

SS-31
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
SS-31 (Elamipretide): A Peptide Aimed at Protecting Mitochondria From Oxidative Stress
SS-31, also known as Elamipretide, is a molecule actively researched as an antioxidant to protect mitochondria from oxidative stress. In research, SS-31 has demonstrated its ability to stabilize mitochondrial membranes, which helps minimize cell damage under stress conditions.
This peptide is being actively studied for its potential to improve cellular function, including that of neurons and heart cells, which could be useful for treating diseases related to mitochondrial dysfunction, such as neurodegenerative disorders and cardiovascular diseases.
In early studies using models of myocardial infarction and neurodegenerative diseases, SS-31 showed improvements in organ functions and a reduction in disease progression. However, clinical data is still limited, and further research is needed to confirm its broad effectiveness.
SS-31 (Elamipretide): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
SS-31 is one of the most conceptually important compounds in this entire series. Not because its clinical evidence is the most extensive — it isn’t — but because it represents the first successful pharmacological proof of a concept that has driven mitochondrial biology research for decades: that selectively targeting the inner mitochondrial membrane can restore bioenergetic function in disease.
On September 19, 2025, the FDA granted accelerated approval to elamipretide for Barth syndrome — an ultra-rare X-linked mitochondrial cardiomyopathy affecting approximately 150 Americans, with 85% of early deaths occurring before age 5 and no previously approved treatment. This made elamipretide the first-ever FDA-approved mitochondria-targeted therapeutic — a milestone anticipated in mitochondrial medicine for nearly two decades.[2]
The broader programme has been more difficult. Heart failure trials (STRIVE-HF, PROGRESS-HF) failed their primary endpoints. The MMPOWER-3 Phase 3 trial in primary mitochondrial myopathy also failed its primary endpoints. The pattern — dramatic efficacy where cardiolipin is the specific and primary pathological target, failure in broader conditions where mitochondrial dysfunction is one factor among many — teaches an important lesson about mechanism-based drug development.
| At a glance | |
|---|---|
| INN / Generic name | Elamipretide |
| Research name | SS-31; also: MTP-131, Bendavia |
| Name meaning | SS = Szeto-Schiller; 31 = compound designation in the series |
| Structure | D-Arg-dimethylTyr-Lys-Phe-NH&sub2; (tetrapeptide; 4 amino acids) |
| Molecular weight | ~640 Da |
| Discoverers | Dr. Hazel H. Szeto (Weill Cornell / Cornell University) and Dr. Peter W. Schiller (IRCM, Montreal) |
| Mechanism | Selectively targets inner mitochondrial membrane; binds cardiolipin → stabilises cristae structure → reduces ROS → maintains ATP production |
| FDA approval | ✅ Accelerated approval September 19, 2025 (Barth syndrome) |
| Administration | Subcutaneous injection (~92% bioavailability) |
| Ongoing Phase 3 trials | Primary mitochondrial myopathy; dry AMD |
The Discovery: Serendipity and Confocal Microscopy
The SS peptide series originated at the IRCM (Institut de recherches cliniques de Montréal) in Peter Schiller’s laboratory around 2000. Schiller had been designing novel opioid peptide analogues with an alternating aromatic-cationic structure. A key breakthrough occurred when he created a fluorescent version for a confocal laser scanning microscopy study, allowing researchers to observe for the first time that it entered cells and concentrated specifically in mitochondria. This was not predicted by any existing pharmacological model — Schiller and Szeto had not designed these peptides to be mitochondria-targeted. This led to the creation of a new class of molecules — Szeto-Schiller (SS) peptides — which localise to the inner mitochondrial membrane, the site of energy production in cells.[6]
Structure: The Alternating Aromatic-Cationic Architecture
SS-31’s sequence: D-Arg–dimethylTyr–Lys–Phe–NH&sub2;. D-Arg (D-arginine): D-amino acids are not recognised by most proteases, conferring metabolic stability; arginine’s guanidinium group carries strong positive charge for electrostatic attraction to cardiolipin head groups. dimethylTyr (2’,6’-dimethyltyrosine; Dmt): Two methyl groups on the aromatic ring prevent oxidative modification and contribute to charge shielding. Lys: Second positively charged residue, together with D-Arg driving electrostatic attraction to cardiolipin. Phe: Aromatic hydrophobic residue contributing to membrane penetration. C-terminal amide: Protects the C-terminus from carboxypeptidase cleavage.
