



NAD+
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
NAD+: Not a Peptide, but a Big Deal in Cell Biology
NAD+ is not a peptide, but a coenzyme without which cellular energetics, DNA repair, and the function of a range of NAD+-dependent enzymes simply do not add up into a normal biological picture. That is exactly why there is so much interest in it in the research context: in preclinical models, boosting NAD+ metabolism has often been linked to more favorable metabolic and stress-adaptive outcomes.
But the whole point lies in an honest formulation: the biochemical importance of NAD+ does not automatically equal a proven "anti-aging effect" in humans. In the published human data, NAD+ precursors have more often shown increases in NAD+-related metabolites, whereas clinical effects on well-being, aging, and performance have remained far less clear-cut — and for IV NAD+ the evidence base looks especially limited.
That is why NAD+ is compelling not as a "magic drip," but as one of the most fundamental molecules in modern metabolic science. For the client, the interest here is not about loud promises, but about genuinely strong biology — a space where the science is already highly intriguing, while the marketing still likes to run ahead of the evidence.
NAD+ (Nicotinamide Adenine Dinucleotide): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
NAD+ is unlike anything else in this series. Every other compound covered here is being administered in an attempt to replicate, amplify, or restore a specific signalling molecule. NAD+ is the underlying metabolic infrastructure that all of those signalling systems depend on. It is not a growth factor, a neuropeptide, or a metabolic hormone. It is the universal currency of electron transfer in living cells — present in every cell of every organism from bacteria to humans, participating in hundreds of enzymatic reactions simultaneously.
What makes NAD+ relevant to this series is a convergence discovered over the past 25 years: beyond its classical role as an electron carrier, NAD+ is also consumed as a substrate by three families of signalling enzymes — sirtuins, PARPs, and CD38. These NAD+-consuming enzymes are central to DNA repair, gene regulation, inflammation, and cellular stress response. When NAD+ levels fall, so does the activity of these regulatory systems. And NAD+ levels do fall — measurably, reproducibly, and substantially with age. Tissue NAD+ may be 50% of youthful levels by age 50, with continued decline thereafter.
Oral precursors reliably raise blood NAD+ levels in humans. Whether that rise translates to meaningful clinical benefits is the central unresolved question: the answer appears to be “sometimes yes, in specific populations” rather than “yes universally.”
| At a glance | |
|---|---|
| Full name | Nicotinamide adenine dinucleotide |
| What it is | Universal electron-carrying coenzyme; present in all living cells |
| Oxidised/reduced forms | NAD&sup+; (oxidised, electron acceptor) ↔ NADH (reduced, electron donor) |
| Key consuming enzymes | Sirtuins (SIRT1–7), PARPs, CD38/CD157 |
| Rate-limiting biosynthetic enzyme | NAMPT (nicotinamide phosphoribosyltransferase) |
| Age-related decline | ~50% by age 50; up to 90% by age 80 in some tissues |
| Primary driver of age decline | CD38 upregulation (proven in mice; strong human correlate) [2] |
| Main precursor supplements | NMN (nicotinamide mononucleotide), NR (nicotinamide riboside) |
| FDA status | NAD+ precursors sold as dietary supplements; NMN FDA status under review |
| Best human evidence | NMN improves muscle insulin sensitivity in prediabetic postmenopausal women (Yoshino et al., Science 2021) [4] |
What NAD+ Does: The Two Roles
Role 1: Electron carrier in metabolism
In the oxidised form (NAD+), it accepts electrons — specifically hydride ions (H&sup-;) — from metabolic substrates, becoming NADH. The electrons are then donated to the mitochondrial electron transport chain, driving ATP synthesis. This redox cycling happens hundreds of times per second in every living cell: in glycolysis, the Krebs cycle (three NAD+-reducing steps per acetyl-CoA unit), and the electron transport chain where NADH donates its electrons at Complex I. Without sufficient NAD+, these pathways stall. This is not theoretical — the vitamin B3 deficiency disease pellagra is caused by deficient niacin (a NAD+ precursor), and its neurological and metabolic symptoms reflect NAD+ insufficiency at clinically meaningful scale.
