





Glutathione
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Glutathione: A Foundational Tripeptide With Real Biology Behind It and an Evidence Base Worth Reading Carefully
Glutathione is not a "magic detox," but one of the foundational tripeptides of cellular biochemistry, which in the research context is linked to redox regulation, antioxidant defense, and the neutralization of reactive compounds. That is precisely why it appears so often in conversations about health, skin, and aging — the molecule is genuinely fundamental, not something invented by marketers on a bad day.
In published observations, oral and topical forms showed modest and often reversible cosmetic effects on skin tone, but without turning that signal into a universal story about "rejuvenation." In the clinical context, the topic is especially important through precursors, above all NAC, in acetaminophen overdose — and this is exactly the kind of case where biochemistry is genuinely tied to practice.
At the same time, for IV skin-lightening, general "detox," and broad anti-aging expectations, the evidence base is noticeably weaker than market promises make it sound. If you are interested in molecules with strong scientific logic and a substantial research history, glutathione belongs exactly in that category. What makes it compelling is not loud promises, but the fact that there is real biology behind it.
Glutathione (GSH): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Glutathione is not like the other compounds in this series. It is not a synthetic peptide designed by a pharmaceutical laboratory. It is not a growth factor secretagogue or a senolytic. Glutathione is a tripeptide present in virtually every cell in every living organism — the most abundant non-protein thiol compound in animal cells, present at millimolar concentrations intracellularly and essential for life. Mice lacking the ability to synthesise it die before birth. It is central to antioxidant defence, xenobiotic detoxification, immune function, DNA repair, and redox signalling across every organ system.
The complexity in this article arises from a different question: does supplementing glutathione through oral, topical, or intravenous routes meaningfully raise tissue glutathione levels, and does that produce clinically relevant benefits? The answers diverge sharply by route:
- Oral glutathione: Modest evidence of some benefit; bioavailability is limited but not zero; reasonable evidence for skin pigmentation effects at doses studied; generally safe.
- Topical glutathione: Moderate evidence for skin-lightening effects in small trials; good local safety profile.
- ⚠️ Intravenous glutathione: Rapidly growing use for skin lightening and general wellness; evidence of efficacy is weak and conflicting; evidence of harm is real and serious (anaphylaxis, liver failure, kidney failure, Stevens-Johnson syndrome reported); the FDA’s Category 2 placement reflects genuine safety concerns.
| At a glance | |
|---|---|
| Chemical name | Gamma-L-glutamyl-L-cysteinylglycine |
| Abbreviation | GSH (reduced), GSSG (oxidised dimer) |
| Structure | Tripeptide: glutamate–cysteine–glycine with unusual γ-peptide bond |
| Molecular weight | 307 Da |
| Endogenous | Yes — most abundant non-protein thiol in all animal cells |
| Intracellular concentration | 0.5–10 mM (cytosol); dramatically higher than extracellular (~2–20 µM) |
| Age-related decline | Yes — GSH levels decline with age across tissues |
| Primary endogenous functions | Antioxidant defence; xenobiotic conjugation; redox signalling; immune function; DNA repair |
| Oral supplementation | Limited but non-zero bioavailability; some evidence of skin effects |
| Topical use | Moderate skin-lightening evidence in small RCTs |
| IV use | ⚠️ Weak efficacy evidence; serious safety concerns; FDA Category 2 |
| FDA status (IV) | ⚠️ Category 2 bulk drug substance — cannot be legally compounded |
The Biochemical Foundation: What Glutathione Actually Does
Structure and synthesis
Glutathione’s sequence is Glu-Cys-Gly. Its most distinctive chemical feature is the γ-peptide bond linking glutamate to cysteine — an unusual bond that protects glutathione from hydrolysis by normal intracellular peptidases, giving it a longer intracellular half-life than a conventional tripeptide.[1] The rate-limiting step in synthesis is the GCL reaction, which is tightly feedback-inhibited by GSH itself. When intracellular GSH is adequate, new synthesis slows. This feedback loop is one reason why simply flooding the cell with exogenous GSH may not raise tissue levels as expected: the cell’s own synthesis down-regulates in response.
