
Orexin B
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Orexin B: The Research Peptide Behind the Brain's "Stay Awake" Signal
Orexin B is a naturally occurring neuropeptide best known in neuroscience as one of the key signaling molecules tied to wakefulness and sleep-wake stability. In the research context, it has been studied as a high-affinity OX2R agonist, with published data linking the orexin system to arousal, REM suppression, motivation, and stress-response signaling across the CNS.
What makes it especially interesting is that orexin biology sits at the center of one of the most important modern sleep discoveries: in narcolepsy type 1, loss of orexin neurons is the core pathology. That is exactly why Orexin B remains such a compelling molecule for researchers — not as a consumer shortcut, but as a window into one of the brain's most powerful wake-regulating systems.
In other words: small peptide, very big neuroscience story.
Orexin B (Hypocretin-2): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Orexin B (also called hypocretin-2, HCRT-2, or OX-B) is a 28-amino acid neuropeptide co-produced alongside Orexin A (hypocretin-1) in a small, anatomically discrete population of approximately 70,000 neurons in the lateral hypothalamus. Together they constitute the orexin/hypocretin system — a master regulatory network for sleep-wake state stability, arousal, appetite, reward, and metabolic homeostasis. The system’s clinical importance is now proven definitively: selective destruction of these ~70,000 neurons causes narcolepsy type 1 (NT1), one of the most debilitating neurological sleep disorders.
The pharmacological story follows two opposing strategies simultaneously: (1) blocking orexin signalling for insomnia via dual orexin receptor antagonists (DORAs) including suvorexant (FDA 2014) and daridorexant (FDA 2022); and (2) restoring orexin signalling for narcolepsy via OX2R-selective agonists. Oveporexton (TAK-861/Takeda) completed two positive Phase 3 trials (September 2025) and received FDA Priority Review — poised to become the first therapy targeting the actual pathophysiology of NT1. Orexin B is the endogenous ligand that preferentially activates OX2R, the receptor subtype responsible for most of the wakefulness-maintaining function.
| At a glance | |
|---|---|
| Names | Orexin B; Hypocretin-2 (HCRT-2); OX-B |
| Length / MW | 28 amino acids; ~2,937 Da |
| Gene | HCRT (prepro-orexin/prepro-hypocretin); chromosome 17q21 in humans |
| C-terminal modification | Amidation (required for full receptor binding; removal abolishes activity) |
| Producing neurons | ~70,000 lateral hypothalamic neurons |
| Primary receptor | OX2R (orexin receptor 2 / HCRTR2) — binds OX-A and OX-B with similar affinity |
| Secondary receptor | OX1R (binds OX-B with ~10–100× lower affinity than OX-A) |
| Approved drugs (antagonists) | ✅ Suvorexant, lemborexant, daridorexant (insomnia) |
| FDA NDA under Priority Review (agonist) | Oveporexton (TAK-861) for narcolepsy type 1 |
Discovery: 1998 and the Simultaneous Discovery Problem
The orexin/hypocretin system was discovered simultaneously by two independent groups in 1998, producing a nomenclature confusion that persists to this day. de Lecea et al. (Scripps Research Institute) characterised the peptides as products of a hypothalamus-specific mRNA and named them hypocretin-1 and hypocretin-2, published in PNAS, January 1998.[1] Sakurai et al. (University of Texas Southwestern) identified the same peptides as orphan receptor ligands and named them orexin-A and orexin-B (from Greek orexis = appetite), published in Cell, February 1998.[2] Both names are correct and used interchangeably in the literature.
The critical follow-up discoveries: Chemelli et al. (1999) — orexin knockout mice develop narcolepsy;[3] Lin et al. (1999) — narcoleptic dog mutation is in the OX2R gene;[4] Nishino et al. (2000) — orexin-A is undetectable in CSF of human narcoleptic patients.[5] These discoveries, within two years of orexin’s initial characterisation, created one of the most complete molecular explanations of any major neurological disorder in history.