Despite the presence of positively charged arginine and lysine residues, elamipretide retains high cell permeability, which is suggested to be due to positive charge shielding by electrons in π orbitals in aromatic rings of phenylalanine and dimethyltyrosine. The aromatic rings’ electron clouds reduce the net positive charge at the cell surface while preserving the compound’s ability to accumulate at the highly negatively charged inner mitochondrial membrane — where the electrochemical gradient is substantially more negative than the plasma membrane.[5]
Target: Cardiolipin and the Inner Mitochondrial Membrane
What is cardiolipin?
Cardiolipin (CL) is an unusual phospholipid with two phosphate head groups and four fatty acid chains, found almost exclusively in the inner mitochondrial membrane (IMM). It comprises approximately 20% of IMM lipid content and is essential for cristae structural integrity; assembly and supramolecular organisation of respiratory complexes I, III, IV (the “respirasomes”); ATP synthase efficiency; and maintenance of the ~−180 mV electrochemical gradient driving ATP production. Cardiolipin externalisation (flip to the outer membrane) acts as an “eat me” signal for damaged mitochondria; its peroxidation triggers cytochrome c release and apoptosis.
How SS-31 engages cardiolipin
Elamipretide localises to the inner mitochondrial membrane and binds to cardiolipin via electrostatic interactions due to its positively charged amino acid residues. This binding stabilises cardiolipin, preventing oxidative damage and maintaining mitochondrial membrane potential. Elamipretide reduces cardiolipin peroxidation, preserving mitochondrial structure and function through the maintenance of cristae integrity, reduction in ROS production, and preservation of mitochondrial ATP production.[7]
The PNAS cross-linking/mass spectrometry study (Chavez et al., 2020) identified SS-31’s protein interaction partners in mitochondria: the SS-31-interacting proteins, all known cardiolipin binders, fall into two groups — those involved in ATP production through the oxidative phosphorylation pathway and those involved in 2-oxoglutarate metabolic processes — directly confirming that SS-31 concentrates at cardiolipin-binding sites associated with the OXPHOS machinery.[4]
Barth Syndrome: The Proof-of-Concept Disease
Barth syndrome (BTHS) is an X-linked recessive mitochondrial disease caused by mutations in the TAFAZZIN (TAZ) gene, encoding an acyltransferase required for cardiolipin remodelling. TAZ mutations → defective cardiolipin remodelling → elevated MLCL/CL ratio → structurally compromised IMM → mitochondrial bioenergetics failure → cardiomyopathy + skeletal myopathy. Clinical features: left ventricular non-compaction cardiomyopathy, dilated cardiomyopathy, skeletal muscle weakness, intermittent neutropenia, growth retardation, 3-methylglutaconic aciduria. Prognosis: 85% of early deaths occur before age 5. US prevalence: approximately 150 patients.
Barth syndrome’s pathophysiology is directly and specifically a cardiolipin problem. SS-31’s mechanism — cardiolipin stabilisation — addresses the primary molecular defect with unusually high mechanistic precision.
The TAZPOWER trial
Part 1 (Phase 2/3, 28 weeks, double-blind, placebo-controlled): 12 patients randomised 2:1 to elamipretide vs. placebo. Published by Thompson et al. in Genetics in Medicine (2021).[1] Long-term extension (to 168 weeks/~3.5 years): Eight patients improved their ability to walk in six-minute increments, with an average improvement of 96.1 metres per person over their baseline. An improvement was seen in cardiac stroke volume. Participants had improved cardiolipin levels (normalised MLCL/CL ratio) compared to when they began the study — directly confirming the drug is reaching its target and producing the intended molecular effect.
The 10-6 advisory committee vote reflects genuine scientific tension: a very small patient population (N cannot be large given ~150 US patients), open-label extension design, no randomised controlled comparison at the longest follow-up. The vote was a real judgment call that the evidence was sufficient for accelerated approval in a disease with no alternative and extreme severity.
