
Humanin
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Humanin: A Mitochondrial Micropeptide With Real Scientific Depth
Humanin is not just another "trendy peptide," but the body's own mitochondrial-derived micropeptide that attracted scientific attention as a signal of cellular protection. In the research context, it has been studied in places where cells are especially vulnerable to stress: in neurons, the heart, metabolic models, reproductive tissues, and the biology of aging.
In preclinical data, Humanin and its more potent analogs showed anti-apoptotic, cytoprotective, and anti-inflammatory effects, which is why interest in it moved far beyond neurobiology alone. That is exactly what makes it genuinely intriguing: it does not look like a "peptide riding hype," but rather like part of a large and very much alive science of mitochondria, cellular resilience, and age-related biology.
In other words, Humanin is interesting not because it shouts the loudest, but because the biology behind it has something real to say. At the same time, the line matters: Humanin is not yet a proven "longevity peptide" and not a ready-made clinical therapy for rejuvenation, the brain, the heart, or metabolism in humans.
Practical Takeaway
If what interests you is not loud promises but a strong scientific story with real biological depth, Humanin is definitely worth attention.
Humanin: A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Humanin is different from every other compound in this article series. It is not a synthetic pharmaceutical designed to exploit a known receptor. It is not a fragment of an exogenous hormone. Humanin is a peptide encoded directly in the mitochondrial genome of every cell in the human body — discovered not by medicinal chemists, but by a Japanese neuroscientist looking for something to protect neurons from Alzheimer’s disease.
This origin story is remarkable: scientists found that the mitochondrial genome — long considered a purely metabolic instruction set — encodes a small peptide that gets secreted from cells and acts as a survival signal. Humanin was the first identified member of what is now an entire family of mitochondrial-derived peptides (MDPs), which includes the small humanin-like peptides (SHLPs 1–6) and MOTS-c.[1]
Understanding humanin requires holding two frames simultaneously. What is established: humanin is an endogenous 24-amino acid peptide encoded within the mitochondrial genome. It circulates in human plasma. Its levels decline with age. It is lower in Alzheimer’s disease, MELAS, and coronary artery disease. Children of centenarians have substantially higher humanin levels than age-matched controls. In cell culture and animal models, humanin and its analogues protect against a broad range of cellular stressors through multiple molecular mechanisms. What is not established: whether exogenous humanin administration in humans replicates these protective effects, whether it is safe, what dose does what, and whether the association between circulating humanin levels and longevity reflects causation or correlation. No human intervention trials have been completed.[3]
| At a glance | |
|---|---|
| Origin | Endogenous peptide; encoded in human mitochondrial genome |
| Gene | MT-RNR2 (16S rRNA gene of mitochondrial DNA) |
| Discovery | 2001 — Nishimoto lab, Keio University; independently confirmed by Reed lab and Cohen lab |
| Length | 24 amino acids (cytoplasmic translation); 21 AA (mitochondrial translation) |
| Full sequence (24 AA) | MAPRGFSCLLLLTSEIDLPVKRRA |
| Molecular weight | ~2,700 Da |
| Classification | Mitochondrial-derived peptide (MDP); founding member of the MDP family |
| Key analogue | HNG (S14G-humanin) — approximately 1,000× more potent than native humanin |
| Primary receptors | CNTFR/WSX-1/gp130 trimeric complex (→ JAK2/STAT3); FPRL1/FPR2 (→ ERK1/2) |
| Intracellular targets | BAX, IGFBP-3, Bid (anti-apoptotic) |
| FDA status | ❌ Not approved; no approved indication; no IND filed |
| Human trials | ❌ None completed |
| WADA | Not specifically listed |
The Discovery: Mitochondria as a Communication System
In the late 1990s, Ikuo Nishimoto and colleagues at Keio University screened the entire expressed genetic library from the surviving neurons of an Alzheimer’s patient brain, looking for whatever was keeping those cells alive. Further functional and positional screening of the clones carrying various fragments of the 16S rRNA revealed a 75 bp open reading frame that yields a 24-amino acid peptide, designated humanin.[1]
The mitochondrial genome is only 16,569 base pairs — an ancient bacterial relic — and was believed to encode only 13 proteins, all components of the oxidative phosphorylation machinery. Finding a small open reading frame within the 16S rRNA itself, encoding a functional secreted peptide, was entirely unexpected. The term humanin was coined by its discoverer, Professor Nishimoto, prior to his premature passing from cancer, to denote the potential of this molecule to restore the “humanity” of patients with Alzheimer’s disease.[2]
The simultaneous and independent discovery of humanin by the Reed lab (screening for Bax-binding proteins) and the Pinchas Cohen lab at USC (screening for IGFBP-3-binding proteins) immediately confirmed this was a genuine multi-functional endogenous molecule.
