

KPV
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
KVP (Lys–Val–Pro): A Short Research Tripeptide Around Which It Is All Too Easy to Confuse Science and Similar Letters
KVP is the tripeptide Lys–Val–Pro, which in published sources appears as a small research candidate at the intersection of PepT1 biology, food-derived bioactive peptides, and inflammatory models. In the research context, it is associated with a transport-based logic in which short tripeptides may participate in intracellular signaling scenarios, and in secondary reviews KVP is described as a molecule with a potentially interesting anti-inflammatory profile.
But this is exactly where the most intriguing part begins: some of the louder descriptions attributed to KVP seem, in the published literature, to be drawn from data on KPV — and that is already a completely different peptide. That is why KVP is interesting not as a "ready-made hit," but as a careful research molecule for those who like to dig deeper and see where a beautiful hypothesis ends and the real evidence base begins.
Practical Takeaway
If what you need is a peptide with a live scientific intrigue, a PepT1 context, and a noticeable share of nomenclature detective work, KVP is exactly that kind of case. This is not a story about loud promises — it is a story about a short peptide that deserves to be looked at carefully.
KPV (Lys-Pro-Val): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
KPV is a tripeptide — three amino acids long — that was discovered by asking a deceptively simple question: which part of α-melanocyte-stimulating hormone (α-MSH) is responsible for its anti-inflammatory activity? The answer, identified in the 1990s and definitively confirmed in subsequent decades, turned out to be the C-terminal three amino acids: lysine-proline-valine (KPV). This minimal fragment retains potent anti-inflammatory activity comparable to full-length α-MSH, and does so through an entirely different mechanism — not through melanocortin receptors (which mediate α-MSH’s tanning, appetite, and sexual effects), but through a gut peptide transporter called PepT1.
The discovery established two things that remain remarkable twenty-five years later: first, that the anti-inflammatory and the endocrine activities of α-MSH are pharmacologically separable; second, that a naturally occurring tripeptide small enough to be absorbed from the gut can suppress the master transcription factor of inflammation (NF-κB) at nanomolar concentrations in multiple cell types without apparent toxicity.[1]
The evidence for KPV is almost entirely preclinical — two decades of cell culture and animal model data, principally from IBD models and dermatological models, with a substantial nanoparticle drug delivery research programme aimed at solving the fundamental problem of getting KPV to inflamed colonic tissue in useful concentrations after oral administration. As of 2026, no human clinical trial data has been published. The translational gap between mouse colitis models and human IBD trials has not yet been crossed.
| At a glance | |
|---|---|
| Full name | Lys-Pro-Val (KPV); α-MSH C-terminal tripeptide; α-MSH(11-13) |
| Type | Naturally occurring tripeptide; anti-inflammatory peptide |
| Molecular weight | ~342 Da |
| Sequence | Lysine–Proline–Valine |
| Origin | C-terminal residues 11–13 of α-melanocyte-stimulating hormone (α-MSH) |
| Primary mechanism | PepT1-mediated cellular uptake → NF-κB suppression |
| Binds melanocortin receptors? | ✅ No — explicitly demonstrated not to bind MC1R, MC3R, MC5R |
| Evidence base | Entirely preclinical (in vitro + animal models) |
| Human clinical trials | ❌ None |
| FDA/regulatory status | ❌ Not approved; research chemical |
From α-MSH to KPV: The Discovery
α-Melanocyte-stimulating hormone (α-MSH) is a 13-amino acid neuropeptide derived from POMC by post-translational cleavage. Its sequence is: Ac-Ser¹-Tyr²-Ser³-Met&sup4;-Glu&sup5;-His&sup6;-Phe&sup7;-Arg&sup8;-Trp&sup9;-Gly¹⁰-Lys¹¹-Pro¹²-Val¹³-NH&sub2;. α-MSH has a documented dual nature: it is the hormone responsible for skin pigmentation (via MC1R) and also a hormone with anti-inflammatory, antipyretic, and immunomodulatory effects.
