
ARA 290 peptide (Cibinetide)
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
ARA 290 (Cibinetide): An EPO-Derived Peptide With a Clear Concept and a Real Clinical Trace
ARA 290, or cibinetide, is a short synthetic peptide derived from the B-helix of erythropoietin, but designed with emphasis not on hematopoiesis — rather on the research interest surrounding its nonerythropoietic reparative signaling. In the scientific context, this molecule attracted attention because it was developed as a more refined EPO-derived candidate: preserving the appeal of tissue-protective biology while moving away from the classic hematologic profile of full EPO.
In early studies and clinical observations, ARA 290 showed notable signals in areas such as small fiber neuropathy, neuropathic symptoms, and changes in small nerve fibers, which is exactly why it became particularly discussed within its category. Its appeal, however, does not rest on loud promises, but on a rare combination of a clear idea, careful design, and an already existing clinical biography — and for a peptide, that is, to put it mildly, rather good company.
It is also important that its status remains investigational: this is not an approved drug, but a candidate that earned attention through data rather than marketing noise. If what interests you is a peptide with a strong scientific concept, a real clinical trace, and a clear research rationale, ARA 290 is definitely worth a closer look.
ARA 290 (Cibinetide): A Scientific Review of the Innate Repair Receptor Agonist
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
ARA 290 — also known as cibinetide or helix-B surface peptide (HBSP) — is a synthetic 11-amino acid peptide engineered from a specific three-dimensional region of erythropoietin (EPO). EPO has two distinct biological personalities. One drives red blood cell production in bone marrow and carries well-known risks (thrombosis, hypertension at high doses). The other quietly activates a tissue-repair and anti-inflammatory system in damaged organs and nerves. ARA 290 was designed to isolate and deliver only that second function — the protective one — without triggering the first.
The peptide targets what researchers call the innate repair receptor (IRR) — a molecular partnership between the EPO receptor and CD131 (the beta-common receptor subunit). Across multiple published Phase 2 clinical trials — in patients with sarcoidosis-associated neuropathy, diabetic peripheral neuropathy, and diabetic macular oedema — the compound has shown a consistent safety profile and promising signals for neuropathic pain relief and structural nerve fibre regeneration.[1][2][3] No Phase 3 trial results have been published to date.
| At a glance | |
|---|---|
| Other names | Cibinetide, helix-B surface peptide (HBSP) |
| Sequence | pyroglutamate-EELERALNSS (11 amino acids) |
| Molecular weight | 1257 Da |
| Developed by | Michael Brines and Anthony Cerami, Araim Pharmaceuticals (Tarrytown, NY) |
| Primary target | Innate Repair Receptor (IRR): EPO receptor + CD131 heterodimer |
| Class | Non-erythropoietic, tissue-protective EPO-derived peptide |
| Highest clinical phase | Phase 2 (completed for sarcoidosis-SFN) |
| Regulatory status | Not approved; FDA Orphan Drug + Fast Track Designations (sarcoidosis neuropathy); EU Orphan Drug Designation |
| Development status | Phase 2 complete; end-of-Phase 2 FDA meeting completed; Phase 3 not yet publicly initiated |
The Scientific Foundation: Two Faces of Erythropoietin
For decades, erythropoietin was understood as a hormone with one primary job: stimulate bone marrow to produce red blood cells. But in the late 1990s and early 2000s, a different picture began to emerge. EPO receptors were found throughout the body — in the brain, peripheral nerves, heart, kidney, and immune cells — in places that have nothing to do with red blood cell production. And in tissue injury models, EPO seemed to be doing something completely different: suppressing inflammation, protecting neurons from apoptosis, promoting vascular repair.
Preclinical studies identified the presence of an endogenous protective system that is activated by inflammation, metabolic stress and tissue injury. The receptor for this response, the innate repair receptor (IRR), is a member of the type I cytokine receptor family and is a complex consisting of β common receptor (CD131) and erythropoietin receptor subunits. The principal mediator of this system is hypoglycosylated EPO produced in situ by many cells as a stress response.[10]
The problem with using full EPO therapeutically for tissue protection: it simultaneously activates the classical bone marrow EPO receptor homodimer, increasing red blood cell mass, blood viscosity, and thrombotic risk. To circumvent this problem, ARA 290 was developed as an engineered peptide that interacts only with the innate repair receptor.[6] Researchers Michael Brines and Anthony Cerami at Araim Pharmaceuticals identified a specific surface region of EPO — the helix-B domain — whose three-dimensional shape was responsible for IRR binding, distinct from the receptor surface that drives erythropoiesis.
