
B7-33
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
B7-33: A Selective Relaxin Analogue With Smart Pharmacology and a Strong Preclinical Story
B7-33 is not just "another peptide," but a selective relaxin analogue designed as a more compact and thoughtfully engineered version of a complex natural molecule. In the research setting, it attracted attention because it acted through RXFP1 with a bias toward ERK1/2 signaling, and in preclinical models it showed antifibrotic, vasoprotective, and cardioprotective effects.
That kind of precise tuning is exactly what makes it especially interesting to people who judge peptides not by loud promises, but by the quality of the underlying idea. B7-33 has a strong scientific rationale, careful design, and a genuinely substantial preclinical story — which is already far more than just a pretty name in a catalog.
At the same time, its story is an honest one: the molecule remains a preclinical candidate, and that sober status arguably gives it even more credibility in the eyes of those who value real research significance. If you are interested in a peptide that stands out not because of hype, but because of smart pharmacology, B7-33 definitely deserves a closer look.
B7-33: A Scientific Review of the Single-Chain Relaxin Mimetic
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
B7-33 is a synthetic single-chain peptide derived from the B-chain of human relaxin-2 — a hormone best known for its roles in pregnancy physiology, but increasingly recognised for its potent anti-fibrotic and vasodilatory properties in multiple organ systems. The problem with using full relaxin-2 therapeutically is its complex structure: two chains held together by three disulfide bonds, making it difficult and expensive to produce, unstable in blood, and associated with some potentially undesirable side effects tied to one of its signalling pathways.
B7-33 was designed to solve that problem. Reported first in 2016 by a research group at the University of Melbourne and Monash University led by Mohammed Akhter Hossain,[1] it is the first known example of reducing a two-chain cyclic insulin-like peptide to a single-chain linear peptide that retains the most therapeutically valuable biological actions — specifically the anti-fibrotic effects — while eliminating the cAMP-dependent signalling that may drive unwanted effects. The compound has no human trial data, but a growing and genuinely impressive body of preclinical evidence across cardiac, renal, pulmonary, and vascular disease models.
| At a glance | |
|---|---|
| Full name | B7-33 (H2 relaxin B-chain analogue, residues 7–33 with KRSL extension) |
| Parent hormone | Human relaxin-2 (H2 relaxin) |
| Target receptor | RXFP1 (Relaxin Family Peptide Receptor 1) |
| Key signalling | Preferential pERK1/2 activation; reduced cAMP signalling |
| Class | Functionally selective (biased) single-chain RXFP1 agonist |
| Developed by | Mohammed Akhter Hossain, Ross Bathgate, Chrishan Samuel, John Wade — University of Melbourne / Monash University |
| First reported | 2016 (Chemical Science) |
| Clinical stage | Preclinical only — no published human trials |
| Regulatory status | Not approved anywhere; research compound only |
| Patent | US Patent 10,081,662 B2 — Modified Relaxin B-chain peptides [10] |
The Science Behind It: Understanding Relaxin First
Human relaxin-2 (H2 relaxin) is a peptide hormone produced primarily by the corpus luteum during pregnancy, where its principal known role is to prepare the body for birth — relaxing ligaments, softening the cervix, and causing profound vasodilation of the renal and systemic circulations. Beyond its reproductive roles, H2 relaxin was discovered to have potent effects throughout the body: it is anti-fibrotic, vasodilatory, anti-inflammatory, and cardioprotective. It signals through its cognate G protein-coupled receptor, RXFP1, which is expressed in the heart, kidneys, lungs, blood vessels, and connective tissue throughout the body.[8]
Serelaxin, the recombinant human relaxin-2 formulation developed by Novartis, reached Phase 3 clinical trials for acute heart failure (RELAX-AHF-1 showed improvements in dyspnoea and some mortality signals; RELAX-AHF-2 did not replicate the mortality benefit). The overall clinical programme did not achieve FDA approval, but the biological science behind RXFP1 as a therapeutic target remains credible and actively pursued.[7]
