

KPV
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
KPV: A Tripeptide at the Crossroads of Anti-Inflammatory Research, Melanocortin Biology, and Mucosal Immunology
KPV, also known as Lys-Pro-Val, is a short tripeptide best known in the field of immunology, where it has been studied as the C-terminal fragment of alpha-melanocyte stimulating hormone (α-MSH) and linked to the biology of inflammation control. In the research context, the main interest in this peptide grew out of studies reporting NF-κB suppression, reduced TNF-α and IL-6 production, and attenuated cytokine signaling in cellular and animal models. That sounds dramatic — and that is precisely why it attracts so much attention.
Published reports have also discussed its relationship with mucosal immunity, intestinal inflammation, and PepT1-mediated uptake in colitis models, while preclinical data have connected it to a broader melanocortin-derived peptide framework, including effects on airway and skin inflammation. Still, a sober filter is essential here: a compelling anti-inflammatory story is not yet a ready-made therapy in a vial. If only biology were that cooperative.
What makes KPV genuinely interesting is that it sits at the crossroads of immune modulation, cytokine biology, and the older tradition of α-MSH–derived bioregulators. For readers who care not just about bold promises but about the actual scientific grounds for interest, this is exactly the kind of peptide worth examining carefully — and without illusions.
KPV: A Scientific Review of the Anti-Inflammatory Tripeptide
Based on peer-reviewed literature — see References. Last updated: May 2026.
The Short Version
KPV is the C-terminal tripeptide of α-melanocyte-stimulating hormone (α-MSH) — just three amino acids: lysine, proline, valine. By itself, this is one of the smallest peptides in the entire research-chemical landscape, and one of the chemically simplest. But the biology that hangs off this tiny molecule has turned out to be genuinely interesting, with a published evidence base that spans gastroenterology, dermatology, inflammation research, and oral peptide pharmacology going back over thirty years.
The promise is straightforward. α-MSH has well-established potent anti-inflammatory and immunomodulatory effects, but the full peptide is 13 amino acids long, signals through several melanocortin receptors (MC1R, MC3R, MC4R, MC5R), and produces a number of off-target effects including skin pigmentation, libido modulation, and effects on energy homeostasis. KPV retains most of α-MSH's anti-inflammatory activity while losing the melanocortin receptor binding entirely — it works through a different mechanism, with a much cleaner side-effect profile. And, unusually for such a small peptide, KPV is reported to be orally bioavailable through a specific intestinal transporter (PepT1).[1][2]
The complications, as usual, sit underneath the optimistic mechanism story.
First: while there is solid academic preclinical work on KPV from multiple independent groups — including Daniel Merlin's lab at Emory, which has published the most rigorous work on KPV-PepT1 interactions and inflammatory bowel disease applications — controlled human clinical trials are essentially absent. Some early Phase 2 work on broader α-MSH peptides occurred in the 1990s and 2000s, but for KPV specifically there is no completed Phase 2 or 3 trial that would support claims of clinical efficacy in humans.
Second: like BPC-157, KPV was placed on the FDA Category 2 bulk drug substance list in September 2023, alongside several other peptides. The same Pharmacy Compounding Advisory Committee review that will address BPC-157 in July 2026 will also examine the status of KPV. The outcome will affect compounding pharmacy access.[8]
Third: KPV's reported applications — inflammatory bowel disease, atopic dermatitis, oral mucositis, post-surgical wound healing — are real clinical needs, but they are also the kinds of conditions where placebo response is substantial and patient expectation effects on subjective outcomes (pain, symptom severity) are well-documented. The case for KPV's efficacy in humans rests almost entirely on extrapolation from animal data and uncontrolled case reports.