The MDP family: humanin was just the beginning
Humanin opened a research programme that revealed several additional mitochondrial-encoded peptides. Six small humanin-like peptides (SHLPs 1–6) are encoded from the 16S rRNA region. SHLP2 protects cells from amyloid β-induced toxicity and age-related macular degeneration. SHLP2 and SHLP3 promote mitochondrial biogenesis and reduce reactive oxygen species. Unlike these cytoprotective SHLPs, SHLP6 induces apoptosis in multiple cell lines. MOTS-c, encoded from the 12S rRNA, has a complementary primarily metabolic profile — exercise mimicry and insulin sensitisation rather than cytoprotection. Together, these MDPs suggest that mitochondria function as a system-wide stress monitoring and response network.[4]
Molecular Biology
Sequence and isoforms
The full 24-amino acid sequence is: MAPRGFSCLLLLTSEIDLPVKRRA. The mitochondrial translation code differs from the cytoplasmic code at one position, producing a 21-amino acid form (MAPRGFSCLLLLTSEIDLPV) — four C-terminal residues shorter. Both isoforms are biologically active.
A natural variant (SNP rs2854128) in the humanin coding region is associated with lower circulating humanin levels and accelerated cognitive ageing in African Americans — providing genetic evidence that endogenous humanin levels influence neurological health outcomes in humans.[9]
The HNG analogue: 1,000× more potent
Humanin-glycine (HNG) contains a single substitution: serine at position 14 replaced by glycine. This produces up to 1,000-fold greater potency depending on the assay, making HNG the standard tool compound for humanin research. Virtually all in vivo animal studies use HNG rather than native humanin because the dose required to achieve effects is substantially lower, reducing experimental confounds.[8] Other analogues include colivelin (fusion with ADNF, producing synergistic effects) and HNGF6A (additional phenylalanine→alanine substitution at position 6).
Mechanisms of Action
Extracellular receptor systems
Extracellular humanin regulates cellular survival, metabolism, and inflammation via two types of cell surface receptors: a trimeric receptor involving CNTFR/WSX-1/gp130 (relaying signals through the STAT3 signalling pathway), and FPRL1/FPR2 (relaying signals through the ERK1/2 signalling cascade).[5][6] The CNTFR/WSX-1/gp130 complex is shared with ciliary neurotrophic factor (CNTF) and interleukin-27, placing humanin in the cytokine/neurotrophic factor receptor space. STAT3 activation drives anti-apoptotic gene expression, pro-survival cytokine production, and insulin sensitivity regulation.
Intracellular interactions
BAX antagonism: Humanin directly binds BAX, the pro-apoptotic Bcl-2 family protein responsible for mitochondrial outer membrane permeabilisation — the committed step in intrinsic apoptosis. By preventing BAX translocation and oligomerisation, humanin can block apoptotic execution even after upstream death signals have been received. IGFBP-3 binding: Humanin binds IGFBP-3’s C-terminal domain, preventing its nuclear import and thereby suppressing IGFBP-3-mediated apoptosis. This also positions humanin as a modulator of the GH/IGF-1 axis. Chaperone activity: The chaperone-like function of humanin — interacting with Aβ oligomers and inhibiting amyloid fibril growth — provides an additional mechanistic explanation for neuroprotection in Alzheimer’s models, and also inhibits islet amyloid polypeptide (IAPP) misfolding relevant to type 2 diabetes.[8]
Physiological Regulation and Longevity Associations
Age-related decline
Humanin levels decline with age — a major risk factor for many of the diseases in which humanin is protective, including Alzheimer’s disease, atherosclerosis, myocardial and cerebral ischaemia, and type 2 diabetes. This decline is consistent across species studied and correlates with mitochondrial DNA copy number decreases with age.[3]
The naked mole-rat exception
Humanin levels are remarkably stable in the naked mole-rat, a model of negligible senescence that lives over 30 years — an extraordinary lifespan for a mouse-sized rodent. Sustained high levels of humanin likely play a pivotal role in the observed negligible senescence in this species.[3]
Centenarians and their children
In children of centenarians, who are more likely to become centenarians themselves, circulating humanin levels are much greater than age-matched controls. Data from newborn cord blood, mitochondrial copy number, and humanin levels suggest that differences in humanin levels may exist starting from birth — supporting the idea that elevated humanin in centenarians may represent a heritable trait rather than simply a consequence of good health.[3]
Inverse correlation with IGF-1 and GH
Humanin levels inversely correlate with circulating GH and IGF-1. The Ecuadorian Laron syndrome cohort (severely GH-resistant individuals with very low IGF-1 and strikingly low cancer rates) has elevated humanin levels — consistent with a model in which humanin is one of the effectors through which reduced GH/IGF-1 signalling extends lifespan.