The GSH/GSSG redox couple
Glutathione exists in two forms: reduced GSH (the active antioxidant form) and oxidised GSSG. In healthy cells, more than 90% of total glutathione is in the reduced GSH form. The antioxidant cycle works as follows: GSH donates an electron to neutralise reactive oxygen species, becoming GSSG. Glutathione reductase then reduces GSSG back to GSH using NADPH, completing the cycle.[3]
Xenobiotic detoxification
Glutathione S-transferases (GSTs) conjugate GSH directly to electrophilic xenobiotics, heavy metals, and endogenous compounds — rendering them more water-soluble and facilitating excretion. This is the primary detoxification mechanism in the liver for many drugs, industrial chemicals, and environmental toxins. The liver is the major site of glutathione synthesis and export precisely because of this central detoxification role.[2]
The intracellular vs. extracellular concentration gradient
Intracellular concentrations range from 0.2 to 10 mM, while cerebral spinal fluid concentration is approximately 4 µM — approximately 250–500× lower than intracellular levels. Thus intracellular synthesis is necessary for maintaining the large concentration difference. The practical implication: orally or intravenously administered glutathione does not simply diffuse into cells. GSH is hydrolysed extracellularly by γ-glutamyl transpeptidase (GGT) on cell surfaces. Cells must synthesise their own GSH intracellularly from precursor amino acids — this is why supplementation strategies that increase cysteine availability (such as N-acetylcysteine) may be more effective at raising tissue GSH than supplementing GSH directly.[1]
Age-Related Decline and Disease Associations
Glutathione levels decline measurably with age across tissues. GSH deficiency contributes to oxidative stress, which plays a key role in aging and the pathogenesis of many diseases including Alzheimer’s disease, Parkinson’s disease, liver disease, cystic fibrosis, and sickle cell anemia.[2]
Parkinson’s disease: GSH is selectively depleted in the substantia nigra of Parkinson’s patients — the brain region containing the dopaminergic neurons that degenerate in this condition. This depletion is only detected in the substantia nigra, whereas complex I deficiency is widespread, suggesting GSH depletion plays a specific and localised role.[5]
Liver disease: Alcoholic liver disease — including fatty liver, fibrosis, cirrhosis, and hepatitis — is associated with GSH depletion, which is why IV glutathione has an approved indication for these conditions in some countries (India, for example).
Cancer paradox: Elevated GSH levels are observed in many cancer cells — a feature that helps them resist oxidative stress and chemotherapy. Lung cancer, larynx cancer, mouth cancer, and breast cancer exhibit higher concentrations (10–40 mM) of GSH compared to healthy cells. This creates a nuanced picture: GSH depletion contributes to cancer initiation by impairing DNA repair; but elevated GSH in established cancer cells promotes their survival and drug resistance.[2]
The Skin-Lightening Mechanism
The anti-melanogenic mechanism of glutathione is the best-characterised basis for its most widely studied supplementation use. It works through several converging pathways. Tyrosinase inhibition: GSH chelates the copper in tyrosinase’s active site (via its thiol group) and directly inhibits the enzyme’s activity, reducing melanin production. Raper-Mason pathway shift: GSH shifts melanin production toward pheomelanin (yellow/red, lighter pigmentation) from eumelanin (brown/black) by competing with DOPA for enzymatic processing. Antioxidant suppression of melanogenesis: GSH’s antioxidant activity reduces ROS-driven melanogenesis, particularly in sun-exposed skin.[6]
Evidence by Route of Administration
Oral glutathione
Bioavailability: Limited but present. Some studies show measurable increases in blood GSH after oral supplementation; others do not. Liposomal and acetylated forms show better absorption. The effective dose appears to be 250–500 mg daily, with effects taking weeks to develop.
Skin-lightening evidence: Five randomized controlled trials and a single open-arm clinical study on oral glutathione at doses of 250–500 mg/day showed a significant reduction in the melanin index compared to placebo. The combination of topical 2% glutathione plus oral glutathione was superior to monotherapy alone.[6] These are real RCTs with placebo controls — the most rigorous evidence in the glutathione supplementation literature. Effect sizes are modest to moderate, durations are short (mostly 4–12 weeks), and long-term sustainability is not established.[10][11]
Safety: Oral glutathione at studied doses appears safe. Reported adverse effects are minimal — occasional GI discomfort. No serious adverse events have been documented at standard doses.
