bans in Sport and Military. bscg.org
Regulatory Sources
- WADA. Prohibited List — S2 and S0 categories (BPC-157 and TB-500). wada-ama.org
- USADA. BPC-157: Experimental Peptide Creates Risk for Athletes. usada.org
- FDA. 503A Bulk Drug Substances List — Category 2 designations. fda.gov
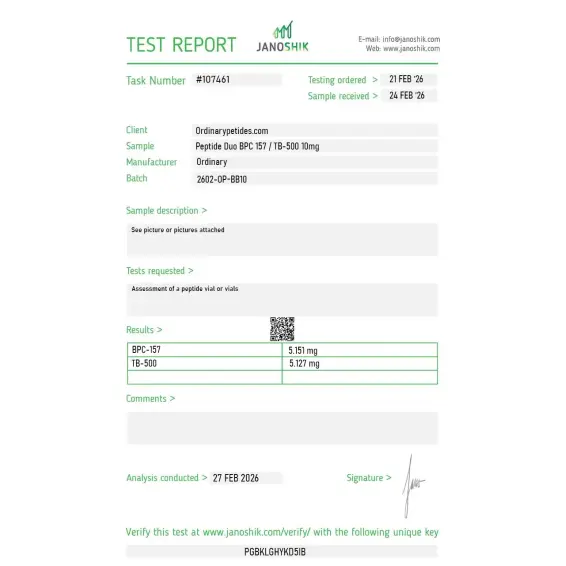
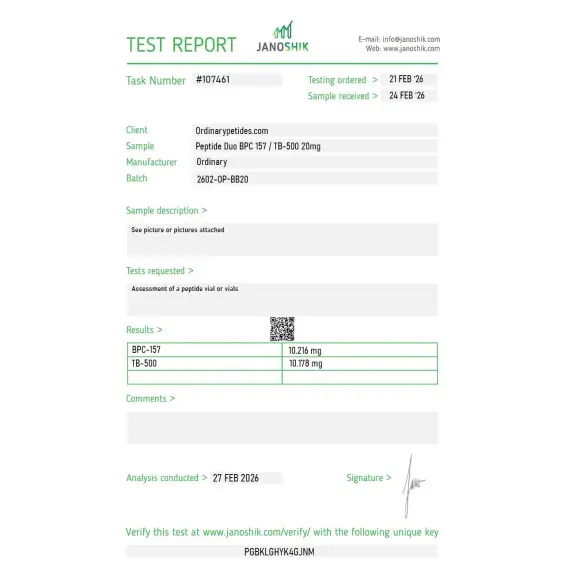
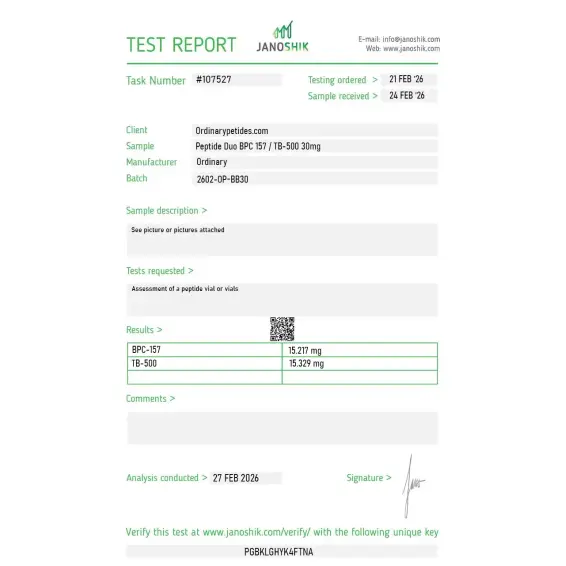
Certificate of Analysis
Independent test reports are available for Peptide Duo BPC-157 / TB-500 10mg, 20mg, and 30mg batches. These reports provide batch-level documentation and analytical verification information for research reference.



What earned the order is that the listing frames the duo as a regenerative-pathway research pairing with the two distinct mechanisms stated — angiogenic versus actin-sequestering — rather than leaning on the recovery-and-healing marketing that usually accompanies this combination. For mechanism work contrasting the co-formulation against each component, that honest framing was the deciding factor. Consistent across two orders.
We run the blend against each component alone — BPC-157 solo, TB-500 solo, the combination — as a three-arm design to isolate whether any interaction effect exists beyond the individual contributions. The co-formulation is the test arm; the standalones are the controls. Sourcing all three from one catalog with matched documentation keeps the only variable the combination itself. The blend held both activities across our regeneration-model conditions.
A two-peptide formulation demands component-resolved documentation, and that's where it fell short — I want each peptide's purity reported separately plus a chromatogram showing both peaks resolved at the stated ratio in the actual vial, not two analyses from two batches presented together. The blend performed, but for a co-formulation the ratio integrity is the thing a single combined purity figure structurally cannot confirm. Component-level QC is the baseline for any mixture.
The reason to study them co-formulated is that BPC-157 and TB-500 are the two compounds the regeneration literature pairs most often, yet they work through entirely separate mechanisms — angiogenic/NO-pathway signaling versus actin sequestering. The blend lets us probe whether the two converge or act independently in a single wound-healing model at a fixed ratio, rather than reconstructing the combination from two stocks. Both components gave their expected separate readouts in our endothelial and migration assays.