Preclinical Disease Evidence
Neurodegeneration
The founding indication. Humanin and HNG protect neurons from cell death induced by mutant APP, mutant presenilin-1 and -2, Aβ1-42 peptide, and Aβ1-43 peptide. The protection is specific to Alzheimer’s-relevant insults — suggesting receptor-specific activity rather than generic cytoprotection. HNG reduces tau hyperphosphorylation in 3xTg-AD mice, rescues cholinergic neuron loss, and ameliorates cognitive deficit in multiple AD mouse models. Human epidemiological data shows humanin levels are decreased in Alzheimer’s disease and MELAS, and a SNP in the humanin coding region is associated with lower levels and accelerated cognitive decline.[7]
Cardiovascular
Multiple rodent models of ischaemia-reperfusion injury show humanin and HNG reducing infarct size, cardiac arrhythmia, and mitochondrial dysfunction. Humanin also prevents atherosclerotic plaque progression in ApoE-deficient mice. Humanin is expressed in human vascular walls, and expression is reduced in vascular disease states.[3]
Metabolic/diabetes
Humanin improves insulin sensitivity via central STAT3 signalling (reducing hepatic glucose output), inhibits IAPP misfolding relevant to β-cell loss in type 2 diabetes, and HNG treatment in middle-aged mice improves metabolic parameters including visceral fat reduction and lean mass preservation, with decreased IGF-1 and inflammatory markers.[4]
The Cancer Ambiguity
⚠️ Humanin is upregulated in gastric cancer and bladder cancer with opposite anticipated effects — promoting and inhibiting tumour progression respectively. In some preclinical models, HNG protects healthy cells from chemotherapeutic toxicity without impeding anti-tumour efficacy. However, other preclinical studies show that systemic humanin treatment promotes tumour progression. These findings suggest that the effects of humanin are cancer-type dependent.[9]
This bidirectional cancer relationship is the most important safety uncertainty for humanin. Humanin activates ERK1/2, AKT, and JAK2/STAT3 — pathways that drive cell survival in healthy cells but are also drivers of proliferation and survival in many cancer cells. The Laron syndrome data is somewhat reassuring, but this population is exceptional in multiple ways beyond humanin levels, and extrapolation is speculative.
Evidence Levels: What Is and Is Not Known
| Domain | Evidence strength | Key limitation |
|---|---|---|
| Neuroprotection (AD models) | Multiple independent labs, consistent across cell culture + rodent models | No human trials; AD mouse models notoriously fail to translate |
| Cardioprotection (I/R injury) | Rodent and one porcine model | No human trials |
| Longevity (animal) | C. elegans lifespan extension; mouse healthspan parameters | Worm → mouse → human translation not validated |
| Longevity (human observational) | Centenarian offspring data; inverse Laron syndrome correlation | Correlation; causation not established |
| Cancer safety | Mixed — protective in some contexts, potentially tumour-promoting in others | Unresolved by any human data |
| Human dosing and PK | Not characterised | No pharmacokinetic studies in humans |
Common Misconceptions
“Humanin is a natural peptide, so supplementing it is like restoring a deficiency.”
This framing is seductive but premature. Endogenous humanin is produced in specific cells, at specific concentrations, in response to specific stressors, acting locally and systemically in a regulated way. Injecting synthetic humanin bypasses all of this regulatory context. The comparison to vitamin D supplementation — another declining-with-age endogenous molecule where supplementation is therapeutically validated — is not yet justified for humanin.