Topical glutathione
A systematic review identified only five clinical trials specifically on topical glutathione. Across these trials, topical 2% glutathione produced measurable melanin index reduction; the effect was localised (applying to treated area only) vs. generalised with oral; skin texture and radiance improvements were reported; and safety was consistently good in all trials.[8]
Intravenous glutathione
⚠️ This is where the evidence picture changes dramatically. There was only one placebo-controlled study on IV glutathione for skin lightening, which did not achieve statistical significance (p=0.054). The 2025 systematic review in the International Journal of Dermatology concluded IV glutathione is “contraindicated” for skin lightening.[6]
The fundamental pharmacokinetic problem is that intravenously administered GSH circulates transiently in plasma and is rapidly degraded by GGT on cell surfaces into its component amino acids. Whether this substrate provision reliably raises intracellular GSH levels is not demonstrated in the IV skin-lightening literature.
Safety concerns: serious and documented
| Adverse event | Severity |
|---|---|
| Anaphylaxis / anaphylactoid reaction | ⚠️ Potentially life-threatening |
| Hepatotoxicity / liver failure | ⚠️ Severe |
| Renal failure | ⚠️ Severe |
| Stevens-Johnson syndrome | ⚠️ Potentially life-threatening |
| Thyroid dysfunction | Moderate |
| Neurological symptoms | Variable |
The FDA issued a specific safety warning in 2023 regarding glutathione from Letco Medical — a major supplier to compounding pharmacies — after safety concerns were identified.[14] Contamination and lack of standardised manufacturing are additional risks on top of the pharmacological safety concerns.
The reductive stress concern: An underappreciated paradox of high-dose glutathione supplementation is the risk of reductive stress — when the redox balance tilts too far toward reduction, it can disrupt normal cell signalling pathways that rely on physiological ROS, impair mitochondrial function, and paradoxically increase superoxide production. High-dose, non-physiological glutathione supplementation has the potential to push cells out of optimal redox balance.
Summary by route
| Route | Best evidence | Typical effect | Safety | FDA compounding status |
|---|---|---|---|---|
| Oral | 5 RCTs (skin lightening) | Modest, variable | ✅ Good | Not specifically restricted |
| Topical | 5 clinical trials | Moderate, localised | ✅ Good | Cosmetic use unrestricted |
| Intravenous | 1 placebo-controlled trial (NS) | Not established | ⚠️ Serious concerns documented | ❌ Category 2 — cannot be compounded |
Applications Beyond Skin Lightening
Neurodegenerative disease
The connection between GSH depletion and neurodegeneration is scientifically well-established, but the therapeutic implication remains difficult. IV or oral GSH does not easily cross the blood-brain barrier in significant quantities. N-acetylcysteine (NAC), a GSH precursor, more reliably raises brain GSH than GSH itself. Several Phase 2 trials of IV glutathione in Parkinson’s disease have been conducted with mixed and generally modest results that have not advanced to Phase 3.[5]
Liver disease
This is the best-established therapeutic use of IV glutathione. In alcoholic liver disease, hepatic GSH is depleted and IV GSH supplementation has demonstrated benefit in some trials. India’s CDSCO has approved IV glutathione specifically for alcoholic fatty liver, fibrosis, cirrhosis, and hepatitis — a legitimate medical use with some evidence base, categorically different from IV glutathione for skin lightening or wellness.
The Oral Bioavailability Problem and Partial Solutions
If the goal is to raise intracellular tissue glutathione, several approaches may outperform oral GSH supplements directly. Liposomal GSH: Encapsulation protects from gut hydrolysis; some studies show improved plasma and white blood cell GSH levels. Acetylated GSH (S-acetyl-glutathione): The acetyl group protects the thiol from oxidation and may improve absorption. GSH precursors (NAC, whey protein): Provide cysteine directly for intracellular GSH synthesis, bypassing the bioavailability problem entirely. NAC has an extensive evidence base as a GSH precursor, including as an antidote for paracetamol (acetaminophen) overdose by restoring hepatic GSH.