The limitations of serelaxin for broader use are structural and pharmacokinetic: H2 relaxin is a complex two-chain molecule with three disulfide bonds, it is unstable in human serum and difficult to synthesise efficiently, and its strong activation of cAMP signalling is likely responsible for reported detrimental tumour-promoting actions that may preclude long-term use. B7-33 emerged from over a decade of structure-activity relationship work aimed at solving all of these problems simultaneously.[1]
Design and Structure of B7-33
The design process began with the observation that the B-chain of H2 relaxin can be processed in vivo into three active isoforms (B1-29, B1-31, and B1-33). The native B-chain (B1-29) is insoluble in water and functionally inactive in isolation. The solution involved two structural modifications: truncation of six residues from the N-terminus of B1-33 (removing B1-6), giving a peptide starting at position 7; and retention of the four C-terminal residues (KRSL) from the B1-33 isoform, which improved solubility. These results represent the first known example of the minimisation of a two-chain cyclic insulin-like peptide to a single-chain linear peptide that retains potent beneficial agonistic effects.[1]
| Feature | Detail |
|---|---|
| Chain structure | Single-chain linear (no disulfide bonds) |
| Length | 27 residues (positions 7–33 of H2 relaxin B-chain) |
| C-terminal extension | KRSL residues improve solubility |
| Structural conformation | Predominantly random coil (unlike helical native B-chain region in H2 relaxin) |
| Key binding residues | RB13, RB17, IB20 — same residues that drive H2 relaxin’s RXFP1 binding |
| In vitro half-life | ~6 minutes in serum (very short; a recognised limitation) |
Mechanism of Action: The Biased Agonism Story
What RXFP1 normally does
When H2 relaxin binds to RXFP1, it activates multiple downstream signalling pathways simultaneously, including both cAMP (cyclic adenosine monophosphate) — a classical GPCR second messenger — and pERK1/2 (phosphorylated extracellular signal-regulated kinases 1 and 2). The cAMP pathway is associated with some cardiovascular effects but also with the tumour-promoting actions documented in prostate cancer models. The pERK1/2 pathway is more specifically associated with anti-fibrotic effects in fibroblasts — the anti-scarring, collagen-degrading response.[8]
What B7-33 does differently
B7-33 was shown to bind to RXFP1 and preferentially activate the pERK pathway over cAMP in cells that endogenously expressed RXFP1. Thus, B7-33 represents the first functionally selective agonist of the complex GPCR, RXFP1.[1] This is called biased agonism or functional selectivity — a concept of growing importance in GPCR pharmacology, where different ligands can activate the same receptor but in different proportions, producing distinct biological outcomes.
The downstream consequence of this pERK1/2 bias is important. The molecular mechanism behind the strong anti-fibrotic actions of B7-33 involved its activation of RXFP1-angiotensin II type 2 receptor heterodimers that induced selective downstream signalling of pERK1/2 and the collagen-degrading enzyme, matrix metalloproteinase (MMP)-2. Furthermore, in contrast to H2 relaxin, B7-33 did not promote prostate tumour growth in vivo.[1]
| Signalling pathway | H2 relaxin | B7-33 | Practical implication |
|---|---|---|---|
| cAMP activation | Strong | Weak/minimal | Less tumour-promoting concern with B7-33 |
| pERK1/2 activation | Present | Strong (preferential) | Primary anti-fibrotic driver |
| MMP-2 induction | Yes | Yes — equivalent potency in fibroblasts | Collagen degradation; fibrosis resolution |
| RXFP2 activation | Yes | No | More selective; RXFP2 not targeted |
Preclinical Evidence: What the Animal Data Shows
Anti-fibrotic effects — multiple organs
B7-33 significantly diminished airway epithelial thickening, total lung collagen concentration and airway hyperresponsiveness to a similar extent to native H2 relaxin in a 9-week OVA-induced murine model of chronic allergic airway disease. Renal fibrosis models showed equivalent MMP-2 activation and collagen degradation to H2 relaxin.