| At a glance | |
|---|---|
| Full name | Lysyl-prolyl-valine (Lys-Pro-Val) |
| Sequence | KPV (3 amino acids) |
| Molecular formula | C₁₆H₃₀N₄O₄ |
| Molecular weight | 342.4 Da |
| Origin | C-terminal tripeptide of α-melanocyte-stimulating hormone (α-MSH, amino acids 11–13) |
| Primary target | Intracellular anti-inflammatory pathways (NF-κB inhibition); IL-1β/IL-6 signaling modulation; transported into cells via PepT1 (SLC15A1) |
| Does NOT bind | Melanocortin receptors (MC1R/MC3R/MC4R/MC5R) |
| Oral bioavailability | Yes — via PepT1 transport (independent of receptor binding) |
| FDA status | ⚠️ Category 2 bulk drug substance (September 2023) |
| EMA status | ❌ Not approved |
| WADA status | Not specifically named on the 2026 Prohibited List |
| Human clinical trials | ❌ No completed Phase 2 or 3 trials for any major indication |
The α-MSH Connection
The parent molecule
α-Melanocyte-stimulating hormone (α-MSH) is a 13-amino-acid neuropeptide produced primarily by post-translational cleavage of pro-opiomelanocortin (POMC) in the pituitary, central nervous system, and several peripheral tissues. Sequence: SYSMEHFRWGKPV. The peptide has been known and studied since the 1950s for its role in melanocyte regulation (hence the name — α-MSH binding to MC1R on melanocytes drives melanin production and pigmentation).
What became apparent through the 1980s and 1990s is that α-MSH does far more than control pigmentation. It has potent and broadly characterized anti-inflammatory and immunomodulatory effects in essentially every tissue where it has been examined. The peptide downregulates pro-inflammatory cytokine production, inhibits NF-κB activation, attenuates inflammatory cell migration, and protects tissues against a wide range of injury contexts.[1]
Why use a tripeptide instead of the full peptide
α-MSH's broader pharmacology — particularly its binding to multiple melanocortin receptors — creates clinical problems for systemic use. MC1R activation causes skin and hair pigmentation. MC3R and MC4R activation affects energy balance, appetite, and libido. MC5R is involved in sebaceous gland regulation. For an anti-inflammatory indication, all of these are off-target effects.
In the 1990s, several groups began investigating which parts of the α-MSH sequence were responsible for which effects. The melanocortin receptor binding was localized to the central core sequence (HFRWG, the “message” sequence). The anti-inflammatory activity, perhaps surprisingly, was largely preserved in the C-terminal tripeptide alone: KPV.[2]
The result is an unusual situation: a fragment of a hormone retains most of the parent's most clinically useful activity (anti-inflammation) while losing essentially all of its receptor-mediated side effects. KPV does not bind melanocortin receptors. It works through a different intracellular pathway. The decoupling is what makes the molecule pharmacologically attractive.
Chemistry
KPV is structurally about as simple as a research peptide gets. Three amino acids, all standard L-amino acids, no modifications, no D-substitutions, no cyclization. The N-terminus is the basic amine of lysine; the C-terminus is the carboxyl of valine. Molecular weight 342.4 Da.
The simplicity has consequences for stability. KPV is reasonably stable in solution at neutral pH but, like most short linear peptides, is susceptible to proteolytic cleavage by endo- and aminopeptidases. The plasma half-life is short — estimates in animal studies suggest minutes to a few hours, depending on route of administration. The compound is typically administered to maintain effect either by frequent dosing or by routes (intranasal, topical, intracolonic) that target tissue locally and minimize the need for sustained plasma levels.
| Property | Detail |
|---|---|
| Length | 3 amino acids |
| Molecular weight | 342.4 Da |
| Charge at physiological pH | Net positive (lysine side chain protonated) |
| Solubility | Highly water-soluble |
| Stability in solution (neutral pH) | Reasonable; degradable by peptidases |
| Plasma half-life | Short (minutes to hours, depending on conditions) |
| Oral bioavailability | Yes, via PepT1 transporter |
| Routes used in research | Oral, intranasal, topical, intracolonic, subcutaneous, IP |
Proposed Mechanisms of Action
1. PepT1-mediated cellular uptake
This is one of the most pharmacologically distinctive features of KPV. The peptide transporter PepT1 (SLC15A1) is a proton-coupled oligopeptide transporter primarily expressed on the apical surface of intestinal epithelial cells, but also expressed on inflamed colonic epithelium, immune cells (particularly macrophages and neutrophils during inflammation), and other tissue cells under inflammatory conditions.
KPV is a substrate for PepT1, which means it can be transported into cells expressing this transporter — including the inflamed epithelium of patients with inflammatory bowel disease, where PepT1 expression is upregulated. The result is that orally administered KPV can be selectively delivered into inflamed tissue while passing through healthy tissue more passively. Daniel Merlin's group at Emory University has done substantial work characterizing this selectivity.[3] Further context on this research direction is available in the inflammation research category.