“The centenarian data proves humanin extends life.”
It shows an association. Children of centenarians have higher humanin. So do naked mole-rats. These are suggestive correlations in humans and experimental lifespan extension in C. elegans. The causal direction — do high humanin levels produce longevity, or do longevity-promoting genetic backgrounds produce high humanin — is not resolved.
“HNG is 1,000× more potent, so it’s the better version to take.”
The 1,000-fold potency difference is measured in specific cell culture assays. It does not mean HNG is 1,000 times better or safer for any human application. Whether this translates to clinical superiority, and what the safety profile difference is, has not been studied in humans.[8]
“Because humanin is produced by the body, it must be safe.”
Insulin is produced by the body. Cortisol is produced by the body. Both can cause serious harm when administered exogenously at the wrong dose. The fact that humanin is endogenous tells us nothing about the safety of injecting pharmacological doses.
Frequently Asked Questions
Does humanin cross the blood-brain barrier?
An important open question for any claimed neuroprotective application. Some evidence suggests humanin can reach the CNS when administered peripherally, particularly under conditions of increased blood-brain barrier permeability as occurs in neuroinflammation. HNG, being more stable, may have better CNS access. However, CNS penetration in healthy humans following subcutaneous injection has not been characterised.
What is CohBar, and is it relevant?
CohBar was a biopharmaceutical company focused on MDP-derived therapeutics, co-founded by Pinchas Cohen and Nir Barzilai, two of the key humanin researchers. It advanced MDP-derived peptides toward clinical development — including CB4209 (an MOTS-c analogue for NASH/obesity). CohBar encountered clinical and financial difficulties and was acquired. The existence of CohBar represents the most credible attempt to translate MDP biology into human therapy, but as of 2026 no MDP-derived drug has reached regulatory approval.
How does humanin relate to MOTS-c?
Both are mitochondrial-derived peptides but encoded from different mitochondrial genes (humanin from 16S rRNA; MOTS-c from 12S rRNA) and have complementary functions. MOTS-c is primarily metabolic — exercise mimetic, AMPK activator, insulin sensitiser. Humanin is primarily cytoprotective and neuroprotective. They represent different arms of a mitochondrial stress-response signalling network.[4]
Key Takeaways
- Humanin is a genuine biological discovery — not a synthetic pharmaceutical candidate but an endogenous mitochondrial-encoded peptide with demonstrated circulating presence in humans and meaningful epidemiological associations with longevity and disease. The field it opened (mitochondrial-derived peptides) is one of the most active areas of aging biology.[1]
- The preclinical evidence is real, broad, and consistent across independent laboratories. The neuroprotective, cardioprotective, metabolic, and lifespan-extending effects in model organisms represent reproducible findings. This earns humanin serious scientific consideration.[7]
- ⚠️ There are no human clinical trials. This is not a minor caveat — it is the central limitation. All efficacy claims are from cell culture or animal models. The history of preclinical biology translating to clinical failure is long and sobering.
- The HNG analogue (S14G-humanin) is the dominant research compound, not native humanin. Most in vivo data comes from HNG. Research chemical “humanin” of unspecified form is not necessarily the compound used in published studies.[8]
- ⚠️ The cancer safety question is genuinely unresolved. The same pro-survival signalling that makes humanin cytoprotective in neurons and cardiomyocytes could, in principle, support tumour cell survival. Until human safety data exists, this risk cannot be quantified.[9]
- Humanin exemplifies the gap between compelling biology and clinical readiness. Its discovery story is among the most remarkable in recent molecular medicine. Its preclinical profile is impressive. But compelling biology and animal data is a description shared by hundreds of compounds that have failed in human trials.
References
Discovery
- Hashimoto Y, et al. A rescue factor abolishing neuronal cell death by a wide spectrum of familial Alzheimer’s disease genes and Abeta. Proceedings of the National Academy of Sciences. 2001;98(11):6336–6341.
- Niikura T, Chiba T, Aiso S, Matsuoka M, Nishimoto I. Humanin: after the discovery. Molecular Neurobiology. 2004;30(3):327–340.