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) — IV compounding | ⚠️ Category 2 (September 2023) — cannot be legally compounded under 503A; specific product safety warning issued [13] |
| FDA (USA) — oral supplement | Sold as dietary supplement without drug approval |
| FDA (USA) — topical cosmetic | ✅ Permitted as cosmetic ingredient without drug approval |
| India (CDSCO) | IV glutathione approved for specified alcoholic liver conditions |
| WADA | Not specifically listed (verify current year’s list) |
What Is Established and What Is Not
| ✅ Established | ❌ Not established |
|---|---|
| Glutathione is essential for life — endogenous GSH is not optional [1] | Whether oral supplementation meaningfully raises tissue GSH levels |
| GSH levels decline with age and in many disease states [2] | Whether supplementation reverses age-related decline in any clinically meaningful way |
| Oral GSH reduces melanin index in 5 RCTs [10][11] | Long-term sustainability of oral skin-lightening effects |
| Topical GSH reduces localised pigmentation [8] | Clinical benefits of IV GSH for any wellness/anti-aging indication |
| IV GSH has documented serious adverse events [6] | Safe and effective IV dosing protocol for any indication |
| IV GSH is Category 2 (safety concerns) in US compounding [13] | Whether liposomal GSH meaningfully outperforms standard oral |
| NAC more reliably raises tissue GSH than direct GSH | Whether restoring GSH halts Parkinson’s progression |
Common Misconceptions
“IV glutathione is more effective than oral because it goes directly into your bloodstream.”
More bioavailable in the blood — yes. More effective at raising intracellular tissue glutathione — not established. IV GSH is rapidly degraded extracellularly. The one placebo-controlled IV trial did not show statistically significant skin-lightening effects.[6]
“Glutathione is the master antioxidant, so more is always better.”
Intracellular GSH levels are tightly regulated by feedback inhibition. Supplementing externally does not simply override this regulation. High-dose non-physiological redox intervention can produce reductive stress and mitochondrial dysfunction.
“It’s natural and endogenous, so IV glutathione must be safe.”
⚠️ Endogenous at intracellular concentrations bears no relationship to the safety of IV injection of supraphysiological doses. The serious adverse events documented with IV glutathione — anaphylaxis, liver failure, renal failure, Stevens-Johnson syndrome — are well-documented case reports.[6] The FDA’s Category 2 placement is based on real safety signals.[13]
“NAC and glutathione are interchangeable.”
N-acetylcysteine (NAC) is a cysteine precursor that reliably raises intracellular glutathione by providing the rate-limiting amino acid for GSH synthesis. It has a much stronger evidence base than direct glutathione supplementation for most indications. They are related but not interchangeable — NAC works upstream of GSH synthesis and may be more effective for raising tissue GSH.
Frequently Asked Questions
Should I take oral glutathione supplements?
For general wellness, the evidence base is modest. The skin-lightening evidence is the strongest available for any supplemental form. Safety appears acceptable at studied doses (250–500 mg/day).[10] Consulting a qualified healthcare provider is appropriate.
What is the safest approach to supporting glutathione status?
The most evidence-backed approaches are indirect: providing GSH precursors (NAC, whey protein, cysteine-rich foods), reducing factors that deplete GSH (alcohol, smoking, excessive oxidative stress), and regular aerobic exercise, which upregulates endogenous GSH synthesis.
Is IV glutathione legal in the US?
For skin lightening and general wellness use through compounding pharmacies under the 503A framework: no, since September 2023 (Category 2).[13] For legitimate medical indications in specific clinical settings, the regulatory picture is more complex. Consult a qualified clinician about the current legal status for any specific proposed use.
Can glutathione treat Parkinson’s disease?
GSH depletion in the substantia nigra is well-documented in Parkinson’s.[5] Multiple Phase 2 trials have explored IV glutathione as a treatment with mixed results. No Phase 3 trial has been conducted. It is not an established treatment. The most promising direction is likely restoring GSH through precursor supplementation rather than direct GSH administration.
