

5-Amino 1MQ
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
5-Amino-1MQ: A Small-Molecule NNMT Inhibitor at the Crossroads of NAD+ Biology, Adipose Metabolism, and Aging Research
5-Amino-1MQ, also known as 5-Amino-1-methylquinolinium iodide, is a small molecule best known in the field of metabolic research, where it has been studied as a selective inhibitor of nicotinamide N-methyltransferase (NNMT) and linked to the biology of NAD+ regulation. In the research context, the main interest in this compound grew out of studies reporting preserved NAD+ pools, increased energy expenditure, and reduced fat mass in preclinical models. That sounds dramatic — and that is precisely why it attracts so much attention.
Published reports have also discussed its relationship with mitochondrial function, SIRT1 signaling, and adipose tissue energy balance, while preclinical data have connected it to a broader metabolic and regenerative framework, including effects on muscle stem cell biology. Still, a sober filter is essential here: a compelling enzymatic story is not yet a ready-made fat-loss solution in a vial. If only biology were that cooperative.
What makes 5-Amino-1MQ genuinely interesting is that it sits at the crossroads of longevity hypotheses, methyl-donor metabolism, and the broader tradition of NAD-centric pharmacology. For readers who care not just about bold promises but about the actual scientific grounds for interest, this is exactly the kind of compound worth examining carefully — and without illusions.
Tesofensine: A Scientific Review of the Triple Monoamine Reuptake Inhibitor for Obesity
Based on peer-reviewed literature and regulatory filings — see References. Last updated: May 2026.
The Short Version
Tesofensine has one of the more interesting backstories in modern obesity pharmacology. It was never meant to be a weight loss drug. Originally developed by the Danish company NeuroSearch under the code name NS2330, it was pushed through Phase 2 trials for Alzheimer's and Parkinson's disease in the early 2000s. It didn't work well for either. But trial participants — many of whom were overweight or obese — kept losing weight. Quite a lot of weight, in fact. The "adverse event" became the indication.
Fifteen years and one Phase 3 trial later, tesofensine produced what is arguably the strongest weight loss data of any small-molecule appetite suppressant ever tested in humans: roughly 10–11% body weight reduction at 0.5 mg/day over 24 weeks, with the higher 1.0 mg dose pushing toward 12%.[1] For comparison, the older generation of obesity drugs — sibutramine, rimonabant, orlistat — topped out at 5–6%. This is small-molecule pharmacology in the same general efficacy range as the early GLP-1 analogs, taken as a pill, without titration, at a fraction of the manufacturing cost.
That's the story you hear in the wellness/biohacker space. Here's what usually gets left out.
The reason tesofensine isn't currently sold in the US or Europe isn't because nobody tried. NeuroSearch and later Saniona pursued Western approval for over a decade. The FDA endorsed the Phase 3 program in 2009. Then, somewhere between the Phase 2 data and the regulatory finish line, the development arc in the US and EU effectively stalled. The drug ended up being commercialized through a Mexico-based partner (Medix), which spent five years and an approximately 20,000-page dossier negotiating with COFEPRIS before getting a favorable opinion in February 2023 and final approval in the 2024–2025 window.[8]
There are two reasons the Western development slowed. The first is competitive: GLP-1 agonists (semaglutide, then tirzepatide) showed up with similar or better efficacy and an entirely different — and, importantly, well-understood — safety profile. The second is intrinsic to the drug: tesofensine raises heart rate. Reliably. Dose-dependently. By roughly 7–8 bpm at the 0.5 mg therapeutic dose, with sympathetic-system mechanisms that look uncomfortably similar to sibutramine — a structurally related drug that was withdrawn from Western markets in 2010 over cardiovascular concerns.[3][4]
| At a glance | |
|---|---|
| Code name | NS2330 |
| Brand names | Tesomet (with metoprolol, for rare indications); commercial obesity product launched in Mexico via Medix |
| Chemical class | Phenyltropane; small molecule |
| Mechanism | Triple monoamine reuptake inhibitor (DAT, NET, SERT) |
| IC50 (in vitro) | DAT ≈ 8.0 nM, NET ≈ 3.2 nM, SERT ≈ 11.0 nM |
| Half-life | ~9 days (220 h) parent; ~16 days (374 h) for active metabolite NS2360 |
| Metabolism | Primarily CYP3A4 (to NS2360) |
| Standard therapeutic dose | 0.25 mg or 0.5 mg once daily, oral |
| Originator | NeuroSearch (Denmark) → Saniona (2014) |
| Mexico/Argentina commercialization | Medix |
| FDA status | ❌ Not approved |
| EMA status | ❌ Not approved |
| COFEPRIS (Mexico) | ✅ Favorable opinion Feb 2023; commercial pathway 2024–2025 |
| Clinical safety database | ~1,600 patients across 20+ trials |
The Backstory: An Anti-Parkinson Drug That Made People Lose Weight
NeuroSearch designed tesofensine in the 1990s as a CNS drug. The pharmacological logic was straightforward: many neurodegenerative diseases involve depleted dopamine and norepinephrine signaling. A compound that prevents reuptake of those neurotransmitters should boost the residual signal. The same logic underlies modern Parkinson's adjuncts.