The Programme That Didn’t Work: Heart Failure
STRIVE-HF (Daubert et al., Circulation: Heart Failure, 2017): N=71, HFrEF patients. Phase 2. Primary endpoint: change in 6-minute walk distance. Failed.[8] PROGRESS-HF (Butler et al., Journal of Cardiac Failure, 2020): Phase 2 continuation. Also failed its primary endpoint.[9]
These failures are important to understand, not dismiss. In heart failure, mitochondrial dysfunction is real but is one component of a multi-system disease involving fibrosis, neurohormonal dysregulation, inflammation, wall stress, and haemodynamic changes. Correcting mitochondrial function alone in established HFrEF — where structural remodelling may be irreversible — may not produce functional improvement on exercise capacity endpoints over short trial durations. The lesson is about disease context, not mechanism validity.
Primary Mitochondrial Myopathy: A Mixed Picture
MMPOWER-3 (Phase 3): N=218 patients with genetically confirmed PMM. Randomised to elamipretide 40 mg/day SC vs. placebo for 24 weeks. Primary endpoints: 6-minute walk test improvement + PMMSA total fatigue score. While this study did not meet its primary endpoints, participants treated with elamipretide did report slightly less total fatigue as assessed by the PMMSA total fatigue score. Phase 3 PMM trial ongoing.[10]
Age-Related Macular Degeneration: Ongoing Phase 3
ReCLAIM (Phase 2, dry AMD): Did not meet primary endpoints (change in low luminance visual acuity or geographic atrophy area). However, elamipretide was associated with a significantly greater reduction in the progression of partial EZ attenuation (15% elamipretide vs. 34% placebo; P=0.01) and in total EZ attenuation (26% elamipretide vs. 48% placebo; P=0.04). In addition, more patients experienced a ≥2-line gain in LL-BCVA (14.6% elamipretide vs. 2.1% placebo; P=0.04). The ellipsoid zone finding — slowing of photoreceptor layer degradation — is biologically meaningful as a predictor of AMD progression. Phase 3 dry AMD trial ongoing.[11]
Complete Clinical Trial Summary
| Trial | Indication | Phase | N | Outcome |
|---|---|---|---|---|
| TAZPOWER Part 1 [1] | Barth syndrome | 2/3 | 12 | ✅ Positive; supported approval |
| TAZPOWER extension | Barth syndrome | OLE | 8–10 | ✅ +96.1m walk; cardiac improvement; MLCL/CL normalisation |
| STRIVE-HF [8] | HFrEF | 2 | 71 | ❌ Failed primary endpoint |
| PROGRESS-HF [9] | HFrEF | 2 | ~71 | ❌ Failed primary endpoint |
| MMPOWER-3 [10] | PMM | 3 | 218 | ❌ Failed primary endpoints; fatigue signal |
| ReCLAIM [11] | Dry AMD | 2 | ~60 | Failed primary; positive EZ signal (P=0.01/0.04) |
| Phase 3 PMM | PMM | 3 | Ongoing | Pending |
| Phase 3 AMD | Dry AMD | 3 | Ongoing | Pending |
Safety Profile
SS-31/elamipretide has a consistently documented and favourable safety profile across all clinical programmes. The most common adverse event is mild injection site reactions — redness, swelling, itching, or brief discomfort at the SC injection site — which generally resolve with continued use. No clinically significant cardiac, hepatic, renal, or haematological adverse events attributable to elamipretide have been documented across Phase 2/3 trial populations. No serious drug-related adverse events were documented in TAZPOWER, STRIVE-HF, PROGRESS-HF, MMPOWER-3, or ReCLAIM.
Elamipretide is metabolised by peptidases to natural amino acid components — no toxic metabolites, no cytochrome P450 interactions anticipated. Subcutaneous bioavailability is approximately 92% — very high for a peptide. The TAZPOWER open-label extension provided up to 168 weeks (~3.5 years) of safety data in Barth syndrome patients without emerging safety signals.
Common Misconceptions
“SS-31 approved means it works for anti-aging.”
The FDA approval is specifically for Barth syndrome — a disease where cardiolipin is the primary molecular defect. The approval does not extend to anti-aging, general mitochondrial optimisation, or any other indication. Accelerated approval for a rare disease is not approval for anti-aging use.