MDP Biology and Longevity
- Yen K, Mehta HH, Kim SJ, et al. The mitochondrial derived peptide humanin is a regulator of lifespan and healthspan. Aging. 2020. PMC7343442. doi: 10.18632/aging.103534
- Bhatt S, et al. Mitochondria-derived peptides in aging and healthspan. Journal of Clinical Investigation. 2022. doi: 10.1172/JCI158449
Mechanisms and Receptor Biology
- Sreekumar PG, et al. Humanin: a harbinger of mitochondrial-derived peptides? PMC3641182. 2013.
- Ying G, et al. Humanin, a newly identified neuroprotective factor, uses the G protein-coupled formylpeptide receptor-like-1 as a functional receptor. Journal of Immunology. 2004;172(11):7078–7085.
Neuroprotection Reviews
- Neuroprotective Action of Humanin and Humanin Analogues: Research Findings and Perspectives. Biology. 2023;12(12):1534. PMC10740898
HNG Analogue
- Okada AK, et al. The Mitochondrial-Derived Peptides, HumaninS14G and Small Humanin-like Peptide 2, Exhibit Chaperone-like Activity. Scientific Reports. 2017. doi: 10.1038/s41598-017-08372-5
Aging and Disease Reviews
- Humanin and Its Pathophysiological Roles in Aging. Biology. 2023;12(4):558.
Key Investigators
- Ikuo Nishimoto, PhD — Keio University (deceased); discovered and named humanin; coined the name to express hope for restoring humanity to Alzheimer’s patients.
- Pinchas Cohen, MD — USC Leonard Davis School of Gerontology; major contributor to humanin biology, the MDP field, centenarian data, and co-founder of CohBar Inc.
- Kelvin Yen, PhD — USC; lead author on the C. elegans and mouse lifespan/healthspan papers; ongoing work on MDP clinical translation.
- Nir Barzilai, MD — Albert Einstein College of Medicine; centenarian biology, IGF-1 longevity work, and humanin centenarian data; co-founder of CohBar Inc.
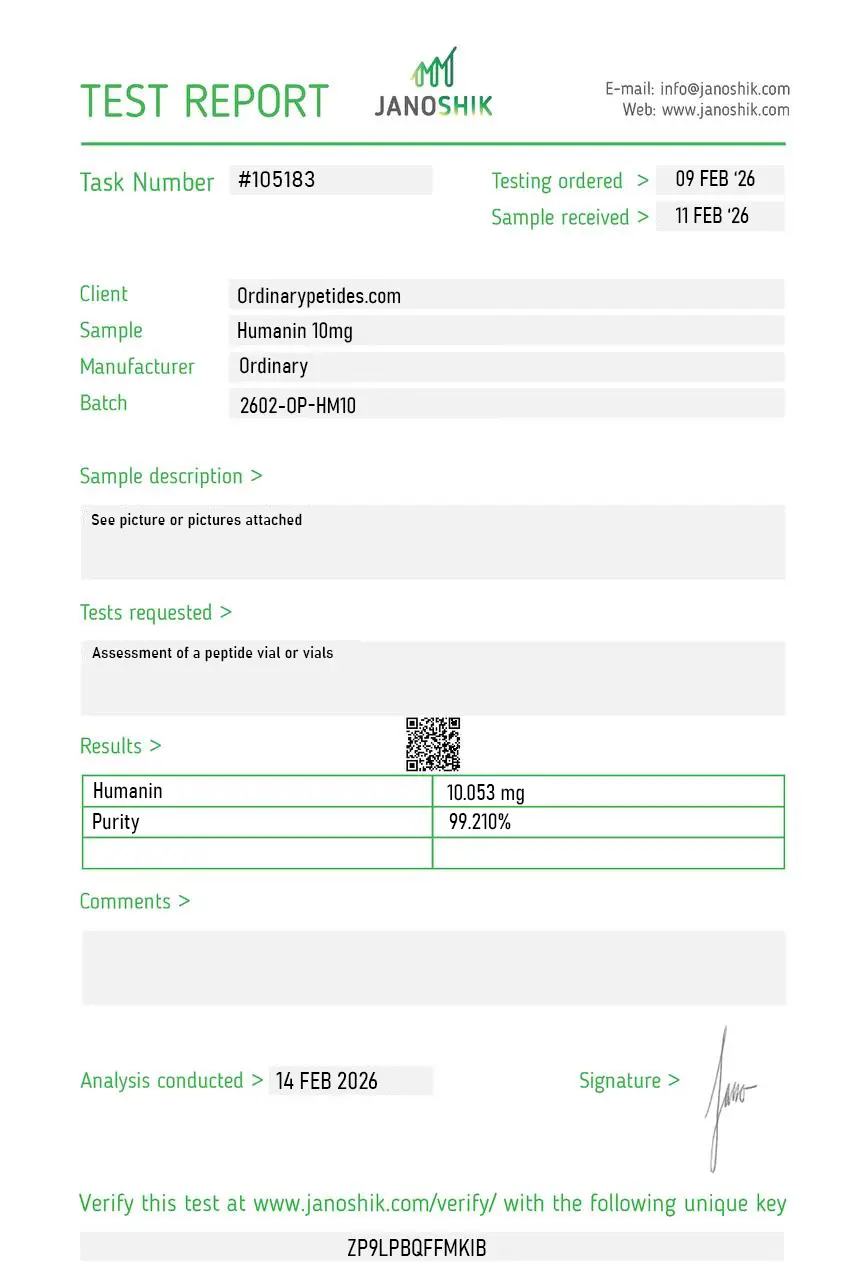
Certificate of Analysis
An independent test report is available for Humanin 10mg. This report provides batch-level documentation and analytical verification information for research reference.