Structure and Chemistry
ARA 290 is a linear synthetic peptide of 11 amino acids derived from the helix-B surface of EPO. Its sequence is pyroglutamate-EELERALNSS, and it carries a molecular weight of 1,257 Da — small enough to be chemically synthesised by standard solid-phase peptide synthesis.[6] The N-terminal pyroglutamate (a cyclised form of glutamine) provides metabolic stability compared to a free glutamine. Despite its short plasma half-life (measured in minutes), cibinetide triggers sustained biological effects when concentrations exceed the low nanomolar affinity of the receptor — a brief exposure window that is sufficient to initiate downstream signalling cascades that persist for much longer. This kinetic profile is actually a safety feature: rapid clearance limits systemic exposure while downstream repair-oriented cellular programmes continue running.
The Innate Repair Receptor: What It Does and Why It Matters
The IRR becomes locally upregulated following tissue injury, and its activation initiates a local anti-inflammatory response, inhibition of death signalling and anti-apoptosis, preventing overt tissue damage.[10] This means the receptor is not constitutively active across all tissues at all times — it is upregulated precisely where and when it is needed. ARA 290 therefore exerts its most significant effects at sites of active injury, not in healthy resting tissue. When ARA 290 engages the IRR, it activates JAK-2 and multiple downstream pathways:
| Effect | Mechanism | Biological consequence |
|---|---|---|
| Anti-inflammatory signalling | Suppression of TNF-α, IL-1β, and other pro-inflammatory cytokines | Reduced chronic tissue-damaging inflammation |
| Anti-apoptotic signalling | Inhibition of programmed cell death in stressed neurons and endothelial cells | Protection of nerve fibres and vessel walls |
| Endothelial barrier protection | Reduced vascular permeability | Better microvascular integrity in peripheral nerves |
| Macrophage/microglia modulation | Shift toward anti-inflammatory phenotype | Reduced neuroinflammation |
| Axonal regeneration support | Promotion of small fibre regrowth | Structural nerve repair (demonstrated by corneal confocal microscopy) |
| TRPV1 antagonism | Direct inhibition of the pain-sensing TRPV1 ion channel [8] | Additional analgesic effect independent of IRR |
Preclinical Evidence
| Model | Key findings |
|---|---|
| Diabetic mouse neuropathy (Akita mice) | Daily ARA 290 reversed neuronal dystrophy in sympathetic ganglia; protected small fibre structure |
| Rat neuropathic pain models [7] | Long-term relief of neuropathic pain requiring functional IRR; pain relief abolished in CD131 knockout mice, confirming IRR-dependent mechanism |
| Coronary atherosclerosis (rabbit) | Helix-B surface peptide suppressed coronary plaque progression |
| Colitis (mouse) | Cibinetide dampened innate immune cell functions and ameliorated experimental colitis |
| Ageing heart (mouse) [9] | Reduced cardiac inflammation and attenuated age-associated heart function declines |
| Spinal cord — microglia suppression [7] | ARA 290 produced long-term pain relief coupled with suppression of the spinal microglia response |
Clinical Trials: What the Human Data Shows
ARA 290 has been tested in multiple published Phase 2 human trials — better than animal data alone, but still insufficient to establish the compound as an approved therapy without Phase 3 confirmation.
Trial 1 — Sarcoidosis-associated small fibre neuropathy (pilot, 2012)
A total of 22 patients diagnosed with sarcoidosis and symptoms of small fibre neuropathy were enrolled in a double-blind, placebo-controlled exploratory trial of three-times-weekly intravenous dosing of ARA 290 (2 mg; n=12) or placebo (n=10) for four weeks.[1] No safety concerns were raised. The trial showed improvements in pain intensity, small fibre neuropathy symptom scores, quality of life, depressive symptoms, and fatigue in the ARA 290 group compared to placebo.