2. NF-κB pathway inhibition
Once inside the cell, KPV inhibits the activation of NF-κB, a master transcription factor that drives the expression of pro-inflammatory cytokines (TNF-α, IL-6, IL-1β, IL-8), chemokines, and adhesion molecules. The exact molecular mechanism by which KPV inhibits NF-κB is not fully resolved, but the phenotypic effect is well-documented across multiple cell types and inflammation models.[4]
3. Cytokine modulation
Downstream of NF-κB inhibition, KPV reduces the secretion of pro-inflammatory cytokines, particularly IL-1β, IL-6, and TNF-α, while preserving (and in some contexts enhancing) anti-inflammatory cytokines like IL-10. This shifts the local cytokine milieu from pro-inflammatory to resolution-supporting.
4. Antimicrobial effects
KPV has been reported to have direct antimicrobial activity against certain pathogens, including Staphylococcus aureus and Candida albicans. This is mechanistically distinct from the anti-inflammatory effects and may contribute to the wound-healing and skin-infection applications.
5. Mast cell stabilization
In some inflammation models, KPV reduces mast cell degranulation, contributing to its potential utility in allergic and hypersensitivity contexts.
| Proposed mechanism | Evidence type | Independence |
|---|---|---|
| PepT1 transport into inflamed cells | Cell culture + mouse models | ✅ Multiple groups (Merlin, others) |
| NF-κB inhibition | Cell culture + animal | ✅ Multiple groups |
| Reduced IL-1β, IL-6, TNF-α | Cell culture + animal | ✅ Multiple groups |
| Antimicrobial activity | In vitro | ✅ Independent reports |
| Mast cell stabilization | In vitro + animal | Limited independent |
| Does NOT bind melanocortin receptors | Binding assays | ✅ Established |
| Specific intracellular receptor | — | ❌ Not identified |
Preclinical Evidence
Inflammatory bowel disease models (the strongest dataset)
The Merlin group at Emory University has published the most rigorous preclinical work on KPV in IBD models. Key findings:
- Oral KPV reduces disease severity in DSS-induced colitis in mice
- The effect requires PepT1 expression in intestinal epithelium
- Reduced inflammatory cell infiltration into colonic tissue
- Reduced colonic IL-6, IL-1β, TNF-α expression
- Preserved epithelial barrier function
- Effective at very low oral doses (μg-range)
This is among the more compelling preclinical datasets for an inflammation peptide, in part because of the PepT1-mediated selectivity for inflamed tissue.[3][4]
Atopic dermatitis and skin inflammation
Topical KPV has been studied in animal models of atopic dermatitis and contact dermatitis. Reported effects include reduced ear swelling, decreased epidermal thickening, and lower inflammatory infiltrate. The compound's small size and topical bioavailability make it potentially attractive for dermatological applications.[5]
Oral mucositis
KPV has been investigated for chemotherapy-induced oral mucositis in animal models, with reported beneficial effects on lesion severity and healing time.
Wound healing
Multiple animal studies have reported accelerated wound closure and reduced inflammatory phase duration with KPV treatment.
Asthma and allergic inflammation
Some animal data on allergic airway inflammation suggests KPV reduces eosinophil infiltration and airway hyperresponsiveness. The data are less mature than for IBD.
Human Evidence
This is the weakest part of the KPV story.
The α-MSH family of peptides has been studied in humans in some contexts — bremelanotide (PT-141, a synthetic α-MSH analog) was eventually approved by the FDA for hypoactive sexual desire disorder; afamelanotide (an α-MSH analog) is approved for erythropoietic protoporphyria. But these are different molecules with different pharmacology, and their development paths do not directly inform KPV's clinical status.
For KPV specifically:
- No completed Phase 2 trial for any major indication has been published.
- Some early-phase work on broader α-MSH-derived peptides in inflammation occurred in the 1990s/2000s, but the KPV-specific clinical development pathway is largely absent.
- Anecdotal case reports and case series from compounding pharmacy use in autoimmune, dermatological, and gastroenterological contexts exist in non-indexed literature.
- No head-to-head comparison with standard treatments (corticosteroids, biologics, etc.) has been done in any controlled setting.