Role 2: Co-substrate for signalling enzymes
NAD+ also plays an important role in the regulation of NAD+-consuming enzymes, including sirtuins, poly-ADP-ribose polymerases (PARPs), and CD38/157 ectoenzymes. In these reactions, NAD+ is consumed: the nicotinamide ring is cleaved, releasing nicotinamide and leaving an ADP-ribose group that is transferred to substrate proteins. Because these enzymes consume NAD+ rather than recycle it, they impose ongoing demand on cellular NAD+ pools that competes with the redox cofactor function.
Sirtuins (SIRT1–SIRT7): NAD+-dependent deacylases and deacetylases that regulate gene expression by removing acetyl groups from histones and transcription factors. SIRT1 deacetylates p53, NF-κB, and PGC-1α — controlling stress responses, inflammation, and mitochondrial biogenesis. When NAD+ falls, sirtuin activity falls proportionally.[1] PARPs: Add ADP-ribose chains to proteins at sites of DNA damage. PARP1 is the dominant consumer of NAD+ under DNA damage conditions — protective acutely but problematic chronically as DNA damage accumulates with age. CD38: A NADase whose expression increases substantially with age and inflammation, degrading not only NAD+ directly but also NMN — reducing both the current pool and the precursor supply for future synthesis.[2]
Why NAD+ Declines with Age
1. CD38 upregulation (the dominant mechanism)
At 32 months, wild-type mice had about half the NAD+ of a young mouse, but the CD38 knockout showed no decrease. Expression and activity of the NADase CD38 increase with aging and CD38 is required for the age-related NAD decline and mitochondrial dysfunction via a pathway mediated at least in part by regulation of SIRT3 activity.[2] What drives CD38 upregulation? Senescent cells and the inflammatory SASP (senescence-associated secretory phenotype) they secrete. As the body accumulates senescent cells with age, resulting chronic inflammation drives CD38 upregulation, which drives NAD+ depletion, which impairs sirtuin-mediated DNA repair and stress responses, which promotes further senescence — a self-amplifying cycle.
2. PARP overactivation from DNA damage
As DNA damage accumulates with age, PARP1 becomes chronically more active. Treatment of old mice with PARP inhibitors or precursors to NAD+ can greatly improve health, including increased insulin sensitivity, reversal of mitochondrial dysfunction, reduced stem cell senescence, and extension of lifespan.[3]
3. NAMPT decline
NAMPT (nicotinamide phosphoribosyltransferase) is the rate-limiting enzyme in the salvage pathway — the main route of NAD+ biosynthesis in mammals. NAMPT expression declines with age in some tissues (white adipose tissue, skeletal muscle), reducing the capacity to regenerate NAD+. This reduced biosynthetic capacity compounds the increased consumption from CD38 and PARPs.
NAD+ Biosynthesis: The Pathways and Precursors
The salvage pathway (dominant in most tissues)
Nicotinamide (NAM) — the breakdown product of NAD+-consuming enzymes — is recycled back to NMN by NAMPT, then NMN → NAD+ by NMNAT. This pathway is the primary NAD+ maintenance route and the one most relevant to supplementation: NMN enters the pathway directly as the penultimate intermediate, bypassing the NAMPT bottleneck. NR (nicotinamide riboside) is phosphorylated by NRK1/NRK2 to become NMN, then proceeds to NAD+.
The Preiss-Handler and de novo pathways
Nicotinic acid (niacin/NA) enters through the Preiss-Handler pathway and still has distinct tissue distribution. Niacin produces “flushing” through GPR109A activation — a side effect NMN and NR avoid because they do not activate this receptor. Tryptophan enters the de novo pathway and is the basis for why adequate dietary protein can partially compensate for niacin deficiency.
NMN vs. NR: a key note
Orally administered NMN appears to be partly converted to nicotinamide in the gut before absorption. NR is absorbed intact in humans and converted to NMN intracellularly by NRK1/2. In practice, head-to-head comparisons in humans show NMN and NR produce comparable increases in blood NAD+ at equimolar doses, suggesting similar effective delivery to the salvage pathway regardless of the mechanistic debate.
Human Clinical Trials
The evidence landscape
There are now more than 40 completed clinical trials of NAD+ precursors in humans. The consistent finding across essentially all studies: oral precursors reliably raise blood NAD+ levels. The inconsistent finding: whether that NAD+ increase produces measurable clinical benefits. The pattern that has emerged is that benefits are most apparent in populations with genuine metabolic impairment or identifiable deficits, rather than in healthy young adults with adequate baseline NAD+.