The Parkinson's and Alzheimer's trials in the early-to-mid 2000s were a disappointment in terms of the primary indication — symptomatic improvement was modest. But a meta-analysis of the obesity sub-populations across those neurological trials showed something striking: at doses of 0.125 to 1.0 mg daily, about 32% of obese subjects on the high dose achieved ≥5% weight loss after just 14 weeks.[2] In obesity research, that's a result you stop and look at twice.
So NeuroSearch repositioned. The result was TIPO-1 (Tesofensine In Patients with Obesity, trial 1) — the Phase 2 study that made the drug famous.
Mechanism of Action
The triple monoamine story
Tesofensine blocks the presynaptic reuptake of three neurotransmitters at once: dopamine, norepinephrine, and serotonin. Most psychiatric drugs target one (SSRIs) or two (SNRIs) of these. Tesofensine hits all three.
The pharmacological consequence in the brain is sustained elevation of all three monoamines in the synaptic cleft. Each one feeds into appetite regulation through different circuits:
- Norepinephrine → activation of sympathetic tone, increased energy expenditure, decreased food-seeking drive
- Dopamine → reduced reward value of food, decreased craving, increased alertness
- Serotonin → enhanced satiety, particularly post-meal fullness
This is roughly the same pharmacological space sibutramine occupied — except sibutramine was primarily a serotonin/norepinephrine reuptake inhibitor with relatively weak dopaminergic action. Tesofensine adds substantial dopamine reuptake inhibition to the mix, and that dopaminergic component is widely thought to be what gives the drug its unusually strong appetite-suppressing effect.
What the Mexican neuroscience group actually showed
The Gutierrez lab at CINVESTAV in Mexico published a striking 2024 paper in PLOS ONE digging into the mechanism at single-neuron resolution.[5] Using optogenetics and chemogenetics in transgenic mice, the group showed that tesofensine specifically inhibits a subset of GABAergic neurons in the lateral hypothalamus — a brain region long known as a master regulator of feeding behavior. When the researchers chemogenetically silenced those same neurons, the food-suppressing effect of tesofensine was amplified.
A few other observations from that paper are worth flagging:
- Tesofensine produced greater weight loss in obese than in lean rats — suggesting the drug doesn't simply suppress appetite globally, but selectively rebalances overactive feeding circuits.
- Unlike phentermine (a classical dopaminergic appetite suppressant), tesofensine at therapeutic doses caused little to no stereotypic behavior — the head-weaving repetitive movements that signal overstimulation of dopaminergic reward circuits.
- Tesofensine blocked the weight rebound that normally follows discontinuation of 5-HTP (a serotonin precursor) — a finding with potential clinical implications for the most frustrating problem in obesity medicine: regain.
This is real mechanistic work, done outside the originator company, and it adds substantial credibility to the drug's biological story. In the broader metabolic research landscape, tesofensine occupies a distinctive niche: a centrally-acting appetite suppressant in a field now dominated by gut-hormone analogs.
| Proposed mechanism | Evidence | Strength |
|---|---|---|
| Triple monoamine reuptake inhibition (DAT/NET/SERT) | In vitro binding and reuptake assays | ✅ Well-established |
| Appetite suppression via dopamine/norepinephrine | Animal + human clinical | ✅ Strong |
| Selective silencing of LH GABAergic neurons | Optogenetics in mice (Perez/Gutierrez 2024) | ✅ Independently demonstrated |
| Increased resting energy expenditure | Indirect calorimetry studies | ⚠️ Modest, not the primary mechanism |
| Decreased food reward / craving | Behavioral studies + clinical reports | ✅ Consistent with dopaminergic action |
| Rebound prevention | Animal data (5-HTP combination) | ⚠️ Preclinical only |
Clinical Evidence: TIPO-1 and the Phase 3 Viking Study
TIPO-1 (Astrup et al., Lancet, 2008)
This is the foundational human study and remains, fifteen years later, one of the better-designed Phase 2 obesity trials in the literature.