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) | ⚠️ Category 2 bulk drug substance (September 2023); PCAC review pending |
| Compounding pharmacies (US) | Cannot be legally compounded under 503A pending review |
| EMA (Europe) | ❌ Not approved |
| WADA | Not specifically named on the 2026 Prohibited List |
The Category 2 placement, like BPC-157's, reflects insufficient safety and efficacy data rather than a finding of established harm. The same general regulatory caution applies. The future of US compounding pharmacy access to KPV will be substantially shaped by the upcoming PCAC reviews.[8]
Safety
Animal safety
Across the preclinical literature, KPV has been reported to be well-tolerated in rodents at doses producing efficacy, across oral, topical, and parenteral routes. No major organ toxicity, no behavioral toxicity, no consistent adverse effect signal. The very small size of the peptide and its rapid clearance reduce the theoretical surface for systemic adverse effects.
Human safety
Limited. The available human safety data for KPV specifically is fragmentary — small uncontrolled studies, anecdotal compounding pharmacy use, no large controlled safety cohort. The broader α-MSH peptide family has been used clinically in some contexts with generally acceptable safety profiles, but extrapolation from one peptide to another in this family is not straightforward.
The cancer question
Worth flagging: KPV's anti-inflammatory mechanism is general (NF-κB inhibition) and does not specifically target oncogenic pathways. Unlike BPC-157 (VEGF) or 5-Amino-1MQ (NNMT), KPV does not have a strong mechanistic linkage to cancer biology pathways that would raise specific oncological concerns. This is a meaningful difference within the inflammation/regenerative peptide class.
That said, chronic broad anti-inflammatory effects in healthy tissue could theoretically have consequences for tumor surveillance (the immune system's ability to identify and eliminate transformed cells is partly inflammation-dependent). This is a general concern for any chronic anti-inflammatory therapy and is not specific to KPV.
Other unknowns
- Long-term safety in healthy users. Not characterized.
- Immunogenicity. Theoretical concern for any synthetic peptide with chronic exposure; not specifically studied for KPV.
- Drug interactions. Not characterized.
- Pregnancy and reproductive effects. Not studied; contraindicated by default.
- Effects on infection susceptibility. Chronic anti-inflammatory effects could theoretically affect host defense; not specifically studied at chronic systemic doses.
- Vendor material quality. Standard research-chemical caveats apply.
| Safety area | Status |
|---|---|
| Acute animal toxicity | ✓ No signal at tested doses |
| Subchronic animal toxicity | ✓ No reported issues |
| Limited acute human safety | ⚠️ Limited data; no major adverse events reported |
| Long-term human safety | ❌ Not characterized |
| Direct cancer mechanism concern | ✓ Less concerning than VEGF-acting peptides |
| Effects on infection surveillance | ⚠️ Theoretical concern with chronic systemic use |
| Pregnancy/lactation | ❌ Contraindicated by default |
| Vendor material quality | ⚠️ Variable |
Common Misconceptions
"KPV is α-MSH."
It is not. KPV is the C-terminal tripeptide of α-MSH (positions 11–13). The two molecules have different pharmacology: α-MSH binds melanocortin receptors and produces pigmentation and energy-balance effects; KPV does not bind melanocortin receptors and works through a different intracellular mechanism. The shared anti-inflammatory effect is real, but the molecules are pharmacologically distinct.
"It causes tanning like Melanotan."
It does not. Melanotan I and II are MC1R agonists. KPV does not bind MC1R or any other melanocortin receptor. The compound does not produce skin pigmentation effects.
"Oral KPV works the same as injectable."
This is partially true but contextual. Oral KPV is transported by PepT1, which is selectively expressed on inflamed gut epithelium. For gut inflammation, oral KPV has a real mechanistic advantage in tissue targeting. For systemic anti-inflammatory effects in other tissues, the comparative bioavailability and efficacy of oral versus parenteral KPV is less well-characterized.
"It's been used in IBD trials with positive results."
The IBD work on KPV is primarily preclinical. There is no completed Phase 2 randomized controlled trial in IBD that has been published in major journals. The mechanistic case is interesting; the clinical efficacy claim outpaces the controlled human evidence.
"It's safe because it's such a small peptide."
Small size reduces some kinds of risk (lower theoretical immunogenicity, faster clearance) but does not eliminate safety considerations. The chronic systemic anti-inflammatory effect of KPV, regardless of molecular size, is a pharmacological action with consequences worth understanding.
Frequently Asked Questions
Why is KPV on FDA Category 2?