The landmark trial: Yoshino et al., Science 2021 (NMN, insulin sensitivity)
Design: 25 postmenopausal women with prediabetes who were overweight or obese, randomised to 250 mg/day NMN or placebo for 10 weeks. Primary outcome: skeletal muscle insulin sensitivity assessed by gold-standard hyperinsulinemic-euglycemic clamp. Skeletal muscle insulin sensitivity improved by approximately 25% compared to placebo. Downstream muscle insulin signalling (AKT and mTOR phosphorylation) was increased; gene expression related to muscle remodelling and PDGFR-β was upregulated.[4]
NMN and physical performance
A Japanese trial (250 mg/day NMN, 65–75 year olds, 12 weeks) found NMN significantly improved 4-metre walking time and sleep quality scores. A trial in healthy middle-aged adults (300 mg/day NMN, 12 weeks) found improved aerobic capacity (increased VO&sub2; max). These findings suggest possible physical performance benefits in older adults, though trials are small.
NR trials: mixed results
NR (1,000 mg/day) raises blood NAD+ by approximately 90% in older adults — confirming bioavailability. However, multiple RCTs found NR does not improve insulin sensitivity in men, does not improve whole-body or muscle insulin sensitivity in middle-aged and older men, and did not improve skeletal muscle mitochondrial function in young men over 7 days despite measurable NAD+ increases.[5]
A 2025 systematic review and meta-analysis of RCTs of NMN and NR for skeletal muscle mass and function in adults ≥60 years found that despite positive preclinical findings, the overall effect was negligible: neither NMN nor NR produced clinically meaningful improvements in skeletal muscle index, handgrip strength, or gait speed across studies.[8]
The tissue specificity problem
A recurring finding that deserves explicit acknowledgement: the reason for the absence of metabolic benefits of NR supplementation in several clinical studies of middle-aged and older-adult men is not known, but one explanation is that oral NAD+ precursors reliably raise NAD+ in blood cells without reliably raising NAD+ in skeletal muscle.[4] Whether they raise NAD+ in brain, liver, or other tissues is not consistently established in humans. A blood NAD+ measurement — the most commonly used endpoint in supplement marketing claims — does not prove that tissue NAD+ (where functional effects would occur) has been restored.
Evidence Summary
| Endpoint | Population | Precursor | Finding | Quality |
|---|---|---|---|---|
| Blood/PBMC NAD+ increase | Multiple populations | NMN and NR | ✅ Consistent, robust increases | Strong |
| Muscle NAD+ increase | Various | NMN and NR | ❌ Not consistently elevated in muscle | Negative/inconclusive |
| Muscle insulin sensitivity [4] | Prediabetic postmenopausal women | NMN 250 mg/d | ~25% improvement (euglycemic clamp) | Moderate (N=25; baseline imbalance concern) |
| Insulin sensitivity (men) | Middle-aged/older men | NR | ❌ No significant benefit in multiple RCTs | Negative |
| Fasting glucose/HbA1c (meta-analysis) [9] | General population | NMN (8 RCTs) | ❌ No significant benefit | Negative meta-analysis |
| Skeletal muscle mass/function [8] | Adults ≥60 years (meta-analysis) | NMN and NR | Negligible effect overall | Moderate; inconclusive |
| Physical performance (walking speed) | Healthy older adults 65–75 | NMN 250 mg/d | Improved walking speed and sleep | Moderate (single study) |
| Long COVID symptoms [6] | Long COVID patients | NR 2000 mg/d | Blood NAD+ restored; functional outcomes pending | Preliminary |
The Supplement Market vs. The Science
What is consistently true: Blood NAD+ levels decline substantially with age. Oral NMN and NR reliably raise blood NAD+ in humans. The mechanisms by which declining NAD+ impairs sirtuin and PARP function are well-characterised. Mouse studies showing metabolic and longevity benefits of NAD+ restoration are compelling. What is not yet established: Whether oral supplementation restores NAD+ in the tissues where functional decline matters most. Whether any NAD+ precursor produces clinically meaningful improvements in healthy adults without pre-existing metabolic impairment. What the optimal dose and duration would be for specific indications.
⚠️ In November 2022, the FDA issued a notification that NMN cannot be marketed as a dietary supplement in the US because it is the subject of prior drug research (a pharmaceutical company had filed IND applications studying NMN as a drug). This has been contested by the supplement industry; the legal and regulatory status of NMN remains contested as of April 2026. NR was granted GRAS (Generally Recognized as Safe) status as a food ingredient in 2016 and remains on the market without equivalent regulatory controversy.