Anna Catania, James Lipton, and colleagues established in the early-to-mid 1990s that systematic fragmentation of α-MSH could separate its anti-inflammatory activity from its melanocortin receptor-mediated activities. The critical finding: the C-terminal tripeptide — positions 11-13: Lys-Pro-Val — retained potent anti-inflammatory activity despite lacking the core melanocortin receptor-binding sequence at positions 6–9 (His-Phe-Arg-Trp). The C-terminal peptide fragment of α-MSH (KPV) exerts a similar or even more pronounced anti-inflammatory activity as full-length α-MSH. This established that the tanning, appetite, and receptor-mediated effects of α-MSH could be entirely dissociated from its anti-inflammatory effects.[3]
The mechanistic puzzle was resolved in a landmark 2008 Gastroenterology paper by Dalmasso et al.: KPV’s anti-inflammatory activity in intestinal epithelial cells is mediated through PepT1 — the proton-coupled oligopeptide transporter (SLC15A1) expressed on the intestinal epithelial brush border. The anti-inflammatory effect of KPV is not MCR-mediated but PepT1-mediated, as confirmed by the finding that KPV does not bind to MC1, MC3, or MC5 receptors and does not compete with α-MSH.[1]
The Two Mechanisms of KPV
Mechanism 1: PepT1-mediated intestinal uptake
PepT1 is a transporter expressed on the apical surface of small intestinal enterocytes that normally transports di- and tri-peptides from the gut lumen during protein digestion. Its defining feature for KPV’s pharmacology: PepT1 expression is dramatically upregulated in inflamed colonic epithelium in IBD. Normal colonocytes have low PepT1 expression; inflamed IBD mucosa has high PepT1 expression. This creates a selectivity mechanism: since expression of colonic hPepT1 is up-regulated in IBD, its transport activity constitutes a potential new target for anti-inflammatory therapies.[1]
The sequence: KPV reaches inflamed colonic epithelium → upregulated PepT1 transports KPV across the apical membrane → intracellular KPV inhibits NF-κB activation by blocking IκB-α degradation → pro-inflammatory cytokines (IL-8, TNF-α, IL-6) transcription is reduced. The Km for KPV transport by hPepT1 was measured at approximately 700 µM, explaining why delivery concentration matters. PepT1 is also expressed by intestinal immune cells (including T cells), providing a second compartment through which KPV can reach immune cells in inflamed bowel tissue.
Mechanism 2: Direct intracellular NF-κB suppression
Independent of PepT1 transport, once KPV reaches intracellular compartments by any route, it acts at the level of IκB-α to suppress NF-κB activation. After TNF-α treatment in the presence of KPV, IκB-α protein level was higher compared with cells treated with TNF-α alone, suggesting a partial inhibitory effect of KPV on TNF-α-induced IκB-α degradation. NF-κB suppression has been demonstrated in colonic epithelial cells (Caco2-BBE), T lymphocytes (Jurkat), macrophages (RAW 264.7), keratinocytes, and vascular endothelial cells — consistent across cell types regardless of which inflammatory stimulus was used.[3]
Endogenous Biology: KPV as a Natural Anti-Inflammatory Signal
KPV is not purely synthetic — it is a naturally occurring fragment. α-MSH is processed in multiple tissues, and the C-terminal tripeptide KPV appears in physiological contexts as part of normal anti-inflammatory signalling during the resolution phase of inflammation. This endogenous origin is important for two reasons: as a naturally occurring tripeptide fragment, KPV is unlikely to be recognised as foreign by the immune system; and the anti-inflammatory activity is physiologically calibrated — it suppresses excessive NF-κB activation but does not eliminate baseline inflammatory signalling needed for normal immune defence.
Preclinical Evidence: Intestinal Inflammation (IBD)
The 2008 landmark papers
Dalmasso et al., Gastroenterology 2008: Established PepT1 as the transport mechanism. In vivo: orally delivered KPV at 100 µM significantly decreased severity of both DSS-induced colitis (chemical model) and TNBS-induced colitis (immunological model) in mice, measured by body weight preservation, myeloperoxidase (MPO) activity, histological inflammation scores, and pro-inflammatory cytokine mRNA levels.[1]
Kannengiesser et al., Inflammatory Bowel Disease 2008: KPV showed significant anti-inflammatory effects in DSS colitis and CD45RBhi T-cell transfer colitis (a model more analogous to Crohn’s disease). Crucially, KPV retained efficacy in mice with a nonfunctional MC1R, confirming MCR-independence.[2]
The delivery technology problem and its partial solutions
Raw KPV, taken orally, faces severe pharmacological obstacles: rapid degradation by intestinal peptidases, poor delivery to the colon, and a Km of ~700 µM requiring high local concentrations at the epithelial surface. The research trajectory from 2008 onwards focused substantially on drug delivery strategies.
The nanoparticle approach addresses both the degradation problem and the targeting problem. Subsequent iterations have explored exosome-based delivery, prodrug strategies, and combination loading (KPV + FK506). None has yet entered human trials.