The September 2023 Category 2 placement reflects the FDA's assessment that available safety and efficacy data on KPV for compounding pharmacy use are insufficient. The placement was part of a broader regulatory action that included BPC-157 and several other peptides. The placement is not a finding of established harm; it reflects insufficient data.[8]
Will the upcoming PCAC review affect KPV access?
The PCAC reviews scheduled for 2026 will examine the status of multiple Category 2 peptides including BPC-157 and KPV. The outcomes will affect compounding pharmacy access. Research-chemical market access operates outside the compounding framework and would not be directly affected by PCAC decisions.
How does KPV compare to corticosteroids for inflammation?
This comparison has not been done in controlled human trials. Mechanistically, KPV and corticosteroids both inhibit NF-κB but through different upstream pathways. Corticosteroids have substantial systemic side effects (osteoporosis, weight gain, glucose dysregulation, adrenal suppression) that KPV does not appear to produce in animal studies. Whether this safety advantage translates to humans at clinically meaningful doses is unknown.
Is it safe to take KPV long-term?
Unknown. No long-term human safety data exist. Chronic anti-inflammatory effects in healthy tissue could theoretically have consequences (effects on infection surveillance, tumor surveillance) that the available data cannot rule in or out.
What other peptides are commonly compared to KPV?
For gut-targeted inflammation, BPC-157 is the most frequent comparison — though the mechanisms are quite different (BPC-157 emphasizes growth factor/angiogenic effects; KPV emphasizes NF-κB and cytokine modulation). For broader immunomodulation, peptides like Thymosin Alpha-1 and Thymalin are sometimes discussed together — though again the mechanisms differ substantially.
Key Takeaways
- KPV is the C-terminal tripeptide of α-melanocyte-stimulating hormone (α-MSH). It retains most of α-MSH's anti-inflammatory activity while losing all melanocortin receptor binding — an unusual and clinically attractive pharmacological profile.[1][2]
- The mechanism is well-characterized: PepT1-mediated cellular uptake (with selectivity for inflamed tissue), NF-κB pathway inhibition, reduced pro-inflammatory cytokine production, and antimicrobial effects.
- The preclinical evidence base is broader and more diverse than for many peptides in this review series, with independent group contributions (Merlin lab at Emory, others) particularly in inflammatory bowel disease models.[3][4]
- Oral bioavailability via PepT1 is a genuinely useful pharmacological feature, particularly for gut-targeted inflammation, and is unusual for a tripeptide.
- ⚠️ Controlled human clinical evidence is essentially absent. No completed Phase 2 or 3 trial for any major indication has been published. Use in humans relies on extrapolation from animal data and uncontrolled case reports.
- ⚠️ FDA Category 2 designation (September 2023) places KPV in the same regulatory situation as BPC-157. The upcoming PCAC reviews will shape compounding pharmacy access.[8]
- Unlike BPC-157 (VEGF) or 5-Amino-1MQ (NNMT), KPV does not have a strong mechanism-based linkage to cancer biology pathways. This is a meaningful safety difference within the inflammation peptide class — though chronic anti-inflammatory effects of any kind have general theoretical considerations for tumor and infection surveillance.
- The compound is sold through research-chemical channels with no GMP-grade quality guarantees. Material identity, purity, and dose accuracy cannot be assumed from vendor labeling.
- Honest framing: KPV is one of the more pharmacologically interesting research peptides currently available. The mechanism is coherent, the preclinical evidence has independent contributions, and the side effect profile (in animals, at least) appears clean. But the controlled human evidence base is still essentially preclinical, and the regulatory landscape is becoming more restrictive. The science merits continued investigation; the case for established human therapeutic use has not been made.
Related Compounds
For other compounds investigated in inflammation, gut healing, and immunomodulation contexts, see the Inflammation Research category. Closely related companions in this space include the regenerative pentadecapeptide BPC-157 (the other Category 2 gut-healing peptide most often discussed alongside KPV), and the thymic immunomodulators Thymosin Alpha-1 and Thymalin. For the broader immunology landscape, see the Immunology Research category.
References
α-MSH and KPV foundational work
- Brzoska T, Luger TA, Maaser C, Abels C, Böhm M. Alpha-melanocyte-stimulating hormone and related tripeptides: biochemistry, antiinflammatory and protective effects in vitro and in vivo, and future perspectives for the treatment of immune-mediated inflammatory diseases. Endocr Rev. 2008;29(5):581–602.