Trial 2 — Sarcoidosis-SFN with corneal confocal microscopy (2013 and 2017)
A larger Phase 2b trial of 64 participants used corneal confocal microscopy (CCM) — a non-invasive imaging technique that directly visualises small nerve fibres in the cornea as a surrogate for peripheral nerve fibre density — as an objective structural endpoint alongside pain scores.[2][4] The trial demonstrated that cibinetide increased corneal nerve fibre abundance — a structural, objective finding that suggested actual nerve fibre regeneration, not just symptomatic pain relief. Most neuropathy treatments address symptoms; ARA 290 appeared to be addressing the underlying structural deficit.
Trial 3 — Type 2 diabetes with neuropathy (2014)
ARA 290 (4 mg) or placebo were self-administered subcutaneously daily for 28 days, followed for an additional month without treatment.[3] No potential safety issues were identified. Subjects receiving ARA 290 exhibited an improvement in haemoglobin A1c and lipid profiles throughout the 56-day observation period. This trial used subcutaneous self-administration — a significant practical step toward real-world use. The HbA1c improvement was an unexpected metabolic finding that extends ARA 290’s potential relevance beyond pure neuropathy.
Trial 4 — Diabetic macular oedema (2020)
A Phase 2 trial of 9 patients received cibinetide 4 mg/day subcutaneously for 12 weeks for diabetic macular oedema.[5] There was no improvement in mean change from baseline in best corrected visual acuity, central retinal thickness, or central retinal sensitivity. However, there was an improvement in NEI Visual Function Questionnaire scores, and some participants experienced improvements in central retinal thickness, tear production, diabetic control, and albuminuria. No serious adverse events or anti-cibinetide antibodies were seen.
Summary of clinical trial data
| Trial | Design | N | Route | Duration | Key findings |
|---|---|---|---|---|---|
| Sarcoidosis-SFN pilot (2012) [1] | RCT, DB | 22 | IV | 4 weeks | Pain, fatigue, depression improved; no safety issues |
| Sarcoidosis-SFN CCM (2013/2017) [2][4] | RCT, DB, Phase 2b | 64 | IV/SC | 4 weeks | Corneal nerve fibre area increased; pain improved |
| T2DM + neuropathy (2014) [3] | RCT, DB | ~40 | SC | 28 days | HbA1c improved; lipid profiles improved; neuropathy symptoms improved |
| Diabetic macular oedema (2020) [5] | Phase 2 | 9 | SC | 12 weeks | Primary endpoints not met; safety confirmed; some exploratory signals |
What Is Confirmed and What Remains Unknown
| Confirmed by published data | Not yet established |
|---|---|
| IRR exists on human tissue, including peripheral nerve vasculature and immune cells [10] | Phase 3 efficacy in any indication |
| ARA 290 is well tolerated in short-term human studies (up to 12 weeks) [1][3][5] | Long-term safety beyond 12 weeks |
| No erythropoietic activity — no red blood cell stimulation [6] | Optimal dose and route for different conditions |
| Structural corneal nerve fibre regeneration observed in sarcoidosis patients [4] | Whether corneal fibre changes predict intraepidermal fibre changes |
| Neuropathic pain improvement in sarcoidosis-SFN (multiple trials) [1][2] | Efficacy in larger, confirmatory Phase 3 studies |
| HbA1c improvement in type 2 diabetes trial [3] | Mechanism of metabolic effects |
| No anti-cibinetide antibodies detected in any trial | Immunogenicity over longer use |
| Mechanism confirmed via CD131 knockout animal models [7] | Durability of effect beyond treatment period |
Safety Profile
Confirmed absent: The most important safety advantage is what ARA 290 doesn’t do. Because it does not activate the classical EPOR homodimer, it produces no measurable increase in haematocrit, haemoglobin, or red blood cell mass.[6] This eliminates the thrombotic and cardiovascular risks that limit EPO’s use in tissue-protective contexts.