Preclinical Evidence: Skin and Wound Healing
In multiple mouse models of contact dermatitis (irritant and allergic), topical or systemic KPV suppresses the inflammatory response. A particularly striking finding: KPV can induce hapten-specific immune tolerance — a persistent state of reduced reactivity to specific allergens following KPV treatment, mediated via IL-10 and persisting after KPV is withdrawn. This tolerisation effect distinguishes KPV from conventional topical anti-inflammatories (steroids, tacrolimus), which provide symptomatic relief without immunological reprogramming.
KPV also promotes wound healing by accelerating re-epithelialisation, reducing matrix metalloproteinase expression, and stimulating keratinocyte migration and proliferation. A 2025 study (Sung et al.) showed KPV protects keratinocytes from particulate matter-induced apoptosis and inflammation. Additionally, unlike corticosteroids — which reduce inflammation but increase infection susceptibility — KPV has demonstrated antimicrobial activity against Staphylococcus aureus and antifungal activity against Candida albicans in a vaginal infection model, a dual anti-inflammatory + antimicrobial profile potentially advantageous in IBD and skin conditions where microbial dysbiosis accompanies inflammation.[6]
Evidence Summary
| Domain | Model | Finding | Evidence quality |
|---|---|---|---|
| NF-κB suppression | Multiple cell lines (Caco2, Jurkat, RAW 264.7) | Consistent IκB-α stabilisation at 10 nM | Strong in vitro |
| IBD — DSS colitis [1] | Mouse | Oral KPV reduces body weight loss, MPO, histology, cytokines | Moderate preclinical |
| IBD — T-cell transfer colitis [2] | Mouse (CD45RBhi) | Anti-inflammatory; MCR-independence confirmed | Moderate preclinical |
| IBD — HA-KPV-NPs [5] | Mouse DSS colitis | HA-NP system dramatically outperforms free KPV | Moderate preclinical |
| Contact dermatitis | Mouse | Reduced inflammation; hapten-specific tolerance induction via IL-10 | Moderate preclinical |
| Wound healing (intestinal) | Caco2 monolayer | Dose-dependent recovery of wounded epithelium | In vitro |
| Antimicrobial [6] | S. aureus, C. albicans | Activity demonstrated | Preliminary preclinical |
| Human clinical trials | None | No data | ❌ N/A |
The KPV Delivery Challenge: Why No Human Trials Yet
KPV’s therapeutic target in IBD is the inflamed colonic mucosa. Reaching that target from oral administration requires surviving gastric acid (pH 1–2), small intestinal peptidases that degrade tripeptides rapidly during nutrient absorption, and absorption from the small intestine before reaching the colon. KPV’s small size (342 Da) and PepT1 affinity mean it would largely be absorbed and degraded before reaching inflamed colonic tissue. The concentration needed at the colonic epithelial surface (informed by the 700 µM Km for PepT1) is far above what simple oral free-peptide administration achieves.
The HA-nanoparticle work addressed this directly with impressive mouse results — but the rodent GI tract is smaller, transit time is different, and the comparison of DSS colitis in mice to human IBD is not straightforward. A prodrug approach, where KPV is covalently modified to protect it during transit and released by colonic enzymatic activity, is an alternative strategy explored in 2024 papers. None has yet entered human trials. Peptide-based therapeutics have emerged as promising alternatives, offering high specificity, favourable safety profiles, and unique biological activities compared to traditional treatments; however, challenges including enzymatic degradation, poor oral bioavailability, and instability hinder their clinical translation.[7]
Comparison: KPV vs. α-MSH vs. K(D)PT
| Compound | Length | MCR activity | Anti-inflammatory mechanism | Status |
|---|---|---|---|---|
| α-MSH | 13 AA | Yes — MC1R, MC3R, MC4R | MCR-mediated + non-MCR | Research; not approved |
| KPV (Lys-Pro-Val) | 3 AA | ✅ No | PepT1-mediated + NF-κB suppression | Research; no human trials |
| K(D)PT (Lys-[D-Pro]-Thr) | 3 AA | Minimal | IL-1 receptor interaction; NF-κB suppression | Research; no human trials |
Safety Profile
KPV’s safety profile, within the limits of available data, is reassuring. As a naturally occurring fragment of α-MSH, the human body produces it. Absence of MCR activity means no tanning, no appetite effects, no Melanotan II-like nausea, flushing, or erection. No cytotoxicity has been observed in multiple cell types at doses substantially above those producing anti-inflammatory effects. No significant systemic toxicity was reported in rodent models at therapeutic doses, including in chronic colitis models. KPV’s suppression of NF-κB appears to modulate pathological excess NF-κB activation rather than eliminating physiological NF-κB function required for normal immune defence — distinguishing it from broad immunosuppressants like corticosteroids. The complete absence of human pharmacokinetic or safety data means organ-specific effects, dose-limiting toxicities, drug-drug interactions, and chronic exposure safety are all uncharacterised.