- Hiltz ME, Lipton JM. Antiinflammatory activity of a COOH-terminal fragment of the neuropeptide alpha-MSH. FASEB J. 1989;3(11):2282–2284.
Merlin group and PepT1 work
- Dalmasso G, Charrier-Hisamuddin L, Nguyen HT, et al. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology. 2008;134(1):166–178.
- Kannengiesser K, Maaser C, Heidemann J, et al. Melanocortin-derived tripeptide KPV has anti-inflammatory potential in murine models of inflammatory bowel disease. Inflamm Bowel Dis. 2008;14(3):324–331.
Dermatology and other applications
- Mastrofrancesco A, Kokot A, Eberle A, et al. KdPT, a tripeptide derivative of alpha-melanocyte-stimulating hormone, suppresses IL-1 beta-mediated cytokine expression and signaling in human sebocytes. J Immunol. 2010;185(3):1903–1911.
- Various publications on KPV in oral mucositis, wound healing, and skin inflammation contexts, 2000s–2020s.
α-MSH family in humans (context)
- Bremelanotide (PT-141, FDA-approved 2019); afamelanotide (FDA-approved 2019). These are pharmacologically distinct from KPV but illustrate clinical development paths within the broader α-MSH peptide family.
Regulatory
- FDA. Certain Bulk Drug Substances Used in Compounding Under Section 503A — Category 2 list (September 2023; includes KPV alongside BPC-157 and several other peptides). PCAC formal reviews scheduled 2026.
Key investigators
- Daniel Merlin, PhD — Emory University School of Medicine. Principal investigator on KPV-PepT1 interactions and IBD applications.
- Thomas A. Luger, MD — University of Münster. Long-time investigator of α-MSH and KPV in dermatology and inflammation.
- James M. Lipton, PhD (deceased) — UT Southwestern. Foundational work on α-MSH C-terminal fragment anti-inflammatory activity.
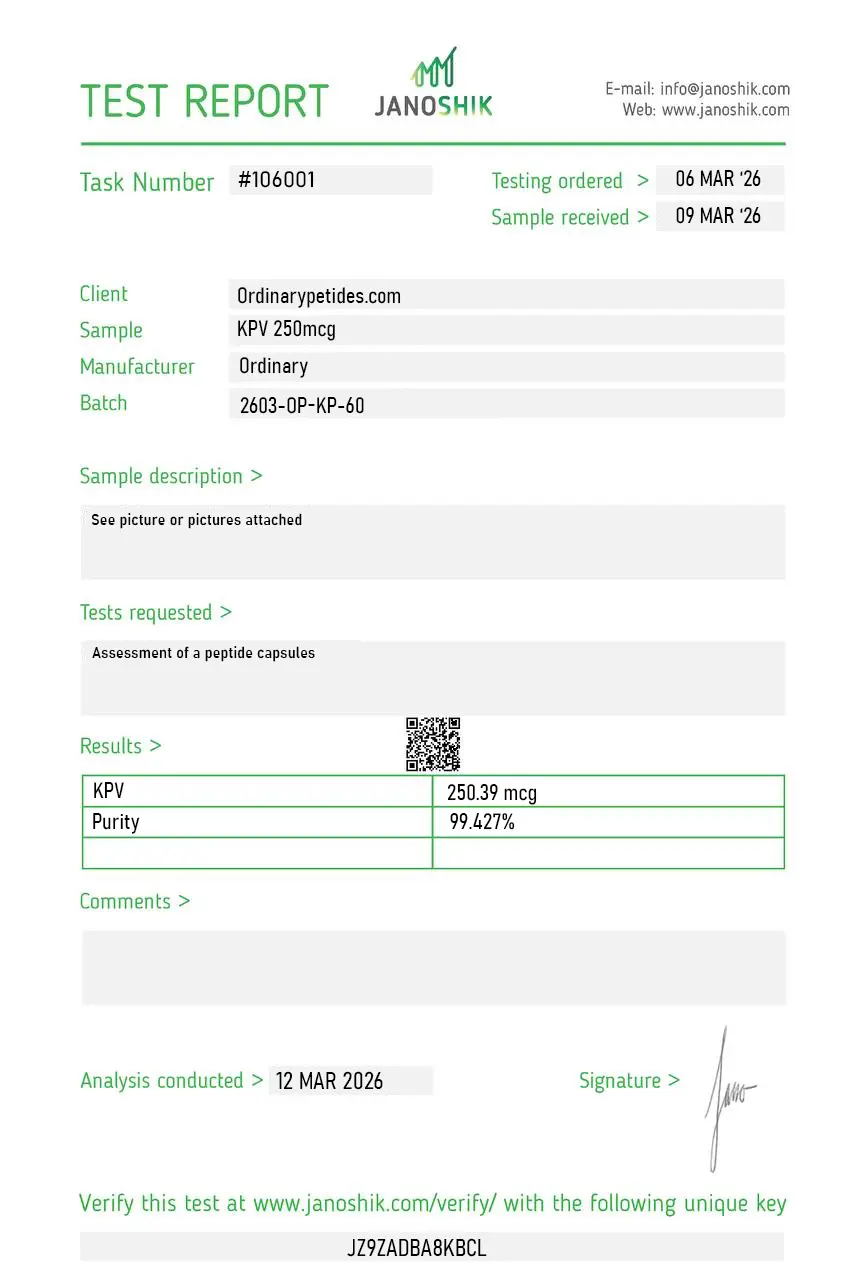
Certificate of Analysis
An independent test report is available for KPV 250mcg. This report provides batch-level documentation and analytical verification information for research reference.