Design: Phase 2, randomized, double-blind, placebo-controlled. Five Danish obesity centers. 203 obese patients (BMI 30–40), 2-week run-in on energy-restricted diet, then randomization to placebo, 0.25 mg, 0.5 mg, or 1.0 mg tesofensine once daily for 24 weeks.[1]
Results:
| Group | Mean weight loss at 24 weeks |
|---|---|
| Placebo | ~2% |
| Tesofensine 0.25 mg | ~5% |
| Tesofensine 0.5 mg | ~9% (some sources report up to 10.6%) |
| Tesofensine 1.0 mg | ~11% |
These numbers are clean dose-response. The 0.5 mg dose — which became the standard for further development — produced approximately twice the weight loss of any then-approved obesity drug at the time. The weight loss was driven primarily by reduced food intake, with a smaller but measurable contribution from increased energy expenditure.
The paper also reported improvements in body composition (preferential loss of fat mass), waist circumference, quality of life scores, and glycemic markers. The drug worked as advertised.
Phase 3 Viking study (Medix, Mexico, 2018)
Saniona's Mexican partner Medix ran the registration Phase 3 trial — 372 obese patients across two Mexican sites — testing 0.25 mg and 0.5 mg doses against placebo. Top-line results were announced in December 2018: both doses produced statistically and clinically significant weight loss versus placebo, replicating the Phase 2 efficacy in a larger population.[6] Detailed peer-reviewed publication of the Phase 3 results was incremental and substantially less prominent in the Western literature than TIPO-1.
The Phase 3 program, combined with the prior NeuroSearch trials, brought the cumulative clinical safety database to approximately 1,600 patients on therapeutic doses for up to a year.
What about the GLP-1 comparison?
This is unavoidable. Anyone evaluating tesofensine in 2026 is implicitly comparing it to semaglutide and tirzepatide. Some honest comparisons:
| Parameter | Tesofensine 0.5 mg | Semaglutide 2.4 mg (Wegovy) | Tirzepatide 15 mg (Zepbound) |
|---|---|---|---|
| Mean weight loss, 24 weeks | ~10% | ~10–12% | ~15% |
| Route | Oral tablet | Weekly injection | Weekly injection |
| Titration needed | No | Yes (16-week ramp) | Yes |
| Cost per month (typical, 2026) | Low (small molecule) | High | High |
| Heart rate effect | ↑ 7–8 bpm | ↑ 2–4 bpm | ↑ 3–5 bpm |
| Psychiatric AE signal | Documented | Minimal | Minimal |
| GI side effects | Mild (dry mouth, constipation) | Substantial (nausea, vomiting) | Substantial |
| Mechanism understood at receptor level | ✅ Well | ✅ Well | ✅ Well |
The honest read: tesofensine is in the same efficacy ballpark as semaglutide. It is cheaper, oral, doesn't require titration, and has fewer GI side effects. It has more cardiovascular and psychiatric concerns. Which matters more depends entirely on the patient. For other weight-management compounds that work through entirely different mechanisms — appetite/satiety via amylin, for instance — see cagrilintide.
Pharmacokinetics: The Long Half-Life Problem
Tesofensine has an unusually long half-life: approximately 9 days for the parent compound, and 16 days for the active metabolite NS2360 (which contributes only modestly — about 6% of total activity, but at 31–34% of parent exposure at steady state).[7]
What this means practically:
- Steady state takes weeks. Don't expect to feel the full effect (or the full side effect profile) until 4–6 weeks in.
- Dose adjustment is slow. If you raise the dose and have a problem, the drug doesn't wash out in a few days.
- Drug interactions persist. Strong CYP3A4 inhibitors or inducers can shift plasma levels in ways that take weeks to normalize.