Common Misconceptions
“Taking NAD+ supplements means you’re taking NAD+.”
NAD+ itself does not enter cells effectively when taken orally — it is too large and polar to cross cell membranes and is degraded in the gut. What people take are NAD+ precursors (NMN, NR) that are absorbed and then converted to NAD+ intracellularly. This is a meaningful distinction: the precursor’s pharmacokinetics, tissue distribution, and conversion efficiency determine what actually happens inside cells.
“Higher blood NAD+ means higher cellular NAD+.”
Multiple studies have found that blood NAD+ rises substantially after supplementation while muscle NAD+ does not increase measurably. Whether brain, liver, or other tissues are repleted is largely unknown in humans.
“Niacin/B3 is essentially the same thing as NMN.”
All forms of vitamin B3 (niacin, nicotinamide, NMN, NR) are precursors in the same NAD+ biosynthesis network but at different steps. Niacin produces vasodilatory flushing through GPR109A; NMN and NR do not. High-dose nicotinamide inhibits sirtuins and is hepatotoxic at excess doses. These compounds differ meaningfully in pharmacology and side effects despite sharing the same ultimate metabolic destination.
Frequently Asked Questions
Does exercise raise NAD+ levels?
Yes. Resistance training increases muscle NAD+ and NAMPT protein levels. HIIT and aerobic exercise raise blood NAD+ in humans and increase SIRT1 activity in muscle. This is one reason exercise produces so many metabolic benefits that resemble what NAD+ precursors are hypothesised to achieve: exercise is a natural inducer of NAD+ production.
Who might benefit most from NAD+ precursor supplementation?
The available human evidence suggests effects are more likely to be meaningful in individuals with genuine metabolic impairment (prediabetes, obesity, older age with declining function) rather than healthy young adults. A healthy 25-year-old with adequate mitochondrial function and normal NAMPT activity may see little functional benefit from supplementation even if blood NAD+ rises.
What about intravenous NAD+?
IV NAD+ infusions are offered by some longevity clinics, typically at doses of 250–1,000 mg over several hours. IV NAD+ does raise circulating NAD+. No rigorous controlled trials have evaluated IV NAD+ for any clinical indication. The infusions are associated with significant discomfort (nausea, flushing, chest pressure) during administration and can cost $200–$1,000 per infusion, substantially exceeding what oral supplementation costs with no proven additional benefit.
What is the relationship between NAD+ and sirtuins?
Sirtuins are NAD+-dependent deacylases — they cannot function without NAD+ as a co-substrate. SIRT1 (nucleus) regulates stress responses, circadian rhythm, and metabolism. SIRT3 (mitochondria) regulates mitochondrial protein acetylation and energy production. When NAD+ falls, sirtuin activity falls proportionally, impairing the regulatory programmes these enzymes execute.[1]
Key Takeaways
- NAD+ is foundational, not optional. It is the universal electron carrier and signalling cosubstrate on which energy metabolism, DNA repair, and gene regulation all depend. Its decline with age impairs regulatory systems that are central to aging biology.
- The age-related decline is real and mechanistically explained. CD38 upregulation driven by the inflammatory consequences of cellular senescence is the primary driver in mice; analogous increases in CD38 are observed in aging human tissues. The decline has identified enzymatic causes.[2]
- ✅ Oral NMN and NR reliably raise blood NAD+ in humans. This is one of the most consistently reproduced findings in the clinical trial literature. It is not sufficient evidence that tissues beyond blood cells are repleted, but it demonstrates the compounds are bioavailable and enter the NAD+ biosynthesis pathway.
- The most important human evidence remains the Yoshino 2021 Science paper — NMN improved muscle insulin sensitivity by ~25% in prediabetic postmenopausal women using the gold-standard euglycemic clamp. It is one trial in 25 women with a methodological concern about randomisation quality. It needs replication in a larger definitive trial.[4]
- ⚠️ Benefits in healthy adults are not established. Multiple NR trials in healthy or metabolically normal adults — particularly men — found no significant metabolic benefit despite confirmed blood NAD+ increases. Current evidence best supports potential benefit in older or metabolically compromised individuals.