Observed adverse events: Mild and transient injection site reactions and occasional headaches were reported at low frequency. No dose-limiting toxicities have been identified. No anti-cibinetide antibodies were detected, suggesting low immunogenicity risk.
| Concern | Status |
|---|---|
| Long-term safety (>12 weeks) | Not evaluated in humans |
| Effects of sustained immune modulation on infection susceptibility or cancer surveillance | Unknown; theoretically possible with any immunomodulatory agent |
| Safety in frail or multimorbid populations | Not systematically studied |
| Interactions with other immunomodulatory drugs | Not characterised |
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) | Not approved; Orphan Drug Designation for sarcoidosis neuropathy; Fast Track Designation [12] |
| EMA (Europe) | Not approved; EU Orphan Drug Designation for sarcoidosis [13] |
| Development stage | End-of-Phase 2 FDA meeting completed; Phase 3 not yet publicly initiated |
| Research chemical market | Sold by various vendors as “not for human consumption” |
Comparison with Related Approaches
| Compound / Approach | Mechanism | Status | Key difference from ARA 290 |
|---|---|---|---|
| Full EPO (rhEPO) | EPOR homodimer + IRR | FDA-approved (anaemia) | Stimulates erythropoiesis → thrombotic risk |
| ARA 290 (cibinetide) | Selective IRR agonist | Investigational | No erythropoiesis; tissue-protective only |
| Pregabalin / gabapentin | Voltage-gated calcium channel modulation | FDA-approved (neuropathic pain) | Symptomatic only; no structural repair |
| Duloxetine | Serotonin-noradrenaline reuptake inhibitor | FDA-approved (diabetic neuropathy) | Symptomatic only; no nerve regeneration |
| BPC-157 | Multiple growth factor pathways | Research only; no clinical trials | Systemic; different mechanisms; no human RCTs |
| Thymosin β4 | Actin sequestration; angiogenesis | Research only | Different mechanism; early-stage |
Potential Research Areas Beyond Current Trials
Small fibre neuropathy (multiple aetiologies beyond sarcoidosis and diabetes — Sjögren’s syndrome, idiopathic SFN, chemotherapy-induced neuropathy)
Cardiac protection and ageing: ARA 290 (cibinetide), an 11-amino acid non-hematopoietic peptide sequence within the cardioprotective domain of erythropoietin, mediates tissue protection by reducing inflammatory and fibrotic responses, and in aged mice reduced cardiac inflammation and attenuated age-associated declines in heart function.[9]
Autoimmune and inflammatory conditions: Colitis, lupus, and other conditions with overactive innate immunity.
Renal protection: Ischaemia-reperfusion injury; transplant protection; diabetic nephropathy (suggested by the albuminuria findings in the macular oedema trial[5]).
Neuroinflammatory diseases: Multiple sclerosis, early Alzheimer’s disease — preclinical signals only; no human trial data.
Common Misconceptions
“ARA 290 is just a form of EPO.”
Structurally derived from EPO’s helix-B domain, but functionally distinct.[6] It does not stimulate red blood cell production, does not raise haematocrit, and is not banned by WADA (unlike EPO). It activates a completely different receptor configuration — the IRR heterodimer — rather than the classical EPO receptor homodimer.
“It’s been proven to treat neuropathy.”
Phase 2 results are promising and the safety data is clean.[1][2][3] However, Phase 3 confirmatory trials have not yet been completed or published. Phase 2 results frequently do not replicate in Phase 3.
“It’s available as a research chemical, so it’s basically the same as what’s studied.”
Research chemical vendors sell compounds with variable purity, no sterility guarantees, no pharmaceutical-grade manufacturing standards, and no regulatory oversight. The compound studied in clinical trials was produced under GMP conditions by Araim Pharmaceuticals. These are not equivalent.
“Short-term safety means it’s safe long-term.”
The longest human trial duration has been 12 weeks.[5] Neuropathic conditions often require months to years of treatment. Long-term safety, including effects on immune surveillance and potential for any compensatory biological changes, has not been evaluated.
Frequently Asked Questions
Is ARA 290 approved anywhere?
No. It holds Orphan Drug Designation and Fast Track Designation in the US,[12] and Orphan Drug Designation in the EU[13] — but these are not approvals. No marketing authorisation exists in any jurisdiction.
What is small fibre neuropathy, and why does it matter here?