“SS-31 failed in heart failure so the mechanism doesn’t work.”
Heart failure is a multi-system disease with irreversible structural remodelling. Correcting mitochondrial function in established HFrEF may not produce functional improvement on 6-minute walk endpoints at Phase 2 trial durations, even if the mitochondrial mechanism is valid. The Barth syndrome data confirms the mechanism works specifically when cardiolipin pathology is the primary driver.
“SS-31 is a naturally occurring peptide.”
SS-31 is entirely synthetic. Unlike MOTS-c, which is encoded in the mitochondrial genome, SS-31 was designed from scratch by Hazel Szeto and Peter Schiller. Its four-amino-acid sequence was deliberately engineered to interact with cardiolipin on the inner mitochondrial membrane. It does not occur in nature.
Frequently Asked Questions
How does elamipretide compare to MitoQ?
MitoQ is a mitoquinone (CoQ10) derivative conjugated to the triphenylphosphonium (TPP+) cation, acting as a mitochondrial antioxidant by scavenging ROS downstream. SS-31 acts by stabilising cardiolipin structurally and reducing the source of ROS production (dysfunctional OXPHOS) rather than scavenging ROS downstream. The mechanisms are complementary but distinct; only elamipretide has FDA approval.
Why is the FDA approval “accelerated”?
Accelerated approval uses a surrogate or intermediate clinical endpoint — here, cardiolipin level normalisation (MLCL/CL ratio) and sustained functional improvement in open-label extension — rather than a primary pre-specified RCT endpoint to support approval. This pathway is appropriate for rare diseases with unmet need and allows earlier patient access; confirmatory post-marketing studies are required.[2]
What is the connection between SS-31 and the broader SS peptide series?
Szeto and Schiller synthesised a series of aromatic-cationic peptides (SS-02, SS-20, SS-31, etc.) with different amino acid combinations, all found to localise to the IMM. SS-31 was selected for clinical development because it showed the most favourable combination of potency, selectivity, and tolerability. Second-generation compounds (e.g., bevemipretide/SBT-272 as a topical ophthalmic formulation for AMD) are also in development by Stealth BioTherapeutics.
Key Takeaways
- ✅ Elamipretide is the first approved mitochondria-targeted therapeutic in history (FDA accelerated approval, September 19, 2025, Barth syndrome). This is a milestone for the entire field of mitochondrial medicine, not just for the specific disease.[2]
- The discovery was genuinely serendipitous — Schiller saw his fluorescent peptide concentrate in mitochondria under confocal microscopy without ever intending to design a mitochondria-targeting compound. Some of the most important pharmacological discoveries arise this way.[6]
- ✅ The mechanism is specific and well-characterised at the molecular level. Cardiolipin binding via electrostatic and amphipathic interactions; stabilisation of OXPHOS complex assembly; reduction of ROS production at its source; maintenance of cristae architecture. This is among the best-characterised mechanisms of any compound in this series.[4][5]
- The clinical trial record is instructive about the limits of mechanism-targeted therapy. SS-31 works dramatically when cardiolipin pathology is the primary driver (Barth syndrome). It failed to demonstrate benefit on primary endpoints when mitochondrial dysfunction is one component of a complex multi-system disease (HFrEF, PMM). This is not a failure of the mechanism — it is information about where the mechanism is sufficient to produce clinical benefit.
- ⚠️ Community off-label use has essentially no clinical trial support. The preclinical rationale for anti-aging and longevity uses exists. The human data supporting these applications does not.
References
FDA Approval and Barth Syndrome Pivotal Data
- Thompson WR, et al. A phase 2/3 randomised clinical trial followed by an open-label extension to evaluate the effectiveness of elamipretide in Barth syndrome, a genetic disorder of mitochondrial cardiolipin metabolism. Genetics in Medicine. 2021;23:471–478.
- FDA accelerated approval of elamipretide for Barth syndrome. September 19, 2025.
- FDA Cardiovascular and Renal Drugs Advisory Committee vote (10–6 in favour). October 11, 2024.