Orexin A vs. Orexin B: Structure and Functional Distinction
Both peptides are cleaved from a single precursor, prepro-orexin — a 130-amino acid protein encoded by the HCRT gene. The signal peptide (28 AA) is cleaved during translation, leaving the 102-amino acid mature prepro-orexin, processed to yield the two active peptides.
Orexin A (Hypocretin-1): 33 amino acids; MW ~3,562 Da. Distinctive features: N-terminal pyroglutamyl residue (cyclised glutamine at position 1 — no other mammalian neuropeptide has this); two intrachain disulfide bonds (Cys6-Cys12, Cys7-Cys14) giving a constrained fold; C-terminal amidation. Receptor selectivity: binds OX1R and OX2R with similar high affinity (Kd ~10–20 nM at both).
Orexin B (Hypocretin-2): 28 amino acids; MW ~2,937 Da. No pyroglutamyl modification; no disulfide bonds (linear peptide); C-terminal amidation essential for receptor binding. Receptor selectivity: binds OX2R with high affinity (~20–30 nM); binds OX1R with ~10–100× lower affinity than OX-A. Hcrt1 is a 33-amino acid peptide featuring a pyroglutamyl residue at the N-terminus and C-terminal amidation, whereas Hcrt2 is a 28-amino acid, also C-terminally amidated, peptide of 2,937 Da.[13]
The functional significance of OX1R vs. OX2R selectivity
OX1R: Primarily expressed in the locus coeruleus (norepinephrine neurons), ventral tegmental area, and cortex. Selectively activated by OX-A. OX1R signalling is involved in arousal, stress responses, anxiety, and drug-seeking behaviour. OX2R: Expressed in the tuberomammillary nucleus (TMN, histamine neurons), dorsal raphe, basal forebrain, and throughout brainstem arousal nuclei. The critical receptor for sleep-wake state maintenance and REM suppression. This selectivity explains why narcolepsy in dogs is caused by OX2R loss-of-function mutations (not OX1R); why OX2R-selective antagonists promote sleep; and why OX2R-selective agonists are the primary therapeutic strategy for narcolepsy. Orexin B is thus uniquely OX2R-preferring among the two natural peptides, making it specifically relevant to the wakefulness-maintenance function.
The Orexin System: Anatomy and Circuitry
The entire orexin system is produced by approximately 70,000–80,000 neurons in the lateral hypothalamic area (LHA) and perifornical region. Despite this small number, their axonal projections innervate virtually the entire brain: cortex, thalamus, basal forebrain, tuberomammillary nucleus, dorsal raphe, locus coeruleus, ventral tegmental area, and spinal cord. This single small population coordinates the entire brain’s sleep-wake state through neuromodulatory control of every major monoamine system simultaneously — which is why their loss produces such profound and multi-symptom disease.
The histamine pathway: OX2R’s primary wakefulness mechanism
The most important downstream target of OX2R signalling is the tuberomammillary nucleus (TMN) — the sole source of histamine in the brain. TMN neurons appear to play an essential role in promoting wakefulness; inactivation of the TMN increases sleep, and mice lacking histamine have less wakefulness. Orexins excite TMN neurons, and microdialysis of orexin-A near the TMN increases wakefulness and induces histamine release in the cortex. Of clinical relevance, hypocretin-deficient individuals with narcolepsy have a 44% reduction in CSF histamine concentrations. This mechanistically explains why antihistamines cause drowsiness (blocking the downstream effector of the orexin system) and why narcoleptic patients have reduced CSF histamine (their orexin neurons are lost, providing no TMN stimulation).
Narcolepsy Type 1: The Disease of Orexin Deficiency
Narcolepsy type 1 (NT1) affects approximately 1 in 2,000–4,000 people globally, caused by selective autoimmune destruction of lateral hypothalamic orexin neurons — typically losing 80–95% of these cells. The clinical tetrad: Excessive daytime sleepiness (EDS) — irresistible sleep attacks, often at inappropriate times; Cataplexy — sudden bilateral muscle weakness triggered by strong emotions while remaining conscious (the pathognomonic symptom, caused by REM-like atonia intruding into wakefulness); Hypnagogic hallucinations — vivid dream-like hallucinations at sleep onset; Sleep paralysis — transient inability to move upon waking or falling asleep. All four symptoms reflect the same pathology: without orexin, the brain cannot stably maintain wakefulness or REM sleep — it oscillates inappropriately between them.