Small fibre neuropathy (SFN) is a condition involving damage to the small unmyelinated and lightly myelinated nerve fibres that carry pain, temperature, and autonomic signals. It causes burning pain, numbness, and autonomic symptoms. Sarcoidosis and diabetes are among the most common causes. No approved disease-modifying therapy exists — which is why ARA 290’s structural regeneration signal is considered significant.
Does ARA 290 increase red blood cell count?
No. This has been specifically measured across clinical trials, and no erythropoietic effect has been detected.[6] This is the central pharmacological distinction from full EPO.
What is the current development status?
As of April 2026, Phase 2 is complete for sarcoidosis-SFN. Araim Pharmaceuticals has conducted an end-of-Phase 2 meeting with the FDA. No Phase 3 trial has been publicly registered or results published.
Is it on the WADA prohibited list?
Not currently. Unlike EPO and erythropoiesis-stimulating agents, ARA 290 does not enhance red blood cell mass or oxygen-carrying capacity. The performance enhancement rationale for prohibition does not apply in the same way.
Key Takeaways
- ARA 290 represents a genuinely novel mechanistic approach — the first selective agonist of the innate repair receptor, designed to deliver EPO’s tissue-protective benefits without its haematologic risks.[6][10]
- The human clinical evidence is the strongest of any peptide in its category — multiple Phase 2 RCTs with published results in peer-reviewed journals.[1][2][3][4]
- Structural nerve regeneration — not just pain relief — is the most distinctive clinical signal, demonstrated by corneal confocal microscopy.[4] If confirmed in Phase 3, this would represent a mechanistic advance over all currently approved neuropathy treatments.
- The safety profile across completed trials is favourable, with no dose-limiting toxicities and no erythropoietic effects. But 12 weeks is the longest human exposure studied — long-term safety remains uncharacterised.
- Phase 3 data is absent. Phase 2 results, however promising, frequently fail to replicate at scale. The compound should not be considered proven effective pending confirmatory trials.
- Research chemical versions are not equivalent to pharmaceutical-grade cibinetide. Purity, sterility, and pharmacokinetic equivalence cannot be assumed from unregulated commercial sources.
References
Key Clinical Studies
- Heij L, Niesters M, Swartjes M, et al. Safety and efficacy of ARA 290 in sarcoidosis patients with symptoms of small fiber neuropathy: a randomized, double-blind pilot study. Molecular Medicine. 2012;18:1430–1436. PMC3563705
- Dahan A, Dunne A, Swartjes M, et al. ARA 290 improves symptoms in patients with sarcoidosis-associated small nerve fiber loss and increases corneal nerve fiber density. Molecular Medicine. 2013;19:334–345.
- Brines M, Dunne AN, van Velzen M, et al. ARA 290, a nonerythropoietic peptide engineered from erythropoietin, improves metabolic control and neuropathic symptoms in patients with type 2 diabetes. Molecular Medicine. 2015;20:658–666. PMC4365069
- Culver DA, Dahan A, Bajorunas D, et al. Cibinetide improves corneal nerve fiber abundance in patients with sarcoidosis-associated small nerve fiber loss and neuropathic pain. Investigative Ophthalmology & Visual Science. 2017;58(6):BIO52–BIO60.
- O’Leary OE, et al. A Phase 2 Clinical Trial on the Use of Cibinetide for the Treatment of Diabetic Macular Edema. Journal of Clinical Medicine. 2020;9(7):2225. doi: 10.3390/jcm9072225
Key Mechanistic and Preclinical Studies
- Brines M, Patel NSA, Villa P, et al. Nonerythropoietic, tissue-protective peptides derived from the tertiary structure of erythropoietin. Proceedings of the National Academy of Sciences USA. 2008;105(31):10925–10930.
- Swartjes M, van Velzen M, Niesters M, et al. ARA 290, a peptide derived from the tertiary structure of erythropoietin, produces long-term relief of neuropathic pain coupled with suppression of the spinal microglia response. Molecular Pain. 2014;10:13. PMC3928087
- Zhang W, Yu G, Zhang M. ARA 290 relieves pathophysiological pain by targeting TRPV1 channel: integration between immune system and nociception. Peptides. 2016;76:73–79.