Heart failure and cardiac remodelling
Treatment with B7-33 significantly lowers TIMP1 and TIMP2 mRNA expression in cardiac tissue 7 days post ischaemia-reperfusion surgery, and left ventricular fibrosis was significantly lower in B7-33-treated animals than in vehicle-treated animals.[3] A 2023 study from Monash University compared B7-33 directly with perindopril (an ACE inhibitor — a standard-of-care drug for heart failure) in an experimental cardiomyopathy model, showing B7-33 reduced left ventricular fibrosis more rapidly than perindopril.[4]
Vascular effects and preeclampsia
Equimolar doses of B7-33 replicated the acute beneficial vascular effects of serelaxin in rat mesenteric arteries and also prevented endothelial dysfunction induced by placental trophoblast conditioned media in mouse mesenteric arteries.[2] The preeclampsia finding is particularly notable — preeclampsia has no approved specific drug treatment, and B7-33’s ability to prevent trophoblast-induced endothelial dysfunction is biologically credible given relaxin’s known role in normal pregnancy vascular adaptation.
Implant anti-fibrosis (foreign body response)
Subcutaneous implantation of PLGA-coated polypropylene samples in mice with B7-33 demonstrated a marked reduction in capsule thickness (49.2%) over a 6-week period.[5] This application — coating implantable medical devices with B7-33 to prevent the fibrotic capsule that forms around foreign materials — represents a clinically relevant use case for biosensors, drug delivery implants, and cell therapy systems.
| Disease model | Species | Key finding |
|---|---|---|
| Allergic airway disease (OVA-induced) | Mouse | Reduced lung collagen, airway thickening, hyperresponsiveness ≈ H2 relaxin |
| Cardiac ischaemia-reperfusion [3] | Mouse | Reduced infarct size; reduced LV fibrosis; improved cardiac function |
| Cardiomyopathy [4] | Mouse | Reduced LV fibrosis; comparable to relaxin; faster than perindopril |
| Renal fibrosis | Rat | Increased MMP-2; collagen degradation equivalent to H2 relaxin |
| Vascular function [2] | Rat / Mouse | Replicates serelaxin’s endothelium-dependent vasodilation; prevents preeclampsia-like endothelial dysfunction |
| Implant encapsulation [5] | Mouse | 49.2% reduction in fibrotic capsule thickness via PLGA coating |
| Prostate tumour [1] | Mouse | Unlike H2 relaxin, B7-33 did NOT promote tumour growth |
The Short Half-Life Problem — and Efforts to Solve It
B7-33 has a short circulation time in vitro in serum (t½ = ~6 min).[1] Six minutes is a significant practical limitation for any compound intended for chronic therapeutic use. The degradation occurs because the unprotected linear peptide is rapidly cleaved by serum proteases. One published approach used lipidation — attaching fatty acid chains to B7-33 to enable binding to serum albumin. By fatty acid conjugation with an appropriate spacer length, the in vitro half-life of B7-33 can be increased from 6 minutes to 60 minutes.[6] A 10-fold improvement, but 60 minutes in vitro still likely represents a very short in vivo half-life by therapeutic standards.
Other approaches under investigation include hydrocarbon stapling (introducing cross-links that constrain conformation and protect from proteases), alpha-aminoisobutyric acid (Aib) substitutions, truncation to minimal active sequences, and polymer drug delivery systems for local, sustained release. This remains an active area of medicinal chemistry.