Mechanism Papers
- Chavez JD, et al. Mitochondrial protein interaction landscape of SS-31. PNAS. 2020;117(26). PMC7334473
- Szeto HH. First-in-class cardiolipin-protective compound as a therapeutic agent to restore mitochondrial bioenergetics. British Journal of Pharmacology. 2014;171:2029–2050.
- Szeto HH, Birk AV. Serendipity and the discovery of novel compounds that restore mitochondrial plasticity. Clinical Pharmacology and Therapeutics. 2014;96:672–683.
- Birk AV, et al. The mitochondrial-targeted compound SS-31 re-energizes ischaemic mitochondria by interacting with cardiolipin. Journal of the American Society of Nephrology. 2013;24:1250–1261.
Clinical Trials
- Daubert MA, et al. Novel mitochondria-targeting peptide in heart failure treatment. Circulation: Heart Failure. 2017;10. (STRIVE-HF)
- Butler J, et al. Effects of elamipretide on left ventricular function in patients with heart failure with reduced ejection fraction: the PROGRESS-HF Phase 2 trial. Journal of Cardiac Failure. 2020;26:429–437.
- Efficacy and Safety of Elamipretide in Individuals with Primary Mitochondrial Myopathy: The MMPOWER-3 Randomised Clinical Trial. PMC10382259