Common Misconceptions
“KPV works like a weaker version of Melanotan or α-MSH.”
KPV has no melanocortin receptor activity whatsoever — confirmed in multiple studies. It does not cause tanning, sexual stimulation, appetite effects, or the nausea and flushing seen with MT-2 and Melanotan I. It works through a completely different receptor system (PepT1) and a completely different molecular mechanism (NF-κB suppression). Calling it “weaker α-MSH” is pharmacologically incorrect.
“Oral KPV is effective for IBD based on the mouse studies.”
⚠️ The mouse studies used oral KPV in specially engineered nanoparticle/hydrogel delivery systems that substantially increased colonic delivery efficiency. Simple oral KPV (free peptide in water) does not recapitulate these conditions. The free-peptide mouse colitis studies used direct gavage concentrations of 100 µM. This is not replicated by standard oral supplementation, and the community narrative that presents KPV as an orally bioavailable anti-inflammatory for gut conditions is overoptimistic relative to what the pharmacology supports for simple oral free-peptide administration.
“KPV is the active anti-inflammatory part of BPC-157.”
KPV and BPC-157 are unrelated compounds from different origins. BPC-157 derives from a gastric protein; KPV derives from α-MSH. They may have overlapping effects on gut inflammation through different mechanisms, but they are distinct molecular entities.
Frequently Asked Questions
Why are there no human trials despite 20+ years of preclinical evidence?
The primary obstacle is drug delivery. KPV’s oral bioavailability to the colon is very poor without the nanoparticle systems that make it work in mice. Moving from HA-NP/hydrogel systems that work in mice to a GMP-manufactured oral formulation suitable for human trials is a substantial pharmaceutical development challenge requiring industry investment. The pharmacology is well established; commercial translation has not been initiated.
Could KPV be used as a rectal suppository or enema for IBD?
This is pharmacologically the most rational delivery route for colitis — bypassing the small intestine entirely and directly contacting the colonic mucosa. Topical/rectal formulations of mesalazine, steroids, and biologics are already used clinically for distal colitis. A rectal KPV formulation would address the colonic delivery problem more directly than oral administration. This route has not been formally studied in published papers but has strong logical appeal.
Is KPV in topical skincare products the same compound?
Some skincare products contain the tripeptide Lys-Pro-Val as an additive marketed for skin-soothing properties. The concentrations in topical cosmetic products are generally far below those studied in research, and the evidence base for topical KPV in skincare is not the same as the IBD research literature. Topical application for skin inflammation is the area where KPV may have the most practical near-term accessibility, given that the gut delivery problem does not apply.
Key Takeaways
- KPV is one of the smallest and most elegantly mechanised anti-inflammatory peptides in this entire series. Three amino acids that suppress NF-κB through PepT1 transport — a mechanism selective for inflamed tissue (where PepT1 is upregulated) and entirely dissociated from α-MSH’s hormonal and pigmentary effects.[1]
- The pharmacological rationale is solid and multiply independently replicated. MCR-independence, PepT1 dependence, NF-κB suppression, and in vivo colitis efficacy have been confirmed by multiple research groups. The basic science is not in question.
- ⚠️ The translational gap is real and not yet bridged. Zero human clinical trial data exists. The oral delivery problem for free KPV to reach inflamed colonic tissue is substantial. Nanoparticle/hydrogel systems that work in mice represent significant pharmaceutical development that has not yet transitioned to human-use formulations.
- The skin/dermatology data is the most clinically accessible application. Topical KPV for skin inflammation avoids the gut delivery problem entirely. The tolerance-induction finding (persistent hapten-specific immune tolerance via IL-10) is particularly compelling and mechanistically distinct from conventional dermatological anti-inflammatories.
- ⚠️ Community oral use of free-peptide KPV for IBD/gut health likely does not achieve the colonic concentrations demonstrated in animal models. The physiology of oral peptide absorption does not favour free tripeptides reaching inflamed colonic tissue intact at therapeutically relevant concentrations.
- KPV has one of the most favourable theoretical safety profiles of any compound in this series. An endogenous tripeptide that selectively modulates excess NF-κB activation without MCR effects, without systemic immunosuppression, and with no demonstrated preclinical toxicity.