- Discontinuation is gradual. Side effects typically resolve over 5–10 days, but full elimination takes substantially longer.
The renal contribution to clearance is small (15–20% in humans), so this is fundamentally a hepatic CYP3A4 drug. That has real implications for drug interactions, which are touched on below.
Safety: The Real Story
Here's where this drug requires the most careful discussion. The efficacy is exceptional. The safety profile is not.
Cardiovascular signal
This is the dominant concern. Across the clinical program, tesofensine consistently produced:
- Resting heart rate increase of ~7–8 bpm at 0.5 mg/day. Dose-dependent — higher at 1.0 mg, lower at 0.25 mg.[3][4]
- Modest blood pressure increases, particularly systolic, at the 0.5 mg and especially 1.0 mg doses. At 0.25 mg, BP changes are typically not clinically significant.
- The mechanism is well-understood: norepinephrine reuptake inhibition increases sympathetic tone and peripheral vascular resistance.
The animal pharmacology supports this story directly. In rats, co-administration of metoprolol (a β1-blocker) fully blocks tesofensine's cardiovascular effects while preserving its appetite suppression — suggesting the two effects, although both downstream of sympathetic activation, can be pharmacologically separated.[10] This is exactly the logic behind Tesomet — the fixed-dose combination of tesofensine plus metoprolol that Saniona has developed for rare eating disorder indications. For broader context on compounds studied in cardiac-relevant settings, see the cardiovascular research category.
Psychiatric signal
This is the second concern, and it's underdiscussed. The clinical trial data document psychiatric adverse events at meaningfully higher rates than placebo: mood changes, anxiety, sleep disturbance, irritability. Estimates from the published literature suggest 12–18% of participants experienced some psychiatric AE, with 2–3% having events serious enough to warrant intervention or discontinuation.
The mechanism makes sense: chronically elevated dopamine, norepinephrine, and serotonin in the brain is, pharmacologically, the same general signature as a moderate-dose stimulant or antidepressant. Anyone with a personal or family history of bipolar disorder, anxiety, major depression, or psychosis is in a meaningfully different risk category for this drug.
Common adverse events
The everyday AE profile is reasonable for a CNS-active appetite suppressant:
- Dry mouth (most common)
- Insomnia / sleep disruption
- Nausea (less than GLP-1s)
- Constipation
- Headache
- Mild anxiety / agitation
Most of these are dose-dependent and improve with the 0.25 mg dose. Morning dosing helps with insomnia given the long half-life.
What's not well-characterized
- Long-term outcomes beyond 1 year. The bulk of the safety data covers up to 12 months of treatment. Obesity is a chronic condition; people taking obesity medications often want to take them for many years. The chronic-use safety profile of tesofensine is incompletely characterized.
- Cardiovascular outcomes (MACE). No dedicated long-term cardiovascular outcomes trial has been conducted. Whether the bpm/BP signal translates to actual cardiovascular events at the population level — unknown.
- Drug-drug interactions. Given CYP3A4 metabolism, interactions with common medications (some antifungals, some macrolides, certain antiretrovirals, grapefruit juice in high quantities) are clinically relevant but not exhaustively mapped.
- Pregnancy. Contraindicated. No human pregnancy data.
| Safety area | Status |
|---|---|
| Resting heart rate increase | ⚠️ Documented, ~7–8 bpm at 0.5 mg, dose-dependent |
| Blood pressure elevation | ⚠️ Modest at therapeutic doses, more pronounced at 1.0 mg |
| Sustained hypertension requiring intervention | ⚠️ ~8–12% of users in trial settings |
| Psychiatric adverse events | ⚠️ 12–18% incidence (anxiety, mood, sleep) |
| Serious psychiatric AE | ~2–3% |
| Long-term (>1 year) safety | ❌ Incompletely characterized |
| Cardiovascular outcomes trial | ❌ Not conducted |
| Drug-drug interactions | ⚠️ CYP3A4-mediated; many relevant interactions |
| MAOI co-administration | ❌ Contraindicated |
| Pregnancy / breastfeeding | ❌ Contraindicated |
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) | ❌ Not approved. Phase 3 program endorsed by FDA in 2009 but never advanced to filing by NeuroSearch/Saniona. |
| EMA (Europe) | ❌ Not approved |
| COFEPRIS (Mexico) | ✅ Favorable regulatory opinion February 2023; resubmission with ~20,000-page dossier 2024; final approval pathway 2024–2025 via Medix |
| Argentina | Commercial rights held by Medix |
| WADA | Not specifically named on the 2026 Prohibited List, but as a stimulant-like CNS-active substance with documented sympathomimetic effects, would likely fall under banned classes for in-competition testing. Tested athletes should verify with their federation. |
The Mexico/Argentina commercialization is a real regulatory approval, not a grey-market arrangement. COFEPRIS reviewed the full clinical dossier and approved the drug after a substantial back-and-forth. The product is sold by prescription through Medix in Mexico.