Based on 1 reviews
5.0
The mitochondrial-derived-peptide framing is what we actually study — Humanin is encoded within the 16S mitochondrial rRNA gene, an open reading frame embedded in what was assumed to be purely structural RNA, and that origin opened the whole MDP field including MOTS-c and the SHLPs. For probing the broader mitochondrial-genome-as-signaling-source biology, Humanin is the founding tool because it was the first discovered. The material delivered the expected anti-apoptotic activity in our BAX-mediated cell-death model.
Humanin (HN) is a naturally occurring 21 to 24-amino acid peptide — the exact length depends on whether it is translated within the mitochondria (21 amino acids) or the cytoplasm (24 amino acids) — encoded within a small open reading frame in mitochondrial DNA, specifically within the 16S ribosomal RNA gene (MT-RNR2). It was first identified in 2001 by Japanese researchers who discovered it in healthy neurons from the brains of Alzheimer's disease patients, where it was acting as a survival factor protecting neurons against amyloid-beta toxicity. This discovery was foundational — Humanin was the first peptide shown to be encoded directly by mitochondrial DNA with systemic biological activity, establishing the entire field of mitochondrial-derived peptides (MDPs). It is highly conserved across chordate species, underscoring its evolutionary importance. Humanin levels decline progressively with age in both rats and humans, suggesting it plays a role in the aging process itself.
A commonly listed Humanin sequence is MAPRGFSCLLLLTSEIDLPVKRRA, which is 24 amino acids long. Some reference sources note that Humanin-related forms can vary in length, but the standard Humanin product listing is often this 24-residue sequence.
Humanin is commonly sold as a lyophilized peptide powder. Multiple product pages describe the material in lyophilized form rather than as a ready-to-use liquid.
Reported purity depends on the supplier, but Humanin product pages commonly list purity in the >95% to ≥99% by HPLC range. Because that number is supplier- and lot-specific, the exact value should be taken from the batch documentation for the product you buy.
Many Humanin sellers state that a Certificate of Analysis (COA) is available, often with HPLC and mass spectrometry data. Some pages say the COA is provided with the product, while others say it is available per lot or on request.
Storage instructions vary slightly by vendor, but the common guidance is to store lyophilized Humanin below about -18°C to -20°C, keep it dry/desiccated, and avoid repeated freeze-thaw cycles. One product page also states that, after reconstitution, short-term storage at 4°C for 2 to 7 days may be used, with longer-term storage below -18°C.
Commercial Humanin peptide products are commonly labeled for research use only and not for human or animal use. Several product pages state this explicitly.
Depending on the seller, Humanin products may come with or link to documents such as a COA, SDS/MSDS, and a datasheet or product specification page. The exact document set depends on the supplier.