Diagnosis: CSF orexin-A (hypocretin-1) below 110 pg/mL is diagnostic of NT1 when cataplexy is present (sensitivity ~87%, specificity ~99%). Orexin-A is measured rather than orexin-B because its CSF concentration is higher and its immunoassay is better standardised; both are produced by the same neurons and both are lost together. Etiology: Strong HLA association (HLA-DQB1*06:02 in >98% of NT1 patients vs. ~25% of the general population); post-infection triggering (multiple cases followed H1N1 influenza infection and the Pandemrix H1N1 vaccine, providing molecular mimicry evidence); CD4+ and CD8+ T cells reactive to orexin neuropeptide fragments found in NT1 patients.
OX2R Structural Biology and Signalling
OX2R is a class A (rhodopsin-family) GPCR coupled primarily to Gq (→ PLCβ → IP3/DAG → Ca²+ mobilisation → PKC activation). Cryo-EM structures of active-state OX2R bound to orexin B reveal that the extended carboxy-terminal segment of the peptide reaches into the core of OX2R to stabilise an active conformation, while small-molecule agonists bind deep inside the orthosteric pocket, making similar key interactions.[12] The C-terminal amidation of orexin B is essential for this receptor-activating interaction — the C-terminal amide forms hydrogen bonds with conserved residues in the OX2R orthosteric binding pocket. This structural insight directly guided the design of synthetic small-molecule OX2R agonists. In TMN histamine neurons, OX2R activation → Gq → PLCb → IP3 → Ca²+ rise → depolarisation; inhibition of KCNQ/M-type K+ channels → increased firing rate; net effect: increased histamine release → sustained cortical arousal.
The Pharmacological Landscape: Antagonists and Agonists
Approved antagonists (for insomnia)
The approved DORAs work by the logical pharmacological opposite of NT1’s pathology — blocking orexin signalling at night to facilitate sleep in people whose orexin system cannot disengage. Suvorexant (Belsomra, Merck, FDA approved 2014): First DORA (dual OX1R + OX2R antagonist); represents a mechanistic revolution — first sleep drug promoting sleep by reducing arousal rather than adding sedation; Schedule IV. Lemborexant (Dayvigo, Eisai, FDA approved 2019): DORA; Schedule IV. Daridorexant (Quviviq, Idorsia, FDA approved 2022): DORA; Schedule IV; clinical data suggesting improvements in both EDS and sleep architecture. Critically, DORAs do not cause respiratory depression — a major advantage over benzodiazepines and barbiturates.
Investigational OX2R agonists (for narcolepsy)
Oveporexton (TAK-861, Takeda) — the clinical leader: Takeda’s Phase 3 studies FirstLight (TAK-861-3001) and RadiantLight (TAK-861-3002) met all primary and secondary endpoints, demonstrating statistically significant improvement across a broad range of NT1 symptoms compared to placebo with P-values of <0.001 across all doses (twice-daily 1 mg and 2 mg) at week 12. The FDA granted Breakthrough Therapy Designation and is reviewing the NDA with Priority Review.[6][9]
The critical preceding story: Takeda’s prior OX2R agonist TAK-994 was discontinued in Phase 2 (2023) due to hepatotoxicity — elevated liver enzymes in a significant proportion of participants. TAK-861 was redesigned with a different chemical scaffold to eliminate the hepatotoxic liability. The Phase 2 publication in NEJM (March 2025) and the two Phase 3 trials (September 2025) confirm both efficacy and acceptable safety; oveporexton as a selective OX2R agonist significantly improved wakefulness, EDS, and cataplexy symptoms in NT1 without observed hepatotoxicity.[7][8]
ALKS 2680 (Alkermes): Competing OX2R agonist in Phase 2; published proof-of-concept data in 2025 showing wake-promoting effects in narcolepsy and idiopathic hypersomnia. ORX142, ORX750 (Centessa Pharmaceuticals): Selective OX2R agonists in early clinical development for NT1, NT2, and idiopathic hypersomnia. TAK-360 (Takeda): Follow-on OX2R agonist being developed for narcolepsy type 2 and idiopathic hypersomnia.