- ReCLAIM Phase 2: Phase 1 Clinical Trial of Elamipretide in Dry Age-Related Macular Degeneration. PMC9560640
- Campbell MD, et al. Improved mitochondrial energetics with SS-31 in aging muscle. Journal of Gerontology A: Biological Sciences and Medical Sciences. 2019.
Review
- Elamipretide: a review of its structure, mechanism of action, and therapeutic potential. International Journal of Molecular Sciences. 2025;26(3):944. PMC11816484
Key Investigators
- Hazel H. Szeto, MD, PhD — Weill Cornell Medical College (Cornell University); co-discoverer of the SS peptide series; developed the mechanistic understanding of cardiolipin-targeted mitochondria therapy.
- Peter W. Schiller, PhD — IRCM, Montreal; co-discoverer; the serendipitous confocal microscopy observation that launched the programme.
- Reid Thompson, MD — Johns Hopkins Medicine; principal investigator of the TAZPOWER Barth syndrome clinical trial.
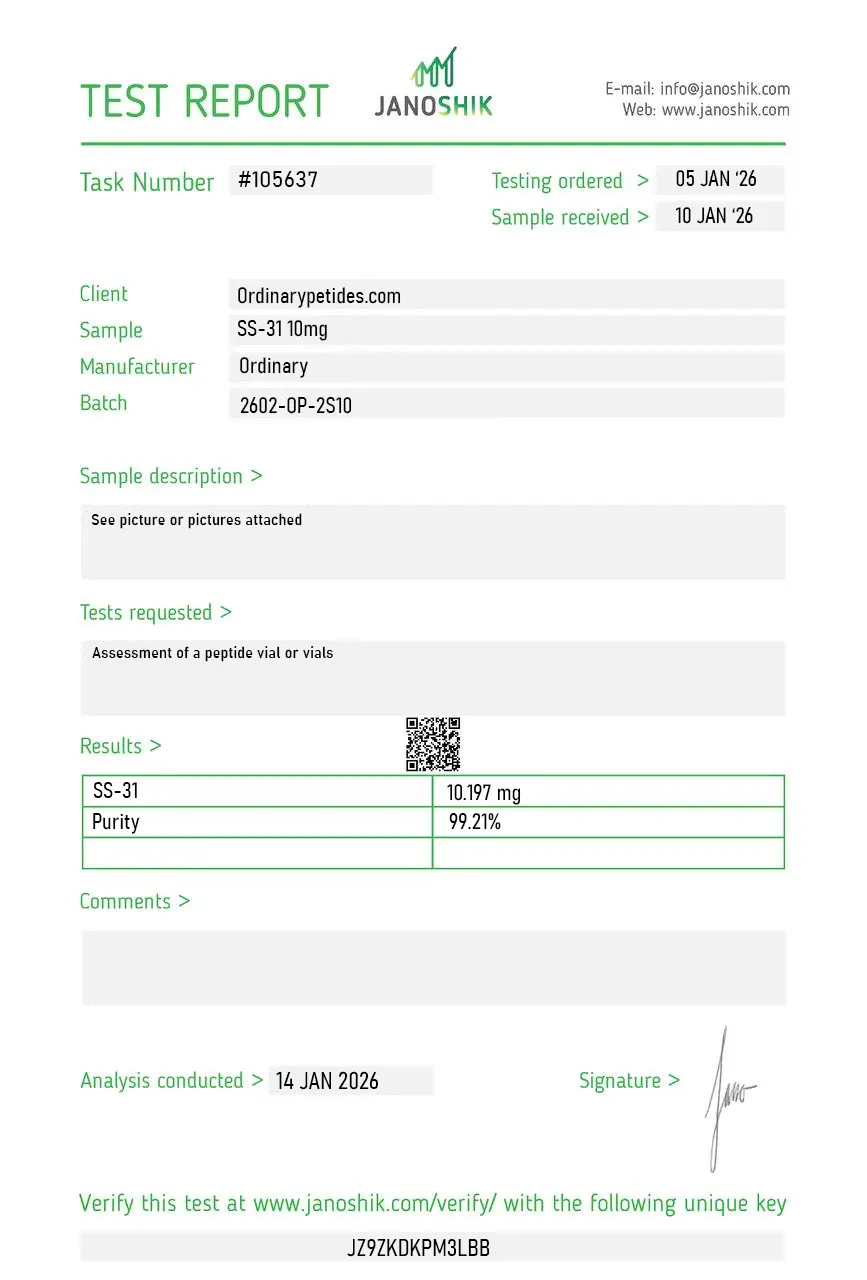
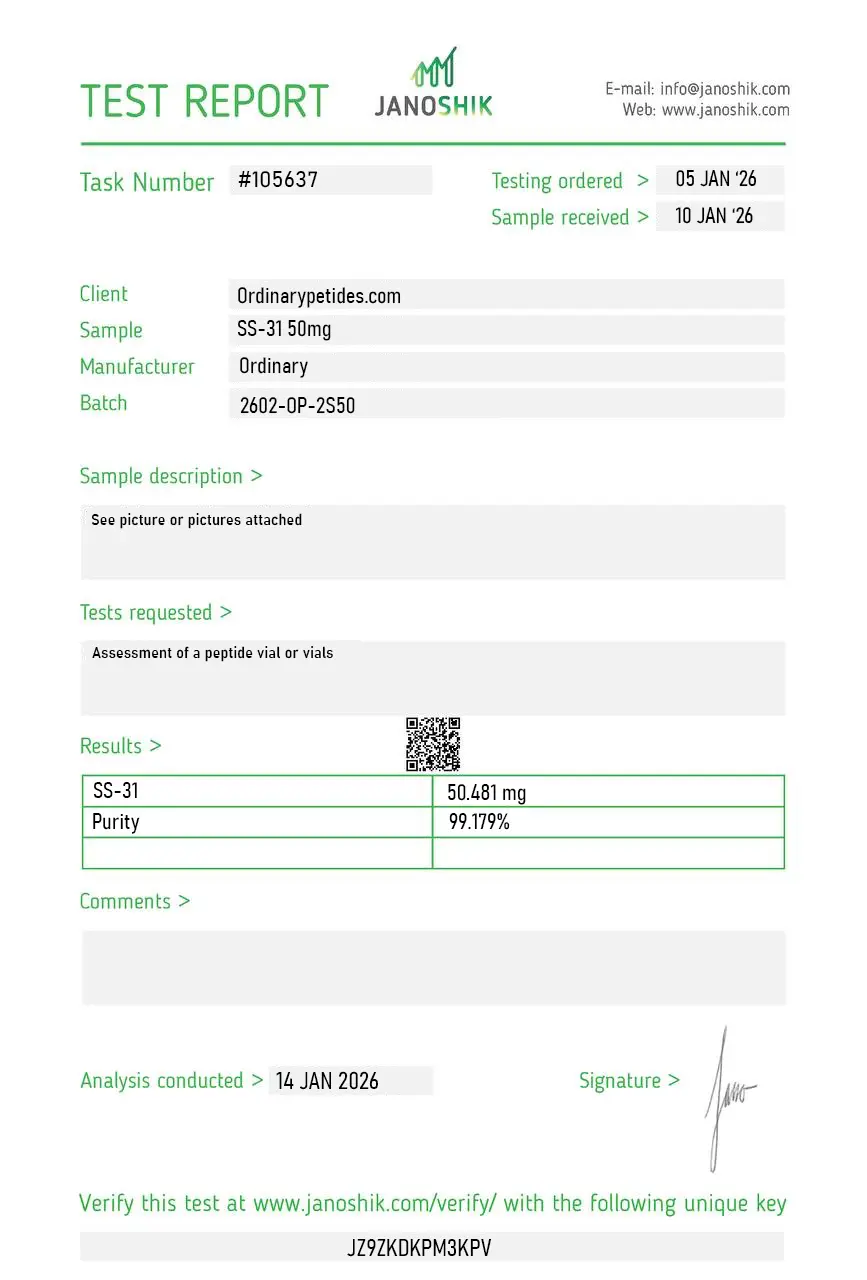
Certificate of Analysis
Independent test reports are available for SS-31 10mg and SS-31 50mg. These reports provide batch-level documentation and analytical verification information for research reference.