KPV (lysine-proline-valine) is a synthetic tripeptide — a chain of just three amino acids — derived from the C-terminal region of alpha-melanocyte-stimulating hormone (α-MSH), a 13-amino acid neuropeptide produced primarily in the pituitary gland. Researchers identified that this short C-terminal fragment preserves much of α-MSH's anti-inflammatory activity while being significantly smaller, more chemically stable, and easier to deliver than the full-length parent molecule. Its small size and aqueous solubility have made it a subject of research into inflammatory conditions where larger biologics or conventional immunosuppressants carry significant systemic risks.
Alpha-MSH is a pleiotropic neuropeptide with well-documented roles in pigmentation regulation, appetite control, fever suppression, and immune modulation. It exerts anti-inflammatory effects primarily through interactions with melanocortin receptors — particularly MC1R and MC3R in peripheral immune tissues — acting as an endogenous counter-regulatory signal that limits the magnitude of immune activation in response to inflammatory stimuli. KPV is the C-terminal tripeptide fragment of α-MSH. Critically, research has established that KPV does not bind melanocortin receptors in the same way as its parent molecule — it does not activate MC1R and therefore does not produce pigmentation effects such as skin darkening. This receptor-independence was confirmed in studies showing KPV retained full anti-inflammatory activity in mice with nonfunctional MC1R receptors.
KPV's anti-inflammatory activity operates through two interconnected intracellular pathways. First, it inhibits NF-κB (nuclear factor-kappa B) — the central transcription factor governing inflammatory gene expression. By blocking NF-κB activation, KPV reduces downstream production of pro-inflammatory cytokines including TNF-α, IL-1β, and IL-6. Second, it suppresses the ERK/p38 MAPK (mitogen-activated protein kinase) signaling cascade. A 2025 study published in Toxicology confirmed that KPV inhibits the ERK/p38 MAPK/NF-κB axis and caspase-1 activation driven by reactive oxygen species (ROS) in human keratinocytes. A mechanistically significant feature is that KPV achieves this intracellular action not through surface receptor binding but through direct cellular uptake via the PepT1 transporter.
PepT1 (peptide transporter 1, SLC15A1) is a proton-coupled di/tripeptide transporter normally expressed in the small intestinal epithelium. It has high affinity for KPV — a Km of approximately 160 µM, among the lowest reported for any PepT1 substrate — allowing efficient cellular uptake. The critical research finding is that PepT1 expression is markedly upregulated in the colon during intestinal inflammation. This creates a tissue-selective uptake mechanism: inflamed gut tissue actively increases its capacity to absorb KPV, meaning the compound preferentially accumulates in the precise tissue compartments where inflammation is most active. This was confirmed mechanistically by Viennois et al. (2016) in Cellular and Molecular Gastroenterology and Hepatology, where KPV had no protective effect in PepT1-knockout mice, definitively establishing that PepT1 transport is required for its anti-inflammatory activity in the gut.