Beyond Narcolepsy and Insomnia: The Broader Orexin System
Feeding behaviour and metabolism: Orexin integrates metabolic signals (glucose, leptin, ghrelin) and was initially named for its appetite-stimulating effects. NT1 patients paradoxically become obese despite reduced caloric intake — suggesting orexin loss disrupts metabolic regulation and energy expenditure beyond sleep. Reward and addiction: OX1R in the VTA mediates orexin’s role in reward processing; OX1R antagonists reduce cue-induced reinstatement of drug-seeking in animal models (alcohol, cocaine, opioids, nicotine). Cardiovascular and respiratory regulation: Orexin increases heart rate and blood pressure; may be implicated in the arousal response that terminates apnoeic episodes in sleep apnoea. Stress and anxiety: OX1R in the extended amygdala mediates anxiogenic effects; OX1R antagonism has anxiolytic effects in animal models. Depression: Seltorexant, a selective OX2R antagonist, is in Phase 3 trials for major depressive disorder with insomnia — a mechanistically distinct application from insomnia DORAs, based on the hypothesis that improved sleep quality improves depression outcomes.
Orexin B as a Research Reagent
Synthetic orexin B is commercially available for in vitro OX2R pharmacology characterisation, electrophysiology studies (brain slice perfusion), drug screening assays (displacement from OX2R binding), and behavioural neuroscience (ICV injection in rodents to characterise arousal effects). The central challenge with exogenous orexin B as a therapeutic agent is the blood-brain barrier (BBB): as a 28-amino acid hydrophilic peptide, orexin B cannot cross the BBB by passive diffusion. This is why all therapeutic development has focused on small-molecule OX2R agonists rather than the peptide itself. Intranasal delivery of orexin A (using olfactory pathway delivery to bypass the BBB) has been explored in research settings with some effect in narcoleptic mice, but remains preclinical.
Clinical Measurement: CSF Orexin-A as NT1 Biomarker
The diagnostic biomarker for NT1 is CSF orexin-A (hypocretin-1) measured by radioimmunoassay from lumbar puncture samples. Threshold: <110 pg/mL (or <1/3 of mean normal values). NT1 with cataplexy: sensitivity ~87%, specificity ~99%. NT2 (without cataplexy): typically normal orexin levels. Idiopathic hypersomnia: typically normal orexin levels. Orexin-A is measured (not orexin-B) because its CSF concentration is higher (~200–400 pg/mL in healthy adults) and its immunoassay measurement is better standardised — both peptides are produced by the same neurons, so either would in principle provide the same diagnostic information.
Safety Profile of the Orexin System
DORA antagonists: Most important real-world signals are next-day cognitive impairment at higher doses, occasional sleep paralysis, and rare complex sleep behaviours. Unlike benzodiazepines and barbiturates, DORAs do not cause respiratory depression. OX2R agonists: Hepatotoxicity emerged with TAK-994 (compound-specific, not a class effect). TAK-861 (oveporexton) showed no hepatotoxicity signal across Phase 2 and Phase 3 trials; ongoing liver enzyme monitoring will be required in any approval label. Other noted effects: nausea, headache, dizziness — mild and transient.