- Winicki N, et al. A small erythropoietin derived non-hematopoietic peptide reduces cardiac inflammation, attenuates age-associated declines in heart function and prolongs healthspan. Frontiers in Cardiovascular Medicine. 2023. PMC9889362
Reviews
- Brines M, Cerami A. The receptor that tames the innate immune response. Molecular Medicine. 2012;18:486–496.
- Brines M, Cerami A. Erythropoietin-mediated tissue protection: reducing collateral damage from the primary injury response. Journal of Internal Medicine. 2008;264:405–432.
Regulatory Sources
- FDA Orphan Drug Designation and Fast Track Designation — Cibinetide (ARA 290) for sarcoidosis-associated neuropathic pain. Araim Pharmaceuticals. fda.gov
- EMA Orphan Drug Designation — Cibinetide for treatment of sarcoidosis. ema.europa.eu
Researchers and Institutions
- Michael Brines, MD, PhD — Araim Pharmaceuticals, Tarrytown, NY. Principal designer of ARA 290 / cibinetide.
- Anthony Cerami, PhD — Araim Pharmaceuticals. Co-developer; pioneering researcher in EPO tissue protection biology.
- Albert Dahan, MD, PhD — Leiden University Medical Center, Netherlands. Principal Investigator for multiple ARA 290 clinical trials.
- Rayaz A. Malik, MD, PhD — Weill Cornell Medicine Qatar. Lead expert on corneal confocal microscopy endpoints in cibinetide trials.
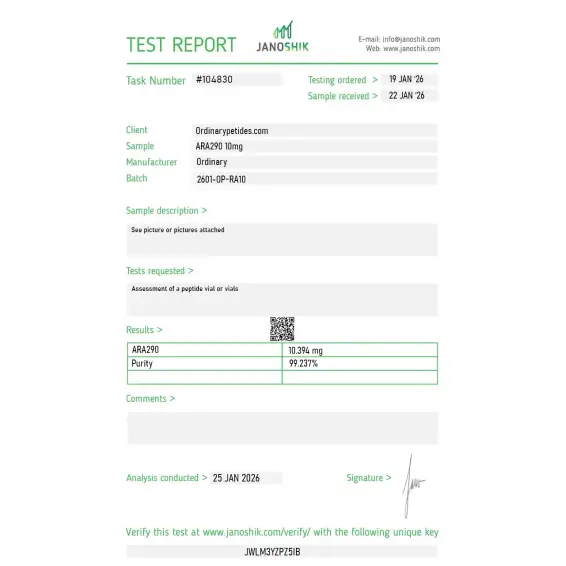
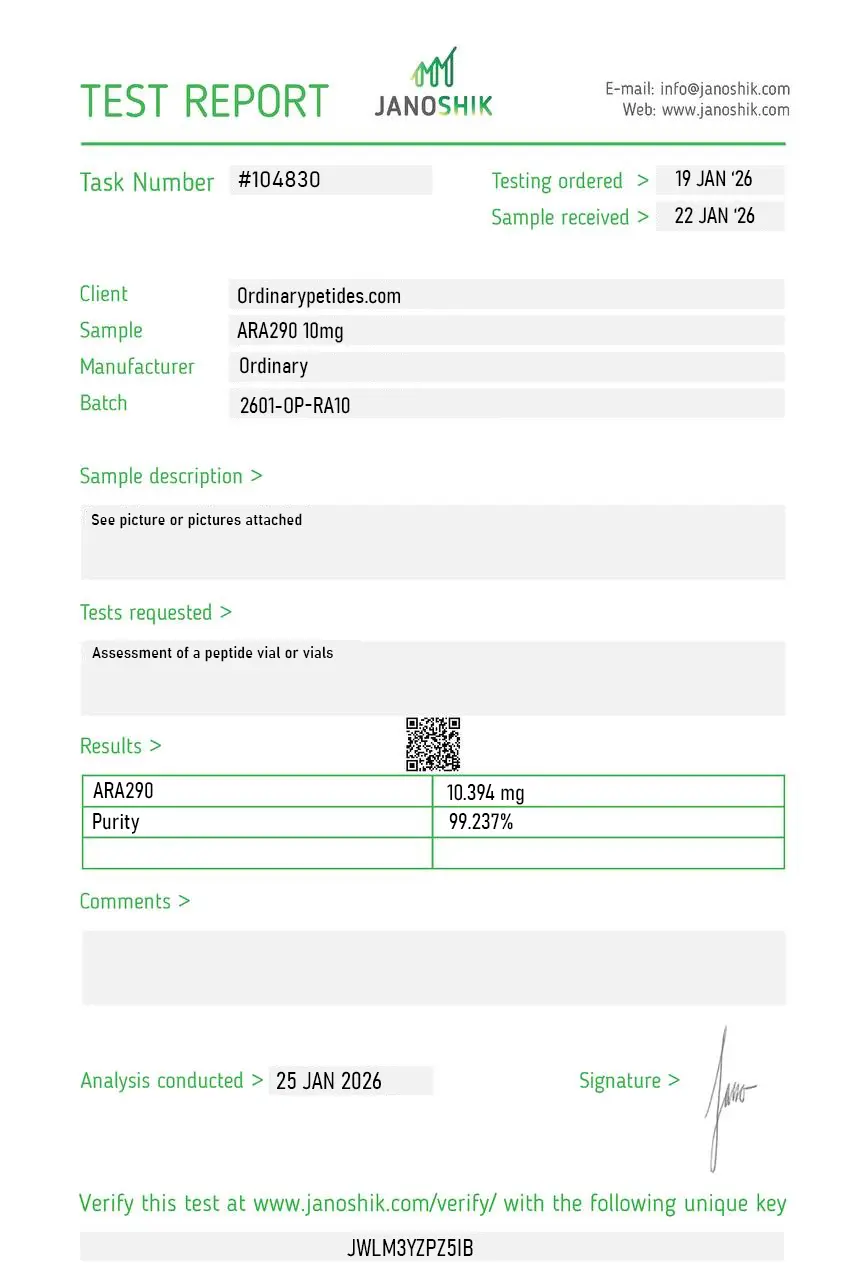
Certificate of Analysis
An independent test report is available for ARA-290. This report provides batch-level documentation and analytical verification information for research reference.
Based on 3 reviews
5.0
The entire research appeal is the receptor dissociation — ARA 290 was engineered from EPO's helix-B region to hit the innate repair receptor, the EPOR/CD131 heteromer, while deliberately not triggering the classical homodimeric EPO receptor that drives erythropoiesis. For studying tissue-protective EPO signaling without the hematopoietic confound, that uncoupling is the whole point, and you can't get it from EPO itself. The material reproduced the IRR-selective signaling in our assays as the design intends.