The BPC-157 / TB-500 stack — sometimes marketed as "BPC/TB Blend" or informally called the "Healing Stack" — combines two of the most widely researched tissue-repair peptides into a single protocol. BPC-157 is a 15-amino acid gastric peptide and TB-500 is a synthetic fragment of Thymosin Beta-4, a naturally occurring actin-regulating protein. While each peptide works through distinct molecular pathways, they are frequently combined because their mechanisms are considered complementary — BPC-157 drives local tissue repair and angiogenesis while TB-500 coordinates systemic cell migration, reduces fibrosis, and promotes long-range healing. Together they are used in research contexts targeting musculoskeletal injury, inflammation, and recovery.
Reconstitute with sterile bacteriostatic water under aseptic conditions, gently swirl until dissolved, calculate dilution carefully, and refrigerate after preparation.
Neither peptide is FDA-approved for therapeutic use. The blend is supplied strictly for research purposes only and is prohibited in professional athletic competition.
Potential research observations include altered angiogenesis signaling, tissue remodeling changes, or localized cellular responses depending on experimental conditions.
In research models, the blend is studied for supporting connective tissue repair pathways, cell migration signaling, angiogenesis, and recovery-related biological mechanisms.
That is a popular hypothesis, but not a confirmed clinical fact. The scientifically correct statement is only that their mechanisms may be theoretically complementary.
In the accessible peer-reviewed literature and official sources, no quality clinical evidence base specifically for the BPC-157 + TB-500 combination is visible.
TB-500 is not full-length Tβ4. In anti-doping work, the fragment Ac-LKKTETQ was identified in TB-500, which is why human data on full-length Tβ4 cannot automatically be transferred to TB-500.
Yes, but very limited ones: small pilot observations and weak studies, including a retrospective knee-pain series and a few pilot investigations in other indications.
It cannot be said confidently. For both components there is a lack of mature human safety data, and the FDA separately points to risks of immunogenicity and peptide impurities for compounded products.
No. BPC-157 is prohibited as an S0 Unapproved Substance, and thymosin-β4 derivatives such as TB-500 are prohibited as growth factor modulators.
BPC-157 primarily activates VEGFR2 to drive angiogenesis and new blood vessel formation, upregulates FAK-paxillin cell migration complexes, stimulates JAK-2 and ERK1/2 survival pathways, and protects epithelial and connective tissue. Its effects are most pronounced locally at or near the site of injury and it acts rapidly given its short half-life of under 30 minutes in circulation.
TB-500 works by binding G-actin — a monomeric form of the cytoskeletal protein actin — and regulating its availability for cell migration and tissue organization. This drives systemic healing by mobilizing progenitor cells from bone marrow, reducing fibrosis and scar formation, promoting endothelial cell migration for vessel repair, and improving connective tissue flexibility. TB-500's effects are more systemic and longer-range than BPC-157's.
The rationale for combining them is that BPC-157 handles the local molecular signaling for repair while TB-500 coordinates the broader cellular architecture of healing. They target different receptor systems and different stages of tissue repair, making true synergy — rather than simple addition — pharmacologically plausible, though not yet formally studied in combination in published research.
Preclinical evidence for each peptide individually includes accelerated tendon, ligament, and muscle healing, reduced inflammation and fibrosis, improved joint recovery, neuroprotection, and gut lining repair. In practice the combination is most commonly researched and anecdotally used for musculoskeletal injuries — particularly tendon and ligament tears, rotator cuff injuries, joint damage, and post-surgical recovery — where both local repair signaling and systemic cellular organization are needed simultaneously. Users and some functional medicine practitioners also report benefits for chronic inflammatory conditions and general tissue resilience.
No published research has formally studied the BPC-157 / TB-500 combination. All evidence for the stack comes from extrapolation of individual peptide studies — the vast majority of which are preclinical animal models — combined with anecdotal reports. Neither peptide is FDA-approved. BPC-157 is explicitly prohibited by the FDA from compounding and is banned by WADA under S0 Unapproved Substances. TB-500 is also prohibited by WADA. In 2025 a two-person pilot study showed IV BPC-157 was well tolerated in humans, and TB-500 has a similarly sparse human safety record. The combination's safety in humans is entirely unknown.
In research and wellness clinic contexts the duo is typically given as separate subcutaneous injections — sometimes on alternating days, sometimes simultaneously at different sites. Common anecdotal protocols use BPC-157 at 250 to 500 mcg daily or twice daily and TB-500 at 2 to 2.5 mg twice per week during a loading phase followed by a reduced maintenance dose. Some compounding pharmacies have historically supplied premixed vials — though this is now prohibited in the United States following the FDA's 2023 Category 2 designation for BPC-157.
Both peptides have shown minimal adverse effects in preclinical animal studies and very limited human data. The most commonly reported effects from the combination are mild injection site reactions and occasional transient fatigue or dizziness. The primary theoretical concern for BPC-157 — its angiogenic activity through VEGFR2 upregulation raising the possibility of promoting tumor vasculature — applies equally to the combination. TB-500's effects on cell migration and progenitor cell mobilization carry a similar theoretical concern in individuals with occult malignancy. Neither concern has been confirmed in human trials, but neither has been ruled out.
Anyone with active cancer or a history of cancer should not use either peptide individually or in combination. Competitive athletes are prohibited from using both under WADA regulations. Pregnant or breastfeeding women should not use it. People sourcing these compounds outside of a clinical trial or formal medical setting face additional risks from unverified purity and potency of black market products. Given that BPC-157 cannot be legally compounded in the United States and that no human combination trial data exists, this stack carries the same fundamental caveat as BPC-157 alone — the clinical evidence base to support its use in humans does not yet exist.