What it is not is a substitute for FDA or EMA approval. The standards for those agencies are different — particularly regarding long-term cardiovascular outcomes — and the absence of approval in those jurisdictions reflects unresolved questions, not just commercial inertia.
Tesomet: The Combination Product
Worth mentioning separately. Tesomet is a fixed-dose combination of tesofensine (typically 0.25 mg or 0.5 mg) plus metoprolol (a β1-blocker). The logic is direct: metoprolol pharmacologically blocks the tachycardia caused by tesofensine without interfering with the appetite suppression.
Tesomet has been investigated specifically for rare obesity indications where the unmet need is most acute and the risk-benefit calculus shifts:
- Prader-Willi syndrome (PWS) — a genetic disorder causing severe hyperphagia
- Hypothalamic obesity — typically following surgical removal of craniopharyngioma or related pituitary/hypothalamic damage
Both are conditions where existing pharmacotherapy is poor, surgical options limited, and the consequences of untreated hyperphagia severe. Tesomet has shown promising Phase 2 data in PWS and hypothalamic obesity (NCT03149445, NCT03845075). As of 2026, Saniona has stated the program is ready for Phase 2b. No regulatory approval for these indications exists yet anywhere.
Common Misconceptions
"It's a peptide."
It isn't. Tesofensine is a small organic molecule of the phenyltropane class — chemically related to cocaine and certain tropane-derivative dopamine reuptake inhibitors, though pharmacologically very different in profile (slow onset, long half-life, no abuse potential of any significance in clinical trials). The "peptide therapy" framing on some wellness sites is straightforwardly wrong.
"It's available because it's safe enough for over-the-counter use in Mexico."
It's available in Mexico because it's an approved prescription drug, with the same monitoring requirements you'd expect — baseline cardiovascular evaluation, BP and heart rate monitoring during treatment, psychiatric history screening. It is not an OTC product.
"FDA didn't approve it because of politics / GLP-1 lobbying."
This view appears occasionally online and isn't supported by the actual regulatory history. The FDA endorsed the Phase 3 program in 2009. NeuroSearch encountered financial difficulties and the program transitioned to Saniona, which prioritized the Mexico/Argentina pathway through Medix. Western regulatory progress slowed because (a) the sponsor's strategic priorities shifted and (b) the cardiovascular safety data, while not disqualifying, did not provide the margin of comfort that the post-sibutramine FDA wanted to see without a dedicated CV outcomes trial. The economics of running such a trial against an incumbent class of approved GLP-1 drugs are unfavorable.
"It works on the same mechanism as the GLP-1 drugs."
It does not. GLP-1 receptor agonists work primarily through gut hormone receptors — slowing gastric emptying, modulating insulin secretion, and acting on hindbrain satiety circuits. Tesofensine is a central monoamine modulator. The clinical phenomenology (appetite suppression, weight loss) overlaps; the mechanism and side effect profile do not.
Frequently Asked Questions
Why isn't there more recent data?
The molecule has been around for over 25 years and its mechanism is well-characterized. The recent literature focuses on niche indications (PWS, hypothalamic obesity, refinement of the mechanism in animals) rather than new pivotal trials, because the obesity Phase 3 data was generated years ago and the commercialization decision moved to Mexico. The Perez/Gutierrez 2024 paper in PLOS ONE is the most recent significant mechanism paper.
Could it come to the US?
Saniona has indicated that Mexican approval may open opportunities elsewhere, but no concrete US filing is publicly announced as of May 2026. Any US pathway would likely require either a partnership with a larger pharma company or fresh long-term cardiovascular safety data.
Is the weight loss durable after stopping?