Key Takeaways
- Glutathione’s endogenous biology is among the most important in all of biochemistry — it is genuinely essential for life, irreplaceable in antioxidant defence and detoxification, and its depletion contributes to a wide range of serious diseases.[1][2]
- The supplementation evidence is route-dependent and highly variable. Oral and topical glutathione have real but modest evidence for skin-lightening effects.[10][11] IV glutathione has weak efficacy evidence and serious documented safety concerns.[6]
- ⚠️ IV glutathione is the most widely misrepresented form. The marketing presents it as a potent systemic rejuvenator; the evidence shows one placebo-controlled trial that did not reach statistical significance and a catalogue of serious adverse events including anaphylaxis and organ failure.
- ⚠️ The FDA’s Category 2 designation for IV compounded glutathione reflects genuine safety data. This is not over-regulation of a harmless supplement; it is a regulatory response to real adverse event reports and inadequate safety characterisation.[13]
- NAC is the better-supported strategy for raising tissue GSH in most clinical contexts. As a cysteine precursor that works upstream of the rate-limiting synthesis step, it has a more reliable mechanistic basis for increasing intracellular GSH than exogenous GSH itself.
- The skin-lightening use of glutathione raises important ethical considerations beyond the clinical evidence. The widespread promotion of skin lightening to populations with darker skin tones reinforces colorism. Clinicians recommending glutathione for this purpose should engage with these dimensions honestly.
References
Fundamental Biochemistry
- Lu SC. Glutathione synthesis. Biochimica et Biophysica Acta. 2013;1830(5):3143–3153. PMC3549305
- Ballatori N, et al. Glutathione dysregulation and the etiology and progression of human diseases. Biological Chemistry. 2009. PMC2756154
- Wu G, et al. Glutathione metabolism and its implications for health. Journal of Nutrition. 2004;134(3):489–492. PMID: 14988435
- Glutathione. Wikipedia. en.wikipedia.org/wiki/Glutathione
Neurodegenerative Disease
- Johnson WM, et al. Dysregulation of glutathione homeostasis in neurodegenerative diseases. Nutrients. 2012. PMC3497002
Clinical Evidence Reviews — Skin Lightening
- Sarkar R, Yadav V, Yadav T, et al. Glutathione as a skin-lightening agent and in melasma: a systematic review. International Journal of Dermatology. 2025;64(6):992–1004. doi: 10.1111/ijd.17535. PMID: 39444151
- Alzahrani TF, et al. Exploring the Safety and Efficacy of Glutathione Supplementation for Skin Lightening: A Narrative Review. Cureus. 2025;17(1):e78045. PMC11862975
- Topical glutathione systematic review. 2025. PMC12710870
- Gupta S. Glutathione in dermatology: A bright future or fading hype? CosmoDerma. 2025;5:51.
Key Oral RCTs
- Arjinpathana N, Asawanonda P. Glutathione as an oral whitening agent: a randomized, double-blind, placebo-controlled study. Journal of Dermatological Treatment. 2012;23(2):97–102.
- Weschawalit S, et al. Glutathione and its antiaging and antimelanogenic effects. Clinical, Cosmetic and Investigational Dermatology. 2017;10:147–153.
- Wahab S, et al. Combination of topical and oral glutathione as a skin-whitening agent: a double-blind randomized controlled clinical trial. International Journal of Dermatology. 2021.