References
Foundational Mechanism Papers
- Dalmasso G, Charrier-Hisamuddin L, Nguyen HT, Yan Y, Sitaraman S, Merlin D. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology. 2008;134:166–178. PMC2431115
- Kannengiesser K, Maaser C, Heidemann J, et al. Melanocortin-derived tripeptide KPV has anti-inflammatory potential in murine models of inflammatory bowel disease. Inflammatory Bowel Diseases. 2008;14:324–331.
α-MSH and Related Peptides Review
- Brzoska T, Luger TA, Maaser C, Abels C, Böhm M. Alpha-melanocyte-stimulating hormone and related tripeptides: biochemistry, antiinflammatory and protective effects in vitro and in vivo. Endocrine Reviews. 2008;29:581–602. PMC2095288
- Luger TA, Scholzen TE, Brzoska T, Böhm M. New insights into the functions of α-MSH and related peptides in the immune system. Annals of the New York Academy of Sciences. 2003;994:133–140.
Drug Delivery / Nanoparticle Technology
- Xiao B, Xu Z, Viennois E, Zhang Y, Zhang Z, Zhang M, Han MK, Kang Y, Merlin D. Orally targeted delivery of tripeptide KPV via hyaluronic acid-functionalized nanoparticles efficiently alleviates ulcerative colitis. Molecular Therapy. 2017;25(7):1628–1640. PMC5498804
Antimicrobial
- Singh M, Mukhopadhyay K. C-terminal amino acids of alpha-melanocyte-stimulating hormone are requisite for its antibacterial activity against Staphylococcus aureus. Antimicrobial Agents and Chemotherapy. 2011;55:1920–1929.
Review: IBD Peptide Therapeutics
- Peptide-based therapeutic and delivery strategies for inflammatory bowel disease: challenges and future directions. PMC12272339. 2025.
Key Investigators
- Anna Catania, MD, PhD — Istituto di Ricerche Farmacologiche Mario Negri, Milan; one of the original researchers identifying KPV’s anti-inflammatory activity and characterising its non-MCR mechanism.