Key Takeaways
- Orexin B (hypocretin-2) is the endogenous OX2R-preferring neuropeptide of the orexin system, produced by ~70,000 lateral hypothalamic neurons. Its preferential affinity for OX2R (vs. orexin A’s dual OX1R/OX2R activity) makes it specifically relevant to wakefulness maintenance and REM suppression.[2]
- Loss of orexin-producing neurons causes narcolepsy type 1 — one of the most molecularly complete explanations of any neurological disorder. The discovery of orexins in 1998 and the narcolepsy-orexin link within two years is a landmark in modern neuroscience.[3][5]
- OX2R is the critical receptor. OX2R in the TMN maintains wakefulness via histamine; OX2R in the vlPAG/LPT suppresses cataplexy by maintaining brainstem motor tone. This 2025 circuit dissection explains how OX2R agonists address the full NT1 symptom spectrum.[10]
- ✅ Two approved drug classes demonstrate the system’s reversible pharmacology. DORA antagonists for insomnia prove that blocking orexin promotes sleep. OX2R agonist development (oveporexton/TAK-861) for narcolepsy proves that restoring orexin signalling restores wakefulness. The FDA has accepted oveporexton’s NDA with Priority Review — approval is imminent.[9]
- Exogenous orexin B peptide itself is not a clinical therapeutic due to BBB impermeability. The therapeutic strategy is small-molecule OX2R agonists that cross the BBB — which is the reason a decade of drug discovery was required after the orexin-narcolepsy link was established.
References
Discovery
- de Lecea L, Kilduff TS, Peyron C, et al. The hypocretins: hypothalamus-specific peptides with neuroexcitatory activity. PNAS. 1998;95(1):322–327.
- Sakurai T, Amemiya A, Ishii M, et al. Orexins and orexin receptors: a family of hypothalamic neuropeptides and G protein-coupled receptors that regulate feeding behavior. Cell. 1998;92(4):573–585.
Narcolepsy-Orexin Link
- Chemelli RM, Willie JT, Sinton CM, et al. Narcolepsy in orexin knockout mice: molecular genetics of sleep regulation. Cell. 1999;98(4):437–451.