Like virtually all obesity medications, weight regain is common after discontinuation. The TIPO-2 extension data showed some weight loss persisted but with substantial individual variation. The animal data on rebound prevention with 5-HTP combination is preclinical and not yet translated to humans.
How does it interact with caffeine, stimulants, or ADHD medications?
Likely additive on cardiovascular and CNS stimulation. This is not formally well-characterized in the literature, but pharmacologically expected. Worth flagging to a prescribing physician.
Key Takeaways
- Tesofensine is one of the most efficacious oral small-molecule appetite suppressants ever developed in humans — ~10% body weight loss at 0.5 mg/day over 24 weeks, replicated across Phase 2 and Phase 3 trials.[1][6]
- The mechanism is well-understood (triple monoamine reuptake inhibition) and supported by elegant single-neuron work showing selective inhibition of GABAergic neurons in the lateral hypothalamus.[5]
- ⚠️ The cardiovascular signal is real. A reliable ~7–8 bpm increase in resting heart rate at therapeutic doses, with mechanism-based concerns that parallel the now-withdrawn sibutramine. No dedicated cardiovascular outcomes trial has been done.
- ⚠️ The psychiatric signal is real and underdiscussed. 12–18% of patients experience some psychiatric AE; 2–3% experience serious events. Personal or family history of mood, anxiety, or psychotic disorders shifts the risk calculus substantially.
- The drug is approved in Mexico (COFEPRIS, via Medix), with a real regulatory dossier and prescription distribution. It is not approved by the FDA or EMA, and the absence of those approvals reflects substantive unresolved questions, not just commercial inertia.
- The 9-day parent half-life and 16-day metabolite half-life mean steady state takes weeks and washout is slow. This is not a drug you titrate quickly or stop abruptly without consequence.
- ⚠️ For anyone with cardiovascular disease, hypertension, arrhythmia, active mood disorder, or who takes MAO inhibitors, this drug is either contraindicated or requires substantial caution. These are not academic concerns — they're the central reason the drug requires medical supervision.
- The comparison to GLP-1 drugs is unavoidable but contextual: tesofensine is cheaper, oral, and has fewer GI side effects, at the cost of a more concerning cardiovascular and psychiatric profile. For the right patient — without cardiovascular or psychiatric risk factors — the trade-off may be reasonable. For the wrong patient, it is not.
Related Compounds
For other compounds investigated for weight management and metabolic regulation, see the Metabolic Research category. Two notable peptide alternatives in this space are the amylin analog cagrilintide and the lipolytic fragment AOD9604.
References
Foundational clinical trial
- Astrup A, Madsbad S, Breum L, Jensen TJ, Kroustrup JP, Larsen TM. Effect of tesofensine on bodyweight loss, body composition, and quality of life in obese patients: a randomised, double-blind, placebo-controlled trial. Lancet. 2008;372(9653):1906–1913. doi: 10.1016/S0140-6736(08)61525-1
- Astrup A, et al. (related meta-analysis from neurological trial sub-populations, cited in Astrup 2008a).
Mechanism
- Sjödin A, Gasteyger C, Nielsen ALH, et al. The effect of the triple monoamine reuptake inhibitor tesofensine on energy metabolism and appetite in overweight and moderately obese men. Int J Obes. 2010.
- Doggrell SA. Tesofensine — a novel potent weight loss medicine. Expert Opin Investig Drugs. 2009;18(7):1043–1046. PMID: 19548858
- Perez CI, Luis-Islas J, Lopez A, et al. Tesofensine, a novel antiobesity drug, silences GABAergic hypothalamic neurons. PLOS ONE. 2024;19(4):e0300544.
Phase 3 and registration
- Saniona/Medix press release, December 2018: Phase 3 Viking study top-line results.
- Tesofensine pharmacokinetic profile and metabolism: half-life ~9 days; CYP3A4 metabolism to NS2360 (M1).
Regulatory and program history
- Saniona Q4 2024 / Q1 2025 corporate filings on COFEPRIS approval pathway.
- Bello NT, Zahner MR. Tesofensine, a monoamine reuptake inhibitor for the treatment of obesity. Curr Opin Investig Drugs. 2009;10(10):1105–1116. PMID: 19777399
Cardiovascular mechanism
- Axel AM, Mikkelsen JD, Hansen HH. Anti-hypertensive treatment preserves appetite suppression while preventing cardiovascular adverse effects of tesofensine in rats. Eur J Pharmacol. 2013. PMID: 23784901
Key investigators
- Arne Astrup, MD, DMSc — Professor of Nutrition, University of Copenhagen. Principal investigator of TIPO-1.