- James M. Lipton, PhD — Tulane University Medical Center; co-founder with Catania of the α-MSH/KPV anti-inflammatory research programme; co-inventor of KPV dermatological patent (US 6,894,028 B2, 2005).
- Didier Merlin, PhD — Georgia State University / Atlanta VA Medical Center; led the nanoparticle drug delivery programme for KPV in IBD; principal author on the HA-KPV-NP Molecular Therapy 2017 paper.
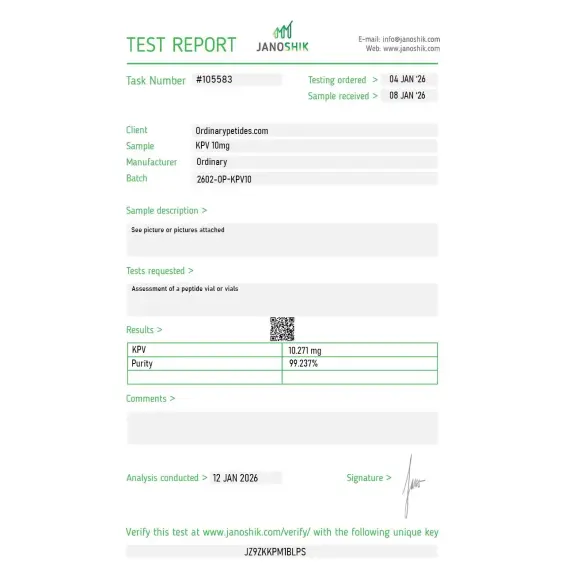
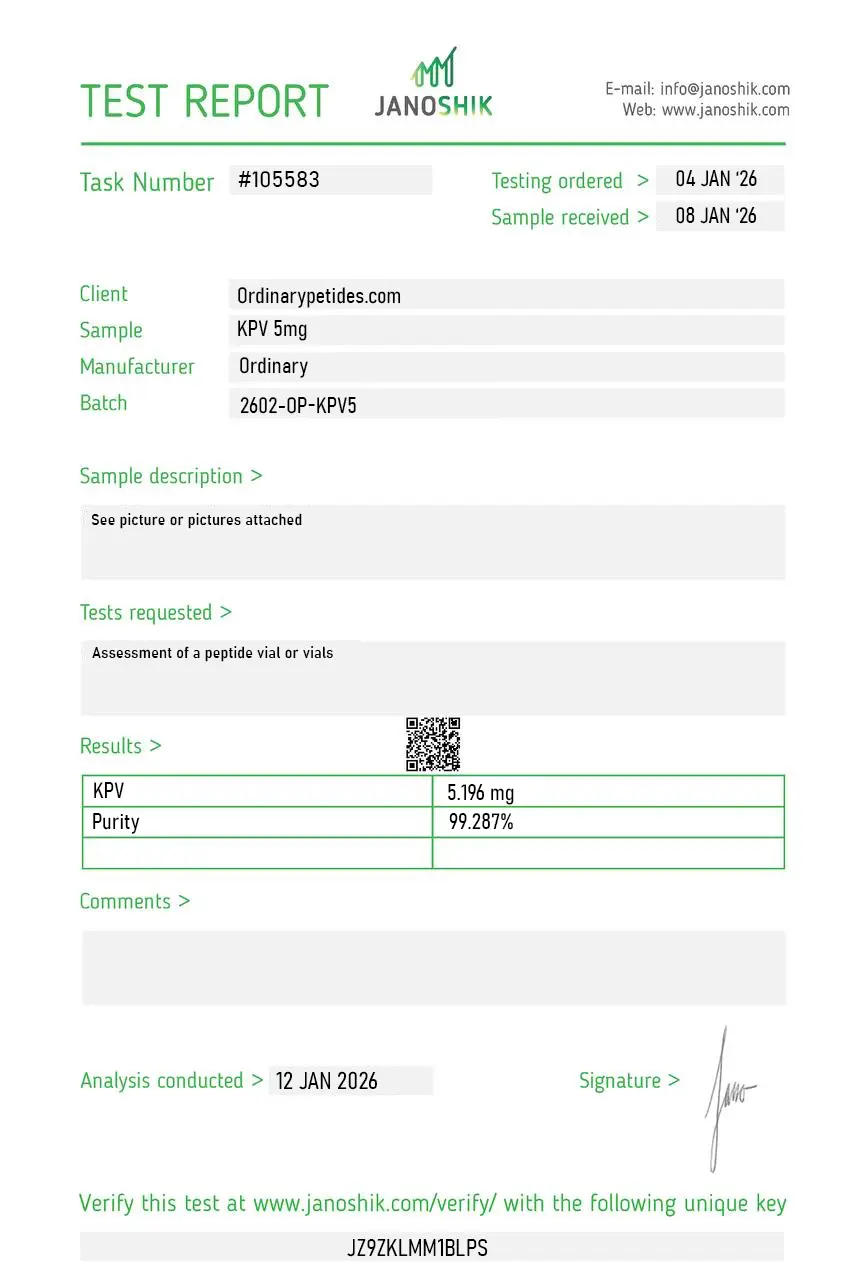
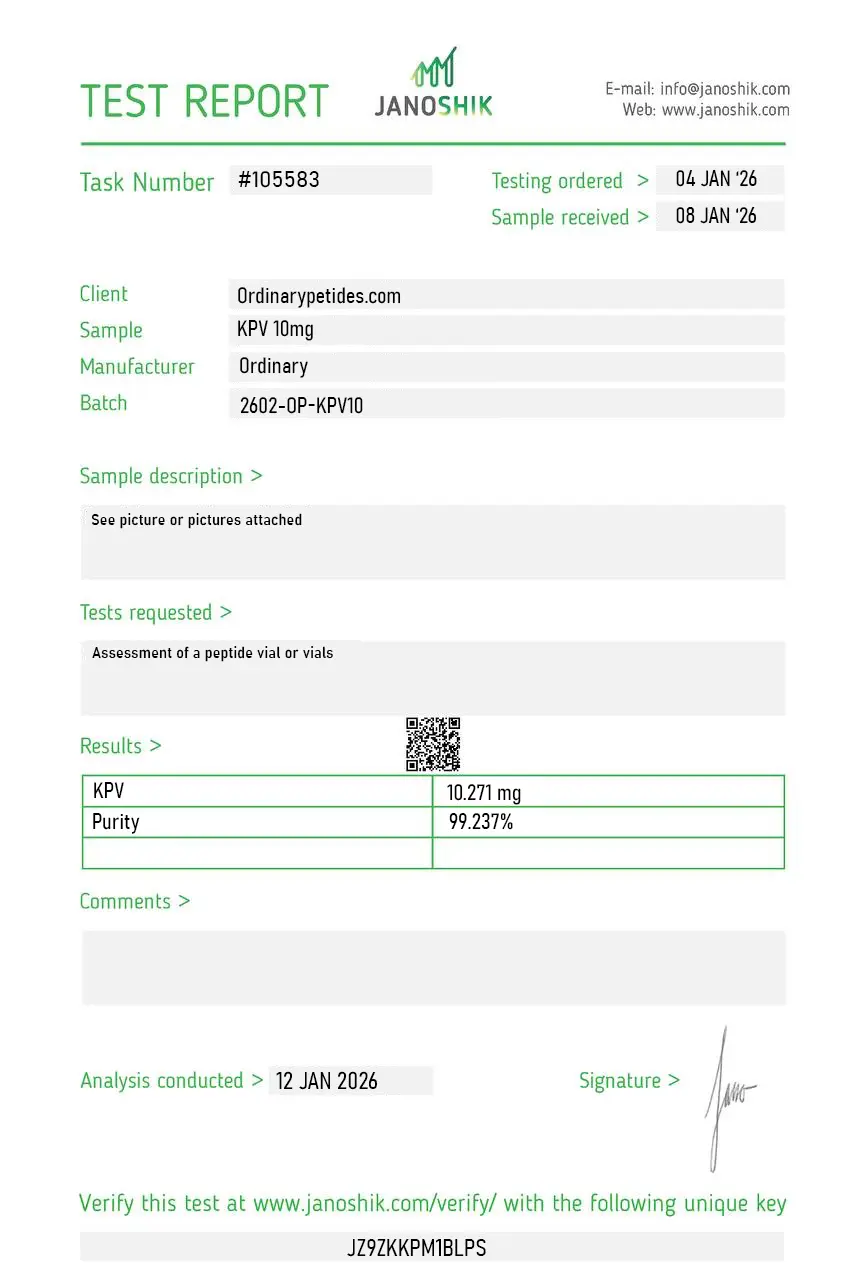
Certificate of Analysis
Independent test reports are available for KPV 5mg and KPV 10mg. These reports provide batch-level documentation and analytical verification information for research reference.
Three amino acids is about as small as a bioactive peptide gets, and that's the practical reason to source KPV from a research supplier rather than synthesize in-house — at this length, the cost-savings calculation for in-house Fmoc synthesis tips against doing it ourselves, especially for the small quantities we use. The material was clean by HPLC when we verified, and the simplicity of the sequence means there's not much that can go wrong synthetically.
The mechanism described on the listing was framed correctly — KPV is the α-MSH C-terminal fragment with anti-inflammatory activity that does NOT go through melanocortin receptors, which is the single most important pharmacological fact about it and the one most listings get wrong by lumping it with MC1R-MC5R compounds. Could be more explicit that the actual receptor or intracellular target for KPV's anti-inflammatory activity remains incompletely defined, so the buyer understands they're working with a mechanism-of-action question, not a settled answer.
As the chemical sequence Lys–Val–Pro, it exists as a tripeptide and can be synthesized; in the literature, it also appears in the context of food/soy bioactive peptides.