We work the β-common-receptor side specifically — CD131 as the shared signaling subunit across the GM-CSF/IL-3/IL-5 family and its role in the tissue-protective heteromer with EPOR. ARA 290 is one of the cleaner pharmacological tools for probing the repair-receptor arm without pulling in classical EPO signaling. Sourcing it reliably matters because the receptor-selectivity readout is the experiment, and the material held that selectivity across our conditions.
What made it worth ordering here is the framing precision — non-erythropoietic is stated plainly, which is the single most important fact about this molecule and the thing careless sources blur by lumping it with EPO mimetics. For receptor-pathway work contrasting IRR-selective signaling against full EPO's dual activity, having the listing get that distinction right was what earned the order. Consistent across two orders.
ARA290 selectively binds to the innate repair receptor (IRR), activating tissue-protective and anti-inflammatory signaling pathways without stimulating erythropoiesis.
Preclinical studies have demonstrated anti-inflammatory effects, neuroprotective signaling, and improved peripheral nerve repair markers in experimental models.
In research settings, signaling pathway changes are often observed within days to weeks depending on dosage and protocol design, though timelines vary by study model.
Cibinetide is another name for ARA290, a synthetic peptide derived from erythropoietin designed to activate tissue-protective pathways without affecting red blood cell production.
As an experimental compound, ARA290 lacks extensive long-term safety data, and peptides in general may carry risks related to dosing, immune response, and regulatory oversight if not used in controlled research environments.
Yes. Cibinetide is the more modern name of the molecule previously known as ARA 290.
p>No, not in the usual sense. It is a short peptide designed from a structural motif of EPO, but without the goal of stimulating erythropoiesis.
Mainly for conditions involving inflammation, neuropathy, and microvascular injury, including sarcoidosis-associated SFN, painful diabetic neuropathy, DME, and transplant-related indications.