- Ranier Gutierrez, PhD — CINVESTAV, Mexico. Mechanism work on LH GABAergic neurons.
- Saniona AB / Medix S.A. — Sponsors of Phase 3 and registration program.
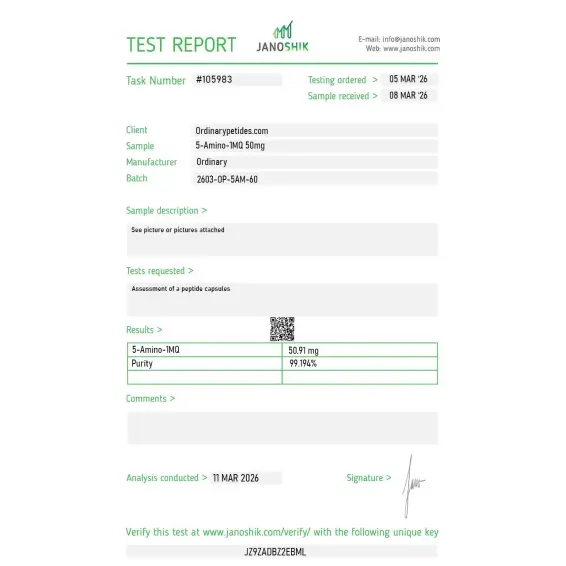
Certificate of Analysis
An independent test report is available for 5-Amino-1MQ 50mg. This report provides batch-level documentation and analytical verification information for research reference.

5-Amino-1MQ (5-amino-1-methylquinolinium) is a synthetic small-molecule compound classified as a selective inhibitor of the enzyme nicotinamide N-methyltransferase (NNMT). It was first characterized as an NNMT inhibitor by Neelakantan and colleagues in a landmark study published in the Journal of Medicinal Chemistry in 2017. With a molecular weight of 159.21 g/mol, it sits in the optimal range for cellular uptake studies. It is not technically a peptide, despite being grouped with research peptides by many suppliers — it is a methylquinolinium derivative and small molecule with oral bioavailability and strong membrane permeability.
5-Amino-1MQ targets NNMT — nicotinamide N-methyltransferase — a cytosolic enzyme expressed at high levels in white adipose tissue and liver, and also present in kidney, brain, lung, heart, and skeletal muscle. NNMT catalyzes the transfer of a methyl group from S-adenosylmethionine (SAM) to nicotinamide, producing 1-methylnicotinamide (1-MNA) and S-adenosyl-L-homocysteine (SAH). This reaction simultaneously depletes two critical cellular resources: NAD+ precursor availability (by diverting nicotinamide away from the NAD+ salvage pathway) and the cellular methyl pool (by consuming SAM). NNMT overexpression has been associated with obesity, insulin resistance, and metabolic dysfunction, making it a compelling therapeutic target.
5-Amino-1MQ acts as a competitive inhibitor of NNMT with an IC₅₀ of approximately 1 µM in biochemical assays. In living adipocytes, the EC₅₀ for reducing intracellular 1-MNA is 2.3 ± 1.1 µM. By blocking the enzyme, the compound prevents the methylation of nicotinamide into 1-MNA, which has two downstream consequences. First, more nicotinamide remains available for the NAMPT-driven NAD+ salvage pathway, raising intracellular NAD+ levels by 1.2 to 1.6-fold in cell culture studies. Second, SAM is preserved, restoring the SAM/SAH ratio and maintaining the thermodynamic drive for DNA and histone methylation reactions throughout the cell.
In diet-induced obese mouse models, NNMT inhibition with 5-Amino-1MQ reduced total body adiposity and plasma cholesterol without any change in food intake — a mechanistically important finding that distinguishes it from appetite-suppressing compounds. Preclinical experiments have indicated that NNMT inhibition can reduce lipid synthesis by over 50% and decrease adipocyte volume by approximately 40% in relevant models. In one study, treated animals showed roughly 7% reduction in body mass over 11 days. Researchers attribute this to increased energy expenditure within fat cells themselves — hypothesized to involve elevated NAD+ driving "futile cycling" and mitochondrial uncoupling-like processes rather than reduced caloric intake.