- ⚠️ The NAD+ supplement market is substantially ahead of the clinical evidence. Commercially popular doses have not been compared to lower doses in powered clinical trials. Tissue NAD+ elevation at commercially recommended doses is not well-characterised. Long-term safety data for NMN is limited. The evidence base is growing quickly, but current marketing claims significantly exceed what the science supports.
References
Foundational Biochemistry and Aging
- Imai S, Guarente L. NAD+ and sirtuins in aging and disease. Trends in Cell Biology. 2014. PMC4112140
- Camacho-Pereira J, Tarragó MG, Chini CCS, et al. CD38 dictates age-related NAD decline and mitochondrial dysfunction through a SIRT3-dependent mechanism. Cell Metabolism. 2016;23(6):1127–1139. PMC4911708
- Sinclair DA, Guarente L. Why NAD+ declines during aging: It’s destroyed. Cell Metabolism. 2016. PMC5088772
Key Human Clinical Trials
- Yoshino M, Yoshino J, Kayser BD, Patti GJ, et al. Nicotinamide mononucleotide increases muscle insulin sensitivity in prediabetic women. Science. 2021;372(6547):1224–1229. doi: 10.1126/science.abe9985
- Elhassan YS, Kluckova K, Fletcher RS, et al. Nicotinamide riboside augments the aged human skeletal muscle NAD+ metabolome and induces transcriptomic and anti-inflammatory signatures. Cell Reports. 2019;28(7):1717–1728.
- Effects of nicotinamide riboside on NAD+ levels, cognition, and symptom recovery in long-COVID: a randomized controlled trial. PMC12675013. 2025.
- Orr ME, Kotkowski E, Ramirez P, et al. A randomized placebo-controlled trial of nicotinamide riboside in older adults with mild cognitive impairment. Geroscience. 2024;46(1):665–682.
Meta-analyses and Reviews
- Prokopidis K, Moriarty F, Bahat G, McLean J, Church DD, Patel HP. The effect of NMN and NR on skeletal muscle mass and function: A systematic review and meta-analysis. Journal of Cachexia, Sarcopenia and Muscle. 2025. PMC12022230
- Effects of NMN on glucose and lipid metabolism in adults: A systematic review and meta-analysis of RCTs. PMC11557618
- Fang EF, Lautrup S, Zhao Y, et al. NAD+ in aging and neurodegeneration. Trends in Molecular Medicine. Multiple reviews, Fang lab, University of Oslo, 2017–2025.
Key Investigators
- David A. Sinclair, PhD — Harvard Medical School; leading proponent of NAD+ biology in aging; co-inventor of multiple patents on NMN and NR applications; key figure in bringing NAD+ aging science to mainstream awareness.
- Shin-ichiro Imai, PhD — Washington University School of Medicine; pioneered the NAMPT/NAD+/SIRT1 axis in metabolic regulation; conducted the foundational mouse NMN studies and the Yoshino 2021 Science human trial.
- Eduardo Chini, MD, PhD — Mayo Clinic; led the CD38 identification as the primary driver of age-related NAD+ decline; continues to investigate CD38 inhibition as a therapeutic approach.
- Evandro Fei Fang, PhD — University of Oslo; leads human and rodent studies on NAD+ in brain aging and neurodegenerative disease; co-leads the NANOM clinical trial programme on NR in Alzheimer’s disease.