How B7-33 Compares to Related Compounds
| Compound | Structure | RXFP1 activation | cAMP | pERK | Clinical status |
|---|---|---|---|---|---|
| H2 relaxin (serelaxin) | Two-chain, 3 disulfides | Full agonist | Strong | Strong | Phase 3 (failed primary endpoint); not approved |
| B7-33 | Single-chain linear | Biased/functionally selective | Weak | Preferential | Preclinical only |
| ML290 | Small molecule | Biased allosteric agonist | Minimal | Strong | Preclinical only |
| Long-acting relaxin analogues | Modified two-chain | Full-agonist analogues | Variable | Variable | Preclinical only |
What Is Confirmed and What Remains Unknown
| Confirmed by published data | Not yet established |
|---|---|
| B7-33 binds RXFP1 using same key residues as H2 relaxin [1] | Human pharmacokinetics, efficacy, or safety |
| Preferential pERK1/2 over cAMP activation (biased agonism) [1] | Whether pERK bias translates to preserved efficacy with reduced risk in humans |
| Anti-fibrotic effects in multiple organ models [3][4] | Optimal dose, route, and frequency for any therapeutic application |
| Vascular effects replicate serelaxin in rat arteries [2] | Long-term consequences of RXFP1 biased agonism |
| Does not promote prostate tumour growth (unlike H2 relaxin) [1] | Whether the short half-life can be overcome for chronic dosing |
| Does not activate RXFP2 (more receptor-selective than H2 relaxin) [1] | Clinical efficacy in preeclampsia, heart failure, or other specific indications |
| In vitro half-life of ~6 min; improvable to ~60 min with lipidation [6] | Whether anti-fibrotic effects require sustained or pulsatile receptor engagement |
| PLGA coating achieves 49.2% capsule thickness reduction in mice [5] | Regulatory and clinical development timeline |
Safety Considerations
No human safety data exists for B7-33. Published preclinical toxicology for B7-33 specifically is limited. The following safety-relevant observations come from the available literature:
Absent tumour promotion: B7-33 did not promote prostate tumour growth in mouse models, which has been a concern with the cAMP-activating effects of full relaxin.[1]
No RXFP2 activation: H2 relaxin also activates RXFP2 (the receptor for the related hormone INSL3), which has roles in testicular function and bone metabolism. B7-33’s RXFP2 selectivity reduces potential off-target effects.[1]
Theoretical concerns: Very short half-life raises questions about dosing feasibility; long-term consequences of sustained pERK1/2 signalling via RXFP1 in various tissues are not characterised; immunogenicity has not been evaluated in published studies; effects in pregnant women, children, or immunocompromised populations are unknown.
Regulatory Status and Research Context
B7-33 is an academic research compound. It is not sold by a pharmaceutical company, is not in clinical development (as of April 2026), and carries no regulatory designation from any health authority. It is protected by US Patent 10,081,662 B2 (Modified Relaxin B-chain peptides), held by the University of Melbourne and associated researchers.[10] It does appear on research chemical vendor websites, typically marked “for research use only” and “not for human consumption.” Published studies used material synthesised by the research groups themselves under controlled laboratory conditions. B7-33 is not currently on the WADA prohibited list.
Common Misconceptions
“B7-33 has been tested in humans.”
No. All published B7-33 data comes from in vitro cell culture experiments and animal models. No human clinical trials have been completed or published.
“It’s basically the same as serelaxin.”
Structurally and mechanistically quite different. Serelaxin is recombinant full H2 relaxin — two chains, three disulfide bonds, strong cAMP activation. B7-33 is a single-chain linear peptide that preferentially activates pERK over cAMP.[1] Their downstream biology overlaps but is not identical.
“Biased agonism means it’s safer.”
Biased agonism means it selectively engages certain signalling pathways. Whether this translates to a genuinely improved safety-efficacy profile in humans has not been tested. The rationale is scientifically sound — the tumour-promotion concern is linked to cAMP, and B7-33 shows reduced cAMP activation — but this remains a hypothesis to be tested in clinical trials, not an established fact.[1]
“The short half-life is solved.”
Lipidation extended in vitro half-life from 6 to 60 minutes.[6] This is an improvement, but 60 minutes in vitro likely still represents a very short in vivo half-life. Meaningful chronic therapeutic use would likely require either a dramatically more stable analogue or an implant-based delivery system. This remains an open research problem.