Regulatory Sources
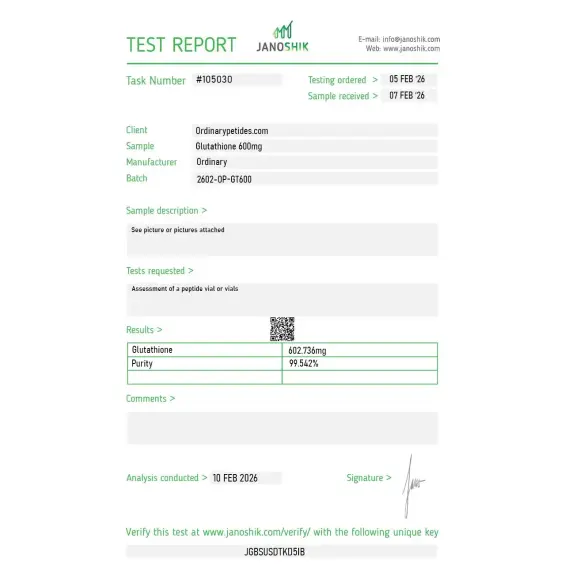
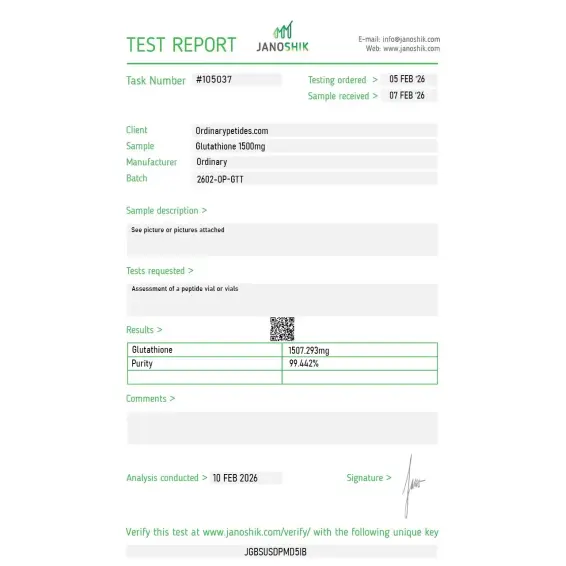
Certificate of Analysis
Independent test reports are available for Glutathione 600mg and 1500mg batches. These reports provide batch-level documentation and analytical verification information for research reference.


Based on 2 reviews
5.0
We use it as the cofactor in glutathione-peroxidase activity assays — GSH is the reducing substrate the enzyme consumes to neutralize peroxides, so characterizing GPx kinetics depends on a clean, fully-reduced GSH supply. The reduced fraction held high enough across orders that our kinetic readouts stayed consistent. For enzyme-cofactor work the reduced-form integrity is the only thing that matters, and it delivered.
The γ-glutamyl linkage is the structurally unusual feature and the reason we work with it specifically — the bond between the glutamate and cysteine is through the side-chain carboxyl, not the standard α-peptide bond, which is what makes GSH resistant to ordinary aminopeptidases and gives it its biological persistence. For studying γ-glutamyl chemistry and the enzymes that actually process it, that non-standard bond is the whole point. The material behaved as authentic γ-glutamyl GSH should in our enzymatic assays.
Yes. It is a tripeptide composed of glutamate, cysteine, and glycine.
No. The clinical standard is N-acetylcysteine, which helps restore glutathione stores and prevent liver injury.
Cautiously, yes, but modestly. For oral and topical forms there are limited data on skin lightening and certain cosmetic effects, but this is not a strong or universal result.
That cannot be said confidently. Precisely for IV forms, the evidence base is weak and the regulatory warnings are the strongest.
No. The biological logic exists, but there is no convincing clinical evidence base for universal anti-aging claims.
The key point is not to confuse glutathione's central role inside the cell with proven benefit from any glutathione supplement or procedure.
Glutathione (GSH) is a naturally occurring tripeptide composed of three amino acids — glutamic acid, cysteine, and glycine — synthesized endogenously by the liver and found in virtually every cell of the human body. It was first identified in 1888 and is often called the body's "master antioxidant" because of its central role in cellular redox balance, detoxification, immune function, and tissue repair. It exists in two forms — reduced glutathione (GSH, the active form) and oxidized glutathione (GSSG) — which are continuously interconverted. Glutathione levels decline with age, chronic illness, environmental toxin exposure, chronic stress, and nutritional deficiency, and this decline is associated with increased oxidative stress and accelerated cellular aging.
Glutathione operates through four primary mechanisms. As a direct antioxidant it scavenges reactive oxygen species (ROS) and reactive nitrogen species, neutralizing free radicals before they damage DNA, proteins, and cell membranes. As an enzymatic cofactor it serves as the essential substrate for glutathione peroxidase enzymes that detoxify hydrogen peroxide and lipid peroxides, and for glutathione S-transferases that conjugate toxic compounds for excretion. As a detoxification agent it binds to heavy metals, drugs, carcinogens, and xenobiotic compounds — forming glutathione conjugates that are exported from cells and eliminated via bile or urine. As a redox network supporter it helps regenerate other antioxidants including vitamins C and E, maintaining the broader cellular antioxidant system. It also plays critical roles in protein folding via regulation of disulfide bonds, immune cell proliferation, and mitochondrial protection.