Based on 1 reviews
5.0
The cardiolipin-binding mechanism is what differentiates SS-31 from generic antioxidants — it concentrates specifically at the inner mitochondrial membrane through electrostatic interaction with cardiolipin's negatively-charged phosphate groups, which is why it's selectively mitochondrial rather than diffusing through the cytoplasm. For probing inner-membrane biology specifically, the targeting peptide is the right tool because most antioxidants don't have that subcellular selectivity. The material delivered the expected mitochondrial accumulation in our imaging assays.
SS-31 stabilizes mitochondrial membranes and protects cells from oxidative stress, helping to prevent their damage.
The peptide is being researched for the treatment of neurodegenerative diseases, cardiovascular disorders, and age-related diseases, but clinical data is limited.
Currently, the side effects of SS-31 are minimal, but long-term effects have not been fully studied.
SS-31 (also known as elamipretide, MTP-131, and Bendavia) is a synthetic aromatic-cationic tetrapeptide with the sequence D-Arg-Dmt-Lys-Phe-NH₂, where Dmt represents 2',6'-dimethyltyrosine — a modified tyrosine with enhanced antioxidant properties. It was discovered serendipitously by Hazel Szeto and Peter Schiller at Cornell University while studying opioid receptors, and represents the lead compound of the Szeto-Schiller (SS) peptide class of mitochondria-targeting therapeutics. It is the first-in-class compound specifically designed to target cardiolipin — a unique phospholipid found almost exclusively in the inner mitochondrial membrane — and has been developed clinically by Stealth BioTherapeutics. It has received FDA Orphan Drug designation for Barth syndrome and primary mitochondrial myopathy, and Fast Track designation for primary mitochondrial myopathy and Leber's Hereditary Optic Neuropathy. It has not received FDA approval for any therapeutic indication.
SS-31's mechanism is fundamentally different from every other compound in this series. While most peptides act on cell surface receptors or intracellular signaling pathways, SS-31 acts inside mitochondria — and does so with remarkable selectivity. Its two positively charged amino acids (D-Arg and Lys) are electrostatically attracted to the highly negatively charged cardiolipin in the inner mitochondrial membrane, causing SS-31 to accumulate at concentrations approximately 5,000-fold higher inside mitochondria than in the surrounding cytoplasm. Once at the inner mitochondrial membrane it serves multiple functions simultaneously. It stabilizes cardiolipin's physical structure, which in turn maintains the folded cristae architecture of the inner membrane where the electron transport chain complexes are organized — cristae collapse is a key early event in mitochondrial dysfunction. It inhibits the aberrant peroxidase activity of cytochrome c — the electron carrier that, when oxidized lipids of the inner membrane convert it from an electron carrier into a peroxidase enzyme, generates reactive oxygen species rather than transferring electrons for ATP production. By restoring cytochrome c to its electron-carrying function SS-31 simultaneously reduces ROS generation and improves ATP output through the same molecular interaction. Its modified tyrosine (Dmt) scavenges reactive oxygen species directly, converting damaging oxygen radicals into stable di-tyrosine. Cross-linking mass spectrometry studies published in PNAS documented that SS-31's protein interactors in mitochondria fall into two groups — components of the oxidative phosphorylation pathway and 2-oxoglutarate metabolic processes — all known cardiolipin binders, mechanistically connecting its cardiolipin binding to improved ATP production.