No. KVP is Lys–Val–Pro, whereas KPV is Lys–Pro–Val. The scientific base for KPV is much better.
In the available public selection, no convincing clinical data are visible; the topic appears mainly preclinical and review-level.
Because of interest in short PepT1-transportable peptides that may reduce inflammatory signaling in the intestine and immune cells.
On the basis of the available literature, it is more correct to say not "it is suitable," but "it is being studied as a potential anti-inflammatory candidate in the preclinical context of intestinal inflammation."
That without clarifying the sequence and the primary sources, discussion of KVP very easily slides into a discussion of KPV. And that is already a different topic.
KPV is a synthetic tripeptide consisting of just three amino acids — Lysine (K), Proline (P), and Valine (V) — representing the C-terminal sequence of alpha-melanocyte stimulating hormone (α-MSH). It was identified as the active anti-inflammatory fragment of α-MSH when researchers sought to isolate which portion of the full 13-amino acid neuropeptide was responsible for its immunomodulatory activity — and found that the final three C-terminal amino acids retained potent anti-inflammatory properties while stripping away the hormonal effects of the parent molecule, including melanogenesis and the broad receptor activations that produce tanning, appetite changes, and sexual effects seen with melanocortin agonists like Melanotan 2. This makes KPV mechanistically distinct from both the MT-1/afamelanotide and MT-2/bremelanotide compounds covered earlier in this series — it shares the α-MSH lineage but produces none of their receptor-mediated side effects. It is not FDA-approved, has no completed human clinical trials as a therapeutic agent, and is not legally compoundable in the United States.