Frequently Asked Questions
Is B7-33 approved for any use?
No. It is a research compound with no regulatory approval anywhere.
What is the most compelling potential application?
Based on the available preclinical data,[3][4] fibrosis-related cardiovascular and renal disease are the most thoroughly studied indications, with acute heart failure and preeclampsia as additional areas of interest.[2] The implant anti-fibrosis application (device coatings) is also a plausible near-term translational opportunity.[5]
Who developed B7-33?
The core team was based at the University of Melbourne and Monash University in Australia. Key figures are Mohammed Akhter Hossain (peptide chemistry), Ross Bathgate (RXFP1 receptor biology, Florey Institute), Chrishan Samuel (organ fibrosis biology, Monash), and John Wade (peptide synthesis, Florey Institute).[11][12][13][14]
How does it compare to other anti-fibrotic peptides?
It is unique in its RXFP1-biased agonism approach. Most other peptides targeting fibrosis work through different pathways (e.g., BPC-157 via growth factor receptors, TB-500 via actin dynamics). B7-33’s direct targeting of a receptor with a validated role in fibrosis resolution across multiple organs gives it a mechanistic specificity that most other anti-fibrotic research peptides lack.
When might human trials begin?
No timeline is publicly available. The short half-life remains a significant barrier to clinical development — the research field is still working on second-generation analogues with improved pharmacokinetics.[6] Preclinical development appears active as of 2023–2024, but no IND filing or clinical trial registration is publicly known.
Key Takeaways
- B7-33 represents a genuine scientific advance — the first functionally selective (biased) agonist of RXFP1, and the first single-chain derivative of a two-chain insulin-like peptide to retain potent biological activity.[1]
- The preclinical evidence across multiple organ systems is consistent and broad — cardiac, renal, pulmonary, and vascular fibrosis models all show positive results.[2][3][4]
- The biased agonism is the central mechanistic innovation — preferential pERK1/2 over cAMP activation may deliver anti-fibrotic benefits without the tumour-promoting concern associated with full relaxin. This is a scientifically credible hypothesis, not yet a proven clinical reality.
- The short half-life is the central pharmacokinetic challenge.[1][6] At ~6 minutes in vitro, B7-33 in its current form is not clinically viable for chronic conditions.