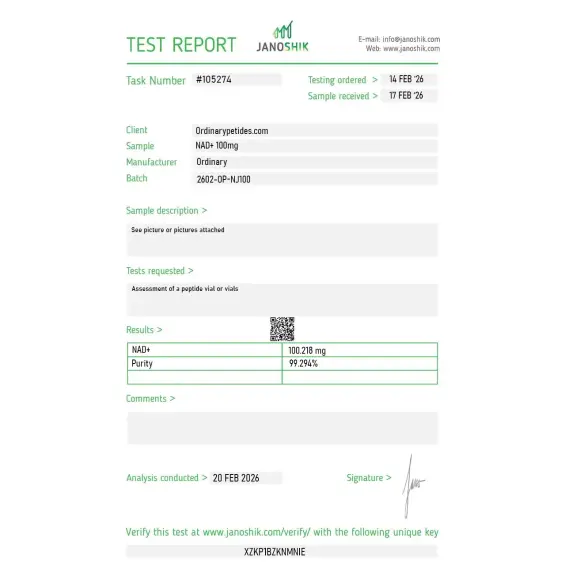
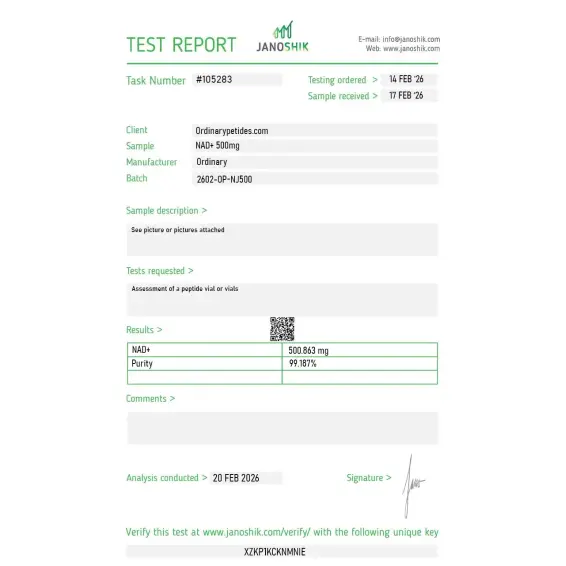
Certificate of Analysis
Independent test reports are available for NAD+ 100mg, 500mg, and 1000mg. These reports provide batch-level documentation and analytical verification information for research reference.
Based on 2 reviews
5.0
We use NAD+ in cell-free SIRT1 deacetylase activity assays where the precursor compounds wouldn't work — SIRT enzymes require NAD+ as cosubstrate directly, consuming it stoichiometrically per deacetylation event, and there's no in-vitro NAD+ biosynthesis to convert NMN or NR. For purified-enzyme sirtuin kinetics, direct NAD+ is the only option. The material gave clean Km determinations for our enzyme preparations across orders.
The compartment-specific NAD+ pool question is what we actually study — cells maintain distinct NAD+ pools in cytoplasm, mitochondria, nucleus, and Golgi, with separate biosynthesis enzymes (NMNAT1/2/3) localized to each compartment, and the pools turn over independently. For probing compartmentalized NAD+ biology in cell-imaging work, the direct cofactor is needed for in-vitro enzyme assays paired with the imaging — not the precursor compounds, which complicate the compartment readout. The material delivered consistent activity in our compartment-specific enzyme readouts.
No. But it is closely related to vitamin B3 metabolism, because many pathways of NAD+ synthesis use niacin, nicotinamide, NR, or NMN as precursors.
Scientifically, no. That is an incorrect classification. It belongs to coenzymes and dinucleotides.
There is no convincing basis for such a claim. Commercial prevalence and scientific proof are not the same thing.
The precursors, especially NR and NMN, are better studied in human trials. But even for them the clinical evidence base is still moderate, not revolutionary.
In a research context, yes. In routine practice, interpretation may be difficult, because the blood level does not always reflect the situation in specific tissues and does not always predict clinical effect.
Nicotinamide adenine dinucleotide (NAD+) is a naturally occurring coenzyme found in every living cell, synthesized from precursor molecules including tryptophan, nicotinamide riboside (NR), nicotinamide mononucleotide (NMN), and niacin (vitamin B3). It exists in two forms — the oxidized form NAD+ and the reduced form NADH — cycling continuously between them as it shuttles electrons in metabolic reactions. It is not technically a peptide in any sense — it is a dinucleotide composed of adenosine and nicotinamide joined by a phosphate group — but it appears frequently in the same longevity, anti-aging, and metabolic optimization contexts as the peptides in this series. NAD+ levels decline progressively and substantially with age — by approximately 50% between young adulthood and middle age — a decline associated with mitochondrial dysfunction, metabolic disease, cellular senescence, impaired DNA repair, and neurodegeneration. Restoring or maintaining NAD+ levels has become one of the most actively researched strategies in geroscience.
NAD+ functions as an essential cofactor in over 500 enzymatic reactions. Its most fundamental role is as an electron carrier in cellular respiration — accepting electrons during glycolysis and the Krebs cycle to form NADH, which then donates electrons to the electron transport chain to generate ATP. Beyond energy metabolism it serves as the obligatory substrate for three families of enzymes with direct longevity relevance. Sirtuins — the SIRT1 through SIRT7 family of NAD+-dependent deacylases — regulate gene expression, stress resistance, mitochondrial biogenesis, inflammation, and DNA repair. They are functionally silent without sufficient NAD+ as substrate. PARP enzymes (poly-ADP-ribose polymerases) consume NAD+ to repair DNA strand breaks — a critical genome maintenance function. CD38 is a major NAD+-consuming enzyme whose activity increases with aging and inflammation, contributing significantly to age-related NAD+ decline. The balance between NAD+ biosynthesis and these three consumption pathways determines cellular NAD+ availability and consequently the activity of all NAD+-dependent processes simultaneously.