The preclinical evidence across multiple disease models is genuinely impressive and spans an unusual breadth of conditions. In cardiac models SS-31 reduces ischemia-reperfusion injury, improves left ventricular function in heart failure, and normalizes mitochondrial dynamics in failing cardiac tissue. In skeletal muscle aging studies in mice prolonged SS-31 treatment reversed age-related redox stress, restored glutathione homeostasis, increased muscle mass, and significantly improved treadmill endurance — without increasing mitochondrial content, demonstrating that quality improvement rather than quantity expansion is the mechanism. In kidney models it protects against ischemia-reperfusion injury and atherosclerotic renovascular disease. In neurological models it restored synaptic viability, mitochondrial motility, and mitochondrial transport in Alzheimer's disease mouse neurons, reduced oxidative stress after subarachnoid hemorrhage, and showed benefit in Parkinson's disease models. In metabolic models it demonstrated benefit in atherosclerosis, diabetes, glaucoma, and osteoarthritis models. In Barth syndrome — a genetic disorder of cardiolipin metabolism — it ameliorated cardiac mitochondrial morphology and defective mitophagy in mouse models consistent with its cardiolipin-binding mechanism.
This is where SS-31's story becomes more nuanced than its preclinical profile suggests. Multiple completed and ongoing clinical trials have produced mixed results. In Barth syndrome the TAZPOWER Phase 2/3 randomized crossover trial showed significant improvement in the 6-Minute Walk Test and Barth Syndrome Symptom Assessment Scale over 48 weeks of open-label extension — a positive signal in this rare genetic cardiolipin disorder where the mechanism is most directly relevant. In heart failure with reduced ejection fraction the PROGRESS-HF Phase 2 trial showed favorable changes in left ventricular volumes but the larger MMPOWER-3 Phase 3 trial in primary mitochondrial myopathy failed to meet its primary endpoint. In atherosclerotic renal artery stenosis a Phase 2a trial showed good tolerability and some renal functional improvement. Overall the clinical picture reflects a compound with compelling mechanism and preclinical data that has not yet translated into consistent definitive efficacy in large randomized trials — a pattern seen with many mitochondria-targeted compounds and possibly reflecting the complexity of delivering benefit in heterogeneous patient populations with established disease.
In clinical trials SS-31 is administered by subcutaneous injection — typically 40 mg daily as a single subcutaneous dose. Intravenous infusion has been used in some cardiac and renal trials. It is not orally bioavailable. Outside of clinical trials SS-31 is available as a research peptide through vendors, but no standardized human therapeutic protocol exists given the absence of FDA approval.
SS-31 has a favorable safety profile consistent across multiple clinical trials — no serious adverse reactions or fatalities have been reported in published trial data. The dominant adverse effects are injection site reactions — erythema in approximately 57% of participants, pruritus in 47%, pain in 20%, urticaria in 20%, and irritation in 10% — almost all mild. Dizziness and headache are occasionally reported. Transient fatigue and mild gastrointestinal symptoms have been noted. Because it does not interact with hormonal pathways, surface receptors, or immune regulatory systems in the manner of most compounds in this series, its systemic safety profile is clean. Its mitochondrial-specificity — it has no effects on normal mitochondria and does not enter the mitochondrial matrix — is cited as a key safety feature.
People with known hypersensitivity to any component of the formulation should not use it. Pregnant or breastfeeding women should not use it given absent safety data. People considering it outside of approved clinical trials should understand the compound remains investigational and the clinical efficacy data in the most relevant disease targets has been disappointing in Phase 3 settings. Wellness and longevity applications based on preclinical aging data represent speculative extrapolation from mouse studies that have not been validated in human trials. The most appropriate pathway to access SS-31 for anyone with a relevant mitochondrial disease is through enrollment in an ongoing clinical trial or the expanded access program operated by Stealth BioTherapeutics.