- Lin L, Faraco J, Li R, et al. The sleep disorder canine narcolepsy is caused by a mutation in the hypocretin (orexin) receptor 2 gene. Cell. 1999;98(3):365–376.
- Nishino S, Ripley B, Overeem S, Lammers GJ, Mignot E. Hypocretin (orexin) deficiency in human narcolepsy. Lancet. 2000;355(9197):39–40.
Clinical Drug Development
- Oveporexton (TAK-861) Phase 3 results: FirstLight and RadiantLight studies. Presented at World Sleep 2025, Singapore, September 8, 2025. Takeda press release.
- TAK-861 Phase 2 results (Dauvilliers et al.). New England Journal of Medicine. March 2025.
- Mitsukawa K, Terada M, Yamada R, et al. TAK-861, a potent, orally available orexin receptor 2-selective agonist, produces wakefulness in monkeys and improves narcolepsy-like phenotypes in mouse models. Scientific Reports. 2024;14(1):20838. PMID 39242684
- FDA accepts NDA for oveporexton with Priority Review. NeurologyLive. March 2026.
Neuroanatomy and Mechanism
- OX2R-selective agonist improves narcolepsy via distinct brain regions. Current Biology. April 14, 2025. doi:10.1016/j.cub.2025.03.040
- Focal restoration of OX2R in the posterior hypothalamus rescues sleepiness in narcoleptic mice. PNAS. 2011. PMC3060231
Structural Biology
- Structures of active-state orexin receptor 2 rationalize peptide and small-molecule agonist recognition and receptor activation. Nature Communications. 2021. doi:10.1038/s41467-021-21087-6
Reviews
- Orexin deficiency in narcolepsy: molecular mechanisms, clinical phenotypes, and emerging therapeutic frontiers. Brain and Behavior. 2025. PMC12515106
- Hypocretin: a promising target for the regulation of homeostasis. Frontiers in Neuroscience. 2025. PMC12415059
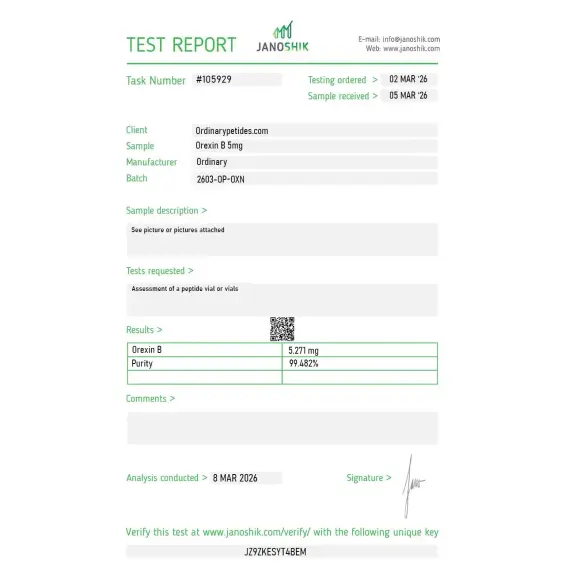
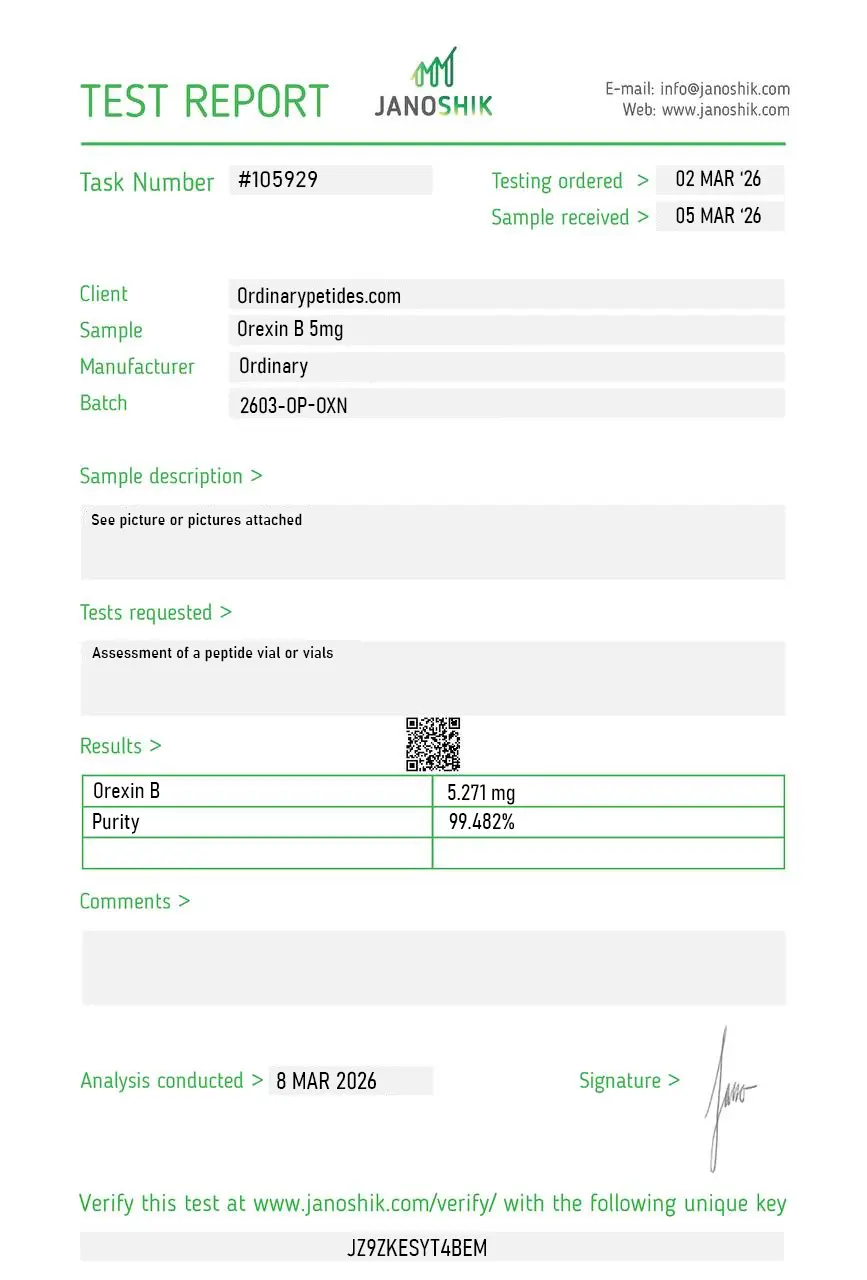
Certificate of Analysis
An independent test report is available for Orexin-B 5mg. This report provides batch-level documentation and analytical verification information for research reference.