KPV's mechanism operates through several complementary pathways that together constitute a well-characterized and genuinely novel anti-inflammatory profile. Its primary mechanism is direct intracellular NF-κB inhibition — KPV is small enough to enter cells and translocate to the nucleus where it directly interacts with and suppresses NF-κB, the master transcription factor governing expression of pro-inflammatory genes. This suppression reduces production of the key inflammatory cytokines TNF-α, IL-1β, and IL-6. Critically this mechanism is receptor-independent — unlike α-MSH which requires binding to melanocortin receptors to exert its effects, KPV acts directly inside cells, explaining why it works even in cell types with minimal melanocortin receptor expression. A published in vitro study confirmed that macrophage activation was inhibited by α-MSH and Melanotan II through cAMP-mediated MC receptor pathways, but not by KPV — confirming KPV uses a genuinely distinct intracellular mechanism rather than simply being a weaker version of its parent molecule. Beyond NF-κB inhibition, KPV promotes epithelial repair and barrier integrity in gut mucosa, activates anti-inflammatory pathways in keratinocytes through MC1R interaction, and has documented antimicrobial activity against Staphylococcus aureus and Candida albicans in laboratory studies — with one study showing over 90% MRSA killing within 15 minutes, though this finding has not been fully reproduced.
A pharmacologically unusual feature of KPV that distinguishes it from most peptides in this series is its documented oral bioavailability. Most peptides are destroyed by gastrointestinal proteases before reaching systemic circulation, requiring injection for therapeutic effect. KPV contains proline and valine in its sequence which provide natural resistance to common digestive enzymes. More importantly, it has been shown to be actively absorbed through the intestinal wall via PepT1 — a peptide transporter expressed throughout the gastrointestinal tract that normally handles di- and tripeptides from digested food proteins. This transporter-mediated uptake allows KPV to reach intestinal immune cells directly and in meaningful concentrations, making oral administration specifically appropriate for gut-targeted anti-inflammatory applications. A 2008 paper in Gastroenterology documented PepT1-mediated KPV uptake and its reduction of intestinal inflammation — one of the more rigorously documented pieces of evidence for oral peptide bioavailability in this entire series.
Published preclinical evidence is more focused and mechanistically coherent than many compounds in this series, though the total publication volume is modest — approximately 70 PubMed results spanning several decades. The strongest evidence base is in gut inflammation — multiple mouse colitis models have shown KPV administration significantly reduces inflammatory markers by approximately 50%, decreases pro-inflammatory cytokine production, protects intestinal tissue integrity, and reduces the incidence and severity of colitis. Topical wound healing research — including a corneal wound study in rabbits showing 100% wound closure versus 0% in controls with four daily topical applications — suggests potent pro-healing activity, though corneal tissue is not directly comparable to facial or body skin. Skin inflammation research in models of psoriasis, eczema, and contact dermatitis has shown KPV reduces keratinocyte hyperproliferation and inflammatory signaling. Systemically, animal studies have documented anti-inflammatory effects in peritonitis models and TNF-α downregulation.
KPV is used through three distinct routes depending on the target application. Oral capsules are the preferred route for gut-targeted inflammation — Crohn's disease, ulcerative colitis, irritable bowel syndrome — given the PepT1-mediated intestinal uptake. Subcutaneous injection is used for systemic anti-inflammatory applications, typically at doses of 200 to 500 mcg per day. Topical creams and gels are used for skin inflammatory conditions including acne, eczema, and psoriasis, though effective transdermal delivery requires addressing KPV's limited skin penetration — research shows standard cream formulations may not achieve meaningful subdermal concentrations without delivery-enhancing technologies such as microneedles or iontophoresis. Nanoparticle delivery systems for topical KPV have been studied in published research to improve stability and controlled release.
KPV has a consistently favorable safety profile across available preclinical evidence — one of the cleaner profiles in this series relative to its anti-inflammatory potency. Because it lacks melanocortin receptor agonist activity it produces none of the tanning, appetite suppression, libido changes, spontaneous erections, or mole darkening seen with melanocortin peptides. It does not suppress immune function broadly in the manner of corticosteroids — a key differentiation noted in published literature — making it potentially more suitable for conditions where infection and inflammation coexist. Injection site reactions including mild redness and irritation are occasionally reported. Mild gastrointestinal sensitivity including bloating has been noted in some oral administration studies at higher doses. People with mast cell activation syndrome or histamine intolerance may experience heightened sensitivity due to temporary shifts in cytokine patterns. Long-term human safety data does not exist.
People with active infections should exercise caution — while KPV does not broadly suppress immunity, its anti-inflammatory action could theoretically blunt beneficial inflammatory responses needed for infection resolution, despite its documented antimicrobial properties. People with autoimmune conditions should discuss with a physician before use given immune modulation effects. Pregnant or breastfeeding women should not use it given absent safety data. Anyone using immunosuppressive medications should be aware of potential additive immunomodulatory effects. It is not FDA-approved for any indication and cannot be legally compounded in the United States.