- No human data exists. Every efficacy and safety observation comes from cells and animals. The translation from preclinical to human outcomes in this area has historically been challenging — serelaxin’s clinical programme is instructive on this point.
- B7-33 is firmly a research compound, not a therapeutic. Using it outside of properly supervised laboratory research introduces unknown risks and bypasses the scientific process by which its potential and its risks are being responsibly characterised.
References
Primary Research Articles
- Hossain MA, Kocan M, Yao ST, et al. A single-chain derivative of the relaxin hormone is a functionally selective agonist of the G protein-coupled receptor, RXFP1. Chemical Science. 2016;7(6):3805–3819. doi: 10.1039/C5SC04754D. PMID: 30155023. PMC6013806
- Marshall SA, O’Sullivan K, Ng HH, et al. B7-33 replicates the vasoprotective functions of human relaxin-2 (serelaxin). European Journal of Pharmacology. 2017;807:190–197. PMID: 28478069
- Devarakonda T, Mauro AG, Guzman G, et al. B7-33, a Functionally Selective Relaxin Receptor 1 Agonist, Attenuates Myocardial Infarction-Related Adverse Cardiac Remodeling in Mice. Journal of the American Heart Association. 2020. doi: 10.1161/JAHA.119.015748. PMID: 32295457
- Alam F, Gaspari TA, Kemp-Harper BK, et al. The single-chain relaxin mimetic, B7-33, maintains the cardioprotective effects of relaxin and more rapidly reduces left ventricular fibrosis compared to perindopril in an experimental model of cardiomyopathy. Biomedicine & Pharmacotherapy. 2023;160:114370. PMID: 36753958
- Welch NG, Mukherjee S, Hossain MA, et al. Coatings Releasing the Relaxin Peptide Analogue B7-33 Reduce Fibrotic Encapsulation. ACS Applied Materials & Interfaces. 2019;11(49):45511–45519. PMID: 31713411
- Handley TNG, Praveen P, Tailhades J, et al. Further Developments towards a Minimal Potent Derivative of Human Relaxin-2. International Journal of Molecular Sciences. 2023;24(16):12670. PMID: 37628851
Reviews and Background
- Conrad KP. G-Protein-coupled receptors as potential drug candidates in preeclampsia: targeting the relaxin/insulin-like family peptide receptor 1 for treatment and prevention. Human Reproduction Update. 2016;22(5):647–664. PMC5001498
- Valkovic AL, Bathgate RA, Samuel CS, Kocan M. Understanding relaxin signalling at the cellular level. Molecular and Cellular Endocrinology. 2019;487:24–33. PMID: 30592984