Humanin operates through multiple receptor systems and intracellular pathways simultaneously. Extracellularly it binds two distinct receptor complexes — the formyl peptide receptor-like 1 (FPRL1), a G protein-coupled receptor, and a trimeric receptor complex consisting of ciliary neurotrophic factor receptor alpha (CNTFRα), the cytokine receptor WSX-1, and the transmembrane glycoprotein gp130. Activation of these receptors triggers downstream signaling through JAK2/STAT3, PI3K/Akt, MAPKs, and JNK pathways — collectively inhibiting programmed cell death and promoting cellular survival. Intracellularly it interacts with pro-apoptotic Bcl-2 family proteins including BAX and tBID, physically binding them and preventing their activation of the mitochondrial apoptotic pathway. It also interacts with IGFBP-3, modulating IGF-1 bioavailability and connecting it to the broader GH-IGF axis. Its net effect across these mechanisms is cytoprotection — shielding cells from stress-induced death through oxidative damage, serum starvation, hypoxia, ischemia-reperfusion injury, and neurotoxic insults.
Neuroprotection is Humanin's most extensively studied application. In Alzheimer's disease models it protects neurons from amyloid-beta and other AD-relevant toxins, and the potent analog Humanin G (HNG) — where serine at position 14 is substituted with glycine, creating a 1,000-fold more potent variant — reduced amyloid accumulation and improved cognitive deficits in transgenic mouse models intranasally administered for three months. In Parkinson's disease and other neurodegenerative models it has reduced neuronal apoptosis with mixed but generally encouraging results. Metabolic health is a second major area — Humanin infused into the brains of diabetic rats significantly improved insulin sensitivity in both liver and skeletal muscle, and it reduces several markers of age-related metabolic dysfunction. Cardiovascular protection through its anti-apoptotic effects in ischemia-reperfusion models has been documented. Reproductive health — protecting germ cells from apoptosis induced by chemotherapy agents — has been studied. Longevity research shows Humanin-transgenic mice have altered aging phenotypes, and elevated Humanin levels correlate with longevity in centenarian offspring studies.
Both are mitochondrial-derived peptides from the same MT-RNR2 genomic region and are frequently discussed together as the two most studied MDPs. Their functional emphases differ somewhat — MOTS-c is more specifically associated with mitochondrial biogenesis, AMPK activation, and metabolic flexibility particularly in skeletal muscle and the nucleus, while Humanin focuses more on Nrf2 pathway activation, cytoprotection, and anti-apoptosis. Genetic studies of longevity have more directly implicated Humanin variants in human lifespan determination. They are considered complementary rather than redundant — working together on different aspects of mitochondrial health and cellular resilience.
As a research compound Humanin is given by subcutaneous injection. Research protocols typically cite 5 to 10 mg per week divided across two to three injections. Animal studies have also used intranasal and intracerebroventricular administration, particularly for neurological applications. It is available as a lyophilized research peptide. There is no standardized human clinical dosing as it has not completed human clinical trials. The potent analog HNG is also available through research peptide suppliers and is considered more active per unit dose.
Humanin has a favorable safety profile in available research given its endogenous nature and the physiological role it plays in cellular homeostasis. It does not disrupt the endocrine system, does not suppress testosterone, is not androgenic, and does not appear to affect the HPG axis. Reported side effects in research contexts are mild — injection site reactions, occasional headache or fatigue at higher doses, and transient digestive upset. The most important safety nuance is the cancer question. Humanin's cytoprotective and anti-apoptotic mechanism — which is beneficial in protecting healthy neurons and cardiac cells — creates a theoretical concern that it could also protect cancer cells from chemotherapy-induced apoptosis. Published research in Scientific Reports found Humanin promoted tumor progression in triple-negative breast cancer models in mice. Separately it has been found upregulated in gastric cancer. These findings create a meaningful paradox — the same BAX-inhibiting and Bcl-2 pathway modulation that protects healthy cells may protect malignant ones. Some research suggests HNG can protect healthy cells from chemotherapy toxicity without impeding anti-tumor efficacy, but this balance has not been reliably demonstrated in human cancer contexts.
People with active cancer or a history of cancer should not use it given the documented pro-tumor signals in specific cancer models — this is a more concrete concern than the theoretical angiogenesis risks associated with BPC-157 or VEGFR2-activating compounds, as direct tumor promotion has been observed in preclinical models. Pregnant or breastfeeding women should not use it. People with significant metabolic disorders including insulin-dependent diabetes should be monitored carefully given Humanin's direct effects on insulin sensitivity. It is not FDA-approved for any therapeutic indication and has no completed human clinical trials.