Based on 1 reviews
5.0
The 28-residue sequence dissolved cleanly without surprises in our standard buffer. Held activity in our OX2R reporter line across the working window.
Orexin B (also known as Hypocretin-2) is a naturally occurring neuropeptide consisting of 28 amino acids, produced exclusively by a small cluster of approximately 50,000 to 80,000 neurons in the lateral hypothalamus and perifornical area of the brain. It is derived alongside Orexin A from a common precursor protein called prepro-orexin. Both orexins were discovered simultaneously in 1998 by two independent research groups — one named them orexins from the Greek word for appetite, the other named them hypocretins for their hypothalamic origin. The key structural difference between the two is that Orexin B is a linear peptide while Orexin A contains two disulfide bonds, and this difference drives their receptor selectivity.
Orexin B binds primarily and with high affinity to the OX2 receptor (OX2R), with significantly lower potency at OX1R — approximately five times less potent than Orexin A at OX1R. OX2R activation triggers G-protein signaling cascades that increase intracellular calcium, depolarize neurons, inactivate inhibitory potassium channels, and increase NMDA receptor expression on cell surfaces — producing long-lasting increases in neuronal excitability. Through these mechanisms Orexin B promotes arousal and wakefulness, modulates energy expenditure, and regulates reward and feeding circuits. Its selective action at OX2R makes it particularly important for wake-maintenance and has guided the development of OX2R-selective drugs for narcoleps
The orexin system — including Orexin B — is described as a master regulator of multiple vital functions. Its key roles include stabilizing wakefulness and suppressing transitions into sleep, regulating energy homeostasis and metabolism through brown adipose tissue activity and sympathetic nervous system signaling, modulating appetite and feeding behavior, regulating mood and emotional states, controlling the stress response and HPA axis activity, and influencing reward circuits and addiction-related behaviors. Orexin B specifically shows a neuroprotective role for dopamine neurons in the midbrain, with research demonstrating it protects against dopamine neuron degeneration — a finding with implications for Parkinson's disease.
Orexin B and the broader orexin system are being studied for narcolepsy and excessive daytime sleepiness — where orexin deficiency is the direct cause — cognitive impairment and age-related dementia, Parkinson's disease given the loss of orexin neurons observed in PD patients, depression and anxiety disorders, obesity and metabolic dysfunction, and addiction medicine. Intranasal delivery of orexin peptides is being investigated as a route to bypass the blood-brain barrier for therapeutic use in cognitive decline and narcolepsy, though CNS penetration remains variable and a key challenge.
Rather than administering Orexin B directly, the most clinically advanced therapeutic approach is blocking the orexin system to treat insomnia. Suvorexant (Belsomra) — a dual OX1R/OX2R antagonist — is FDA-approved for insomnia treatment. Lemborexant is another approved dual orexin receptor antagonist. On the opposite end, OX2R agonists such as danavorexton (TAK-925) are in clinical trials for narcolepsy, demonstrating that selectively activating OX2R — the primary target of Orexin B — increases wakefulness in narcoleptic patients.
Direct exogenous administration of Orexin B as a research peptide carries risks of cardiovascular effects including elevated blood pressure and heart rate through peripheral receptor activation, excessive arousal or anxiety at supraphysiological doses, and difficulty achieving consistent CNS penetration via systemic or intranasal routes. Systemic delivery is complicated by peripheral degradation and poor blood-brain barrier crossing. OX2R agonist drugs in clinical trials have generally shown acceptable tolerability, with headache and nausea among the most commonly reported side effects.
People with cardiovascular conditions including hypertension, arrhythmias, or coronary artery disease should avoid unsupervised use given orexins' sympathoexcitatory cardiovascular effects. Those with anxiety disorders or PTSD should exercise caution as orexin system overactivation has been linked to anxiety-like states. Pregnant or breastfeeding women should avoid it. As Orexin B itself has no approved clinical formulation and exists only as a research peptide, any use must remain strictly within qualified research settings under institutional oversight.