The landmark study by Dalmasso et al. (2008), published in Gastroenterology, demonstrated that PepT1-mediated uptake of KPV significantly reduced intestinal inflammation in both DSS (dextran sulfate sodium) and TNBS (trinitrobenzene sulfonic acid) induced colitis models in mice. Orally administered KPV reduced loss of body weight, colonic myeloperoxidase (MPO) activity, histological signs of inflammation, and pro-inflammatory cytokine mRNA levels. The 2016 Viennois study extended these findings by showing KPV prevented colitis-associated carcinogenesis in wild-type mice. A 2024 study in Frontiers in Pharmacology demonstrated that KPV combined with FK506 (tacrolimus) in PepT1-targeted nanoparticles improved body weight, colon length, and disease activity index while reducing TNF-α, IL-1β, and IL-6 in both acute and chronic colitis models — pointing toward potential combination therapeutic strategies.
KPV has been studied in dermatological research models for several reasons. The melanocortin system is expressed in skin-resident immune cells, keratinocytes, and fibroblasts — tissues directly relevant to inflammatory skin conditions including eczema, psoriasis, and wound healing. A 2025 study published in a peer-reviewed toxicology journal investigated KPV's protective effects against fine particulate matter (PM10)-induced oxidative damage and inflammation in human HaCaT keratinocytes, finding that KPV inhibited the MAPK/NF-κB pathway and reduced ROS-driven IL-1β production. Earlier research characterized KPV's ability to reduce pro-inflammatory cytokine secretion in skin immune cells. Transdermal delivery has also been studied — a 2017 paper in the Journal of Pharmaceutical Sciences examined iontophoretic delivery of KPV across microporated human skin as a potential topical delivery route for inflammatory dermatological conditions.
Yes. Research published in the Journal of Leukocyte Biology (2000) found that KPV — alongside broader α-MSH activity — demonstrated antimicrobial effects against Staphylococcus aureus and Candida albicans at nanomolar concentrations, both killing pathogens and reducing their viability. The researchers specifically noted that many anti-inflammatory drugs reduce immune function, whereas KPV's dual anti-inflammatory and antimicrobial action was preserved simultaneously. This combination has been identified as particularly relevant for wound healing research contexts, where controlling both infection and excessive inflammation are concurrent challenges. This antimicrobial activity is thought to be independent of the NF-κB pathway and represents a mechanistically distinct aspect of KPV's profile.
Conventional corticosteroids and broad-spectrum immunosuppressants exert anti-inflammatory effects by globally suppressing immune function, carrying well-documented risks including immunosuppression, adrenal suppression, and systemic metabolic effects. KPV's mechanism is more targeted: it modulates NF-κB and MAPK signaling pathways in inflamed tissue without broadly shutting down immune function. Preclinical research has described its anti-inflammatory effects as comparable in magnitude to corticosteroids in specific models while preserving fundamental immune responses. The PepT1-dependent tissue-selective accumulation in inflamed gut tissue also suggests a degree of anatomical targeting not achievable with conventional systemically distributed drugs. Researchers consistently frame KPV as an immune modulator rather than an immunosuppressant.
Beyond the gut and skin, KPV's anti-inflammatory mechanism has been studied in human bronchial epithelial cells. A PMC-published study (Land, 2012) examined KPV's inhibition of inflammatory signaling in bronchial epithelium, finding that it disrupts NF-κB-mediated inflammatory signaling and notably suppresses matrix metalloproteinase (MMP) activity — a family of proteases with major roles in immune signaling and tissue remodeling in inflammatory and cancerous lung diseases. The study also noted that because KPV's actions appear not to be receptor-mediated, its structure may be modifiable to improve targeting toward specific pathways, and its small size and aqueous solubility make nebulized delivery to the lung a feasible research direction. This extends the potential research applications of KPV well beyond gastrointestinal and dermatological models.
KPV does not have FDA approval for any clinical indication. It is available as a Research Use Only (RUO) compound. A review scheduled for July 2026 by the FDA is noted in recent literature as a relevant regulatory milestone for the compound. The existing evidence base is almost entirely preclinical — derived from animal models and human cell culture experiments. No completed randomized controlled trials in humans have been published. Key gaps that researchers identify include: the absence of pharmacokinetic data in humans (bioavailability, half-life, tissue distribution across non-gut compartments), no systematic evaluation of long-term safety at varying exposures, limited independent replication of gut findings in non-murine models, and no established delivery system optimized for clinical translation. The mechanistic rationale is considered strong and the preclinical data consistent, but the compound sits at an early translational stage awaiting human trial data to substantiate the animal evidence.