Glutathione has a meaningful human evidence base across several conditions — more so than most peptides in this series. Intravenous glutathione has been shown to reduce cisplatin-induced peripheral neuropathy in cancer patients, a finding strong enough to appear in oncology guidelines. IV administration has demonstrated improvements in walking distance and pain in peripheral artery disease. Inhaled nebulized glutathione has been studied in cystic fibrosis patients where intestinal glutathione deficiency contributes to malabsorption and inflammation — supplementation reduced intestinal inflammation and improved growth in children. In HIV/AIDS it has been studied for AIDS-related weight loss and immune support. It has been evaluated in Parkinson's disease given the well-documented glutathione depletion in the substantia nigra. Skin lightening applications through oral and IV glutathione have been studied in multiple randomized controlled trials showing measurable melanin reduction, primarily by shifting melanin synthesis from dark eumelanin toward lighter pheomelanin through tyrosinase inhibition.
Glutathione is available in multiple forms with significantly different bioavailability profiles. Intravenous (IV) administration delivers the molecule directly into circulation and is used in clinical settings for cisplatin neuropathy protection and vascular disease. Intramuscular injection is used in cosmetic and wellness settings particularly for skin lightening. Oral supplementation has historically shown poor bioavailability — standard capsules are substantially degraded by the gastrointestinal tract — but liposomal oral glutathione formulations have shown meaningfully better absorption and are the preferred oral route. Sublingual forms offer some improvement over standard oral. Inhaled nebulized glutathione reaches lung tissue directly and is used in respiratory conditions. Oral doses studied in trials range from 250 to 1000 mg daily. N-acetylcysteine (NAC), a well-established pharmaceutical precursor to glutathione, is frequently preferred by clinicians for systemic glutathione elevation as it is more bioavailable orally and has an extensive safety and clinical record.
Glutathione has a generally favorable safety profile consistent with its endogenous nature. Oral supplementation up to 500 mg daily for up to two months is considered possibly safe with limited reported adverse effects, though long-term safety data is incomplete. Common mild effects include bloating, abdominal cramping, and loose stools. Skin rash has been reported with topical application. A 2025 review and associated case reports raised more significant concerns about high-dose IV glutathione — liver dysfunction was documented in nearly one-third of patients in one review, and a case of systemic inflammatory response syndrome was reported following high-dose IV glutathione infusion in a patient on tirzepatide. A 2024 animal study raised potential concerns about intramuscular injection effects on ovarian tissue in female rats. These findings underscore that while oral supplementation at moderate doses appears reasonably safe, high-dose IV administration carries a different and less well-characterized risk profile than wellness clinic marketing typically acknowledges.
Glutathione levels fall progressively with age — reductions of 30 to 50% in older adults compared to young adults are commonly reported — and this decline correlates with increased markers of oxidative stress, mitochondrial dysfunction, chronic inflammation, and susceptibility to age-related diseases. Depleted levels are documented in Parkinson's disease, Alzheimer's disease, type 2 diabetes, cardiovascular disease, HIV/AIDS, and chronic liver disease. Whether supplementation meaningfully reverses these associations in humans — rather than simply correcting deficiency where it genuinely exists — remains an area of active investigation and debate.
Pregnant or breastfeeding women should avoid supplementation given insufficient safety data. People with asthma should use inhaled glutathione cautiously as bronchospasm has been reported. Those receiving chemotherapy should consult their oncologist before supplementing — while glutathione protects healthy cells from cisplatin toxicity, there are theoretical concerns it could also reduce the effectiveness of chemotherapy against tumor cells by protecting them. People with cancer should not self-supplement without oncologist guidance for this reason. Those with liver disease should use pharmaceutical-grade formulations only under medical supervision. High-dose IV administration should be reserved for medically supervised settings given the liver dysfunction and inflammatory response signals emerging in 2024 and 2025 literature.