Intravenous NAD+ infusion has been used clinically for decades in addiction medicine — particularly for alcohol and opioid withdrawal — where it appears to support neurological recovery, reduce withdrawal symptoms, and decrease craving, though the evidence base is primarily observational rather than from randomized controlled trials. High-dose niacin (nicotinic acid, a NAD+ precursor) is FDA-approved for dyslipidemia. More recently IV NAD+ infusion has been studied in neurodegenerative conditions, chronic fatigue, and post-COVID syndrome. Oral NAD+ precursors — particularly NR (nicotinamide riboside) and NMN (nicotinamide mononucleotide) — have completed multiple Phase 1 and Phase 2 human trials confirming they safely and effectively raise blood NAD+ levels, with a growing body of evidence for metabolic benefits in specific populations.
Human evidence is more developed than for most compounds in this series but still short of regulatory approval for aging-related indications. Multiple randomized controlled trials with NR and NMN have confirmed significant NAD+ elevation in blood and muscle tissue. Benefits documented in human trials include improved insulin sensitivity in obese or prediabetic adults, improved skeletal muscle mitochondrial function in older adults, reduced markers of inflammation, improved blood pressure in hypertensive patients, and improvements in cognitive function metrics in some populations. A landmark 2023 trial found NMN improved muscle insulin sensitivity and physical performance in postmenopausal women. The cardiovascular and neuroprotective benefits robustly demonstrated in animal studies have not yet been definitively replicated at scale in humans, though early signals are encouraging.
IV NAD+ infusion — typically 500 to 1000 mg infused over several hours — provides the most direct systemic delivery and is used in clinical settings for addiction treatment, neurological conditions, and wellness optimization. Oral NAD+ itself is poorly bioavailable as the molecule does not readily cross cell membranes intact, making precursors — NR, NMN, and niacin — the preferred oral route. NR and NMN are available as oral supplements, are absorbed intact, and are converted to NAD+ intracellularly. Typical human trial doses have been 250 to 1000 mg NR or NMN daily. Subcutaneous NAD+ injection is also practiced in some clinical settings as a middle ground between IV and oral administration.
The safety profile of NAD+ and its precursors is generally favorable. IV NAD+ infusions commonly cause nausea, flushing, chest tightness, and palpitations during the infusion — effects that resolve by slowing the infusion rate. These are well-characterized and manageable rather than dangerous. Oral NR and NMN have shown clean safety profiles in clinical trials with no serious adverse events at standard doses. Niacin — the oldest NAD+ precursor — causes the well-known prostaglandin-mediated flushing response and at therapeutic doses for dyslipidemia can cause hepatotoxicity, making extended-release niacin potentially hepatotoxic at high doses. Nicotinamide (a form of B3 that also raises NAD+) inhibits sirtuins at high concentrations — potentially counterproductive for the longevity applications — and can cause insulin resistance and liver enzyme elevation at high doses. The pharmacologically active forms NR and NMN avoid these concerns at standard supplementation doses.
This is the most nuanced safety question surrounding NAD+ therapeutics. NAD+ is required for DNA repair, and cancer cells — which proliferate rapidly and sustain high levels of DNA damage — have elevated NAD+ demand and often upregulate NAD+ biosynthetic enzymes. The theoretical concern is that elevating systemic NAD+ could fuel tumor growth. Published research presents conflicting signals — some studies suggest NAD+ elevation may actually impair certain cancer types through SIRT1-driven mechanisms, while others show elevated NAD+ supports tumor cell survival. The consensus in the field is that people with active cancer should discuss NAD+ supplementation with their oncologist rather than assuming it is safe or beneficial.
People with active cancer should consult their oncologist before using any NAD+ elevating therapy given the theoretical cancer support concern. People with liver disease should avoid high-dose niacin specifically given its hepatotoxicity risk. Those with a history of gout should use caution as niacin can elevate uric acid. Pregnant or breastfeeding women should consult their physician. People using blood thinners should note that niacin can potentiate anticoagulant effects.