Yes. The most noticeable ones are in neuropathic symptoms and the structure of small nerve fibers. But that is still not the same as a fully proven standard therapy.
No reliable evidence of FDA or EMA marketing approval is visible. The most accurate description remains that it is an investigational phase II candidate.
The key point is that ARA 290 should not be treated as an already proven "regenerative medicine." It is interesting, biologically plausible, and in some ways promising, but the evidence base remains limited.
ARA-290, also known as Cibinetide, is a synthetic 11-amino acid peptide developed by Araim Pharmaceuticals. It was engineered by isolating and modifying the helix-B surface domain of erythropoietin (EPO) — the hormone produced by the kidneys that naturally stimulates red blood cell production. The key innovation was identifying the portion of EPO responsible for tissue protection and anti-inflammatory activity and separating it from the portion responsible for red blood cell stimulation. The result is a compound that captures EPO's regenerative and neuroprotective properties without triggering erythropoiesis, making it both safer and more targeted than EPO itself.
ARA-290 selectively binds to and activates the Innate Repair Receptor (IRR) — a heteroreceptor complex formed by the EPO receptor and the beta-common receptor (CD131). This receptor is upregulated specifically in response to tissue injury, hypoxia, and metabolic stress — meaning it becomes more available precisely when the body needs repair. When ARA-290 activates the IRR it triggers multiple downstream pathways including suppression of pro-inflammatory cytokines such as IL-1, IL-6, IL-12, and TNF-alpha, activation of tissue repair and regeneration signaling, neuroprotection via suppression of microglial inflammatory responses in the spinal cord, promotion of angiogenesis and new blood vessel formation in damaged tissue, improvement of insulin sensitivity, and protection of endothelial cells. Because it does not bind the classic EPO receptor homodimer it produces none of EPO's hematopoietic effects or associated cardiovascular risks.
ARA-290 has completed Phase 2 clinical trials in several conditions. In sarcoidosis-associated small fiber neuropathy — where chronic inflammation destroys small nerve fibers — cibinetide at 4 mg daily for 28 days produced significant improvements in pain intensity, nerve fiber regeneration measured by corneal fiber density, and physical functioning scores. In type 2 diabetes with painful neuropathy, 28 days of daily subcutaneous treatment improved HbA1c levels, lipid profiles, and neuropathic symptoms. In renal ischemia-reperfusion injury models it demonstrated significant kidney protection. Other areas under investigation include diabetic wound healing, islet transplant protection in type 1 diabetes, diabetic macular edema, cardiovascular ischemic injury, and autoimmune inflammatory diseases including lupus.
ARA-290 is not FDA-approved or EMA-approved for any indication. It remains an investigational drug studied through Phase 2 and Phase 3 clinical trials. Unlike many research peptides it is typically not freely available through general research peptide vendors due to pharmaceutical intellectual property protections and its more advanced clinical development status. It is accessible only through clinical trial participation or specialized physician prescribing in select jurisdictions.
It is given as a subcutaneous injection, self-administered by patients in most trial protocols. Doses studied in clinical trials range from 2 mg to 4 mg per injection, administered once daily or several times per week. Treatment courses in trials have typically lasted 4 to 12 weeks depending on the condition being treated. It is supplied as a sterile solution and must be kept refrigerated.
ARA-290 has demonstrated a notably clean safety profile across Phase 2 trials with no dose-limiting toxicity observed. The most common side effect is mild injection site reaction including localized redness or discomfort. Rare cases of mild hypotension have been reported. No increases in red blood cell count, hematocrit, or cardiovascular risks associated with EPO have been observed — which is the primary safety advantage over EPO itself. Long-term safety data beyond 12-week trial periods is still limited.
People with known hypersensitivity to EPO or EPO-derived compounds should exercise caution and disclose this to their physician. Those with severe cardiovascular instability should be monitored given occasional hypotensive effects. Pregnant or breastfeeding women should not use it in the absence of safety data for these populations. Because it is an investigational drug outside of clinical trials, use should only occur under qualified medical supervision. Its mechanism of activating tissue repair and angiogenic pathways raises the theoretical caution — applicable to most angiogenic compounds — in individuals with active cancer.