Elevated intracellular NAD+ resulting from NNMT inhibition activates NAD+-dependent enzymes, most notably the sirtuin family — particularly SIRT1. SIRT1 is a deacetylase that regulates downstream targets including PGC-1α (mitochondrial biogenesis), FOXO transcription factors (oxidative stress resistance), and AMPK (autophagy and cellular energy sensing). The mechanistic chain — NNMT inhibition → increased NAD+ → SIRT1 activation → PGC-1α upregulation → enhanced mitochondrial function and fatty acid oxidation — is consistent across multiple preclinical models and positions 5-Amino-1MQ within the broader NAD+ biology and longevity research landscape alongside NMN and nicotinamide riboside (NR), though through a distinct upstream mechanism.
By reducing NNMT's consumption of SAM, 5-Amino-1MQ preserves the cellular methyl pool. SAM is the universal methyl donor for DNA methylation, histone methylation, and polyamine synthesis. When NNMT is overactive — as occurs in obese adipose tissue and cancer-associated fibroblasts — the SAM/SAH ratio drops, globally reducing the thermodynamic drive for methylation reactions and remodeling chromatin toward pro-metabolic dysfunction or pro-tumor gene programs. A 2023 paper in Scientific Reports (Roberti, Tejedor et al.) demonstrated that NNMT directly regulates the glucocorticoid signaling pathway during early adipogenesis, connecting NNMT activity to hormonal pathways governing fat cell differentiation. This epigenetic dimension gives 5-Amino-1MQ potential relevance in aging and oncology research beyond metabolic disease.
A mechanistically distinct area of 5-Amino-1MQ research involves skeletal muscle regeneration. Muscle repair relies on satellite cells — resident stem cells that activate in response to damage. With aging, satellite cells become increasingly senescent and less capable of effective regeneration. Preclinical studies have found that NNMT inhibition can stimulate muscle satellite cell activity and improve regenerative capacity, particularly in aged muscle models. The proposed mechanism involves the NAD+-SIRT1-AMPK axis promoting autophagy, the NAD+-SIRT2 pathway reducing chronic low-grade inflammation, and restored NAD+ improving neuromuscular junction (NMJ) remodeling. These findings have drawn interest from researchers studying sarcopenia and age-related muscle atrophy.
This distinction is frequently misunderstood. NMN (nicotinamide mononucleotide) and NR (nicotinamide riboside) are NAD+ precursors — they supply additional substrate to directly increase cellular NAD+ levels through the salvage pathway. 5-Amino-1MQ is not a precursor at all — it works upstream by blocking the enzyme that wastes nicotinamide before it can enter the salvage pathway. The two approaches act on adjacent but distinct parts of the same metabolic axis. A 2023 review by Damgaard and Treebak in Science Advances summarized the human NR literature, highlighting progress on direct NAD+ supplementation. 5-Amino-1MQ research, by contrast, remains primarily in preclinical models, and the two strategies are not interchangeable in research design.
Beyond metabolic disease, NNMT has been identified as a significant factor in tumor microenvironments. In cancer-associated fibroblasts (CAFs), excessive NNMT activity depletes SAM and globally reduces histone methylation, remodeling chromatin toward gene programs that support tumor progression. This "methylation sink" phenotype is reversible with genetic or pharmacologic suppression of NNMT. 5-Amino-1MQ is being investigated in oncology research models as a tool to probe this mechanism — not as a therapeutic claim, but as a compound to dissect the causal relationship between stromal NNMT activity and tumor-supportive epigenetic states. This represents a research direction distinct from its metabolic applications.
As of 2026, 5-Amino-1MQ has not received approval from the FDA or any major regulatory authority. It is not on the FDA 503A bulk drug substances list. The entirety of published evidence derives from in vitro cell studies and preclinical animal models. Human clinical trial activity is described as emerging — Phase 1 trials have been registered in some geographies — but no completed, results-reported Phase 2 study exists in the published literature. A 2024 review in Frontiers in Pharmacology (Sun, Zhu et al.) identified NNMT as a novel therapeutic target for metabolic syndrome while noting the continued absence of human trial data. The compound is commercially available from research chemical suppliers as a Research Use Only (RUO) material, intended exclusively for qualified researchers conducting in vitro laboratory work.