- Mallart S, et al. Characterization of a new potent and long-lasting single chain peptide agonist of RXFP1 in cells and in vivo translational models. Scientific Reports. 2022. doi: 10.1038/s41598-022-24716-2
Patent
- Bathgate RAD, Hossain MA. Modified Relaxin B-chain peptides. US Patent 10,081,662 B2.
Researcher and Institutional Profiles
- Mohammed Akhter Hossain, PhD — Florey Institute of Neuroscience and Mental Health / School of Chemistry, University of Melbourne. Principal inventor and peptide chemistry lead for B7-33.
- Ross Bathgate, PhD — Florey Institute of Neuroscience and Mental Health, University of Melbourne. RXFP1 receptor biology lead.
- Chrishan Samuel, PhD — Cardiovascular Disease Program, Monash Biomedicine Discovery Institute, Monash University. Organ fibrosis biology lead.
- John Wade, PhD — Florey Institute and School of Chemistry, University of Melbourne. Peptide synthesis expert.
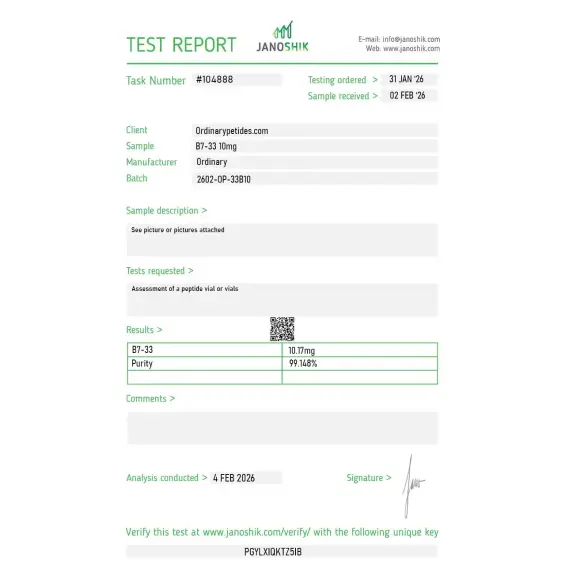
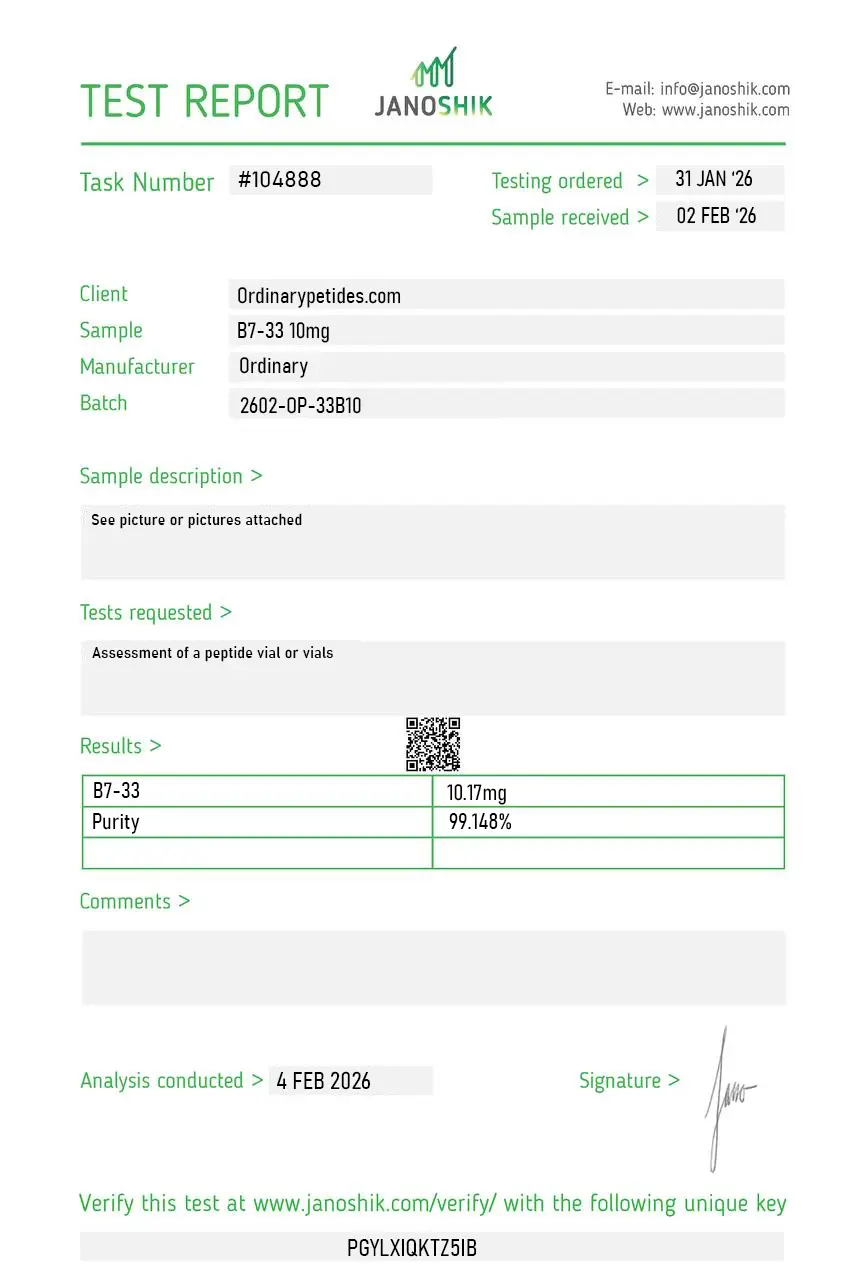
Certificate of Analysis
An independent test report is available for B7-33. This report provides batch-level documentation and analytical verification information for research reference.
Based on 1 reviews
5.0
The biased-agonism property is exactly why we sought it out — B7-33 activates RXFP1 toward pERK signaling while largely bypassing the cAMP arm that native relaxin drives, which in fibrosis models decouples the anti-fibrotic effect from the proliferative cAMP response. For dissecting which RXFP1 downstream branch carries the anti-fibrotic signal, that functional bias is a tool you can't replicate with full-length relaxin. The material reproduced the pERK-selective profile in our cardiac fibroblast assays.
B7-33 is primarily used in laboratory research investigating antifibrotic signaling, collagen remodeling, and extracellular matrix regulation via activation of the RXFP1 receptor.
In research contexts, B7-33 is studied for its potential influence on collagen turnover and fibrotic pathway modulation, which are central to scar formation and dermal remodeling processes.
B7-33 does not directly "remove" scars; rather, in experimental models it may influence collagen regulation and reduce profibrotic signaling pathways associated with scar formation.
It activates the relaxin receptor RXFP1, triggering signaling cascades linked to antifibrotic activity and extracellular matrix remodeling in preclinical research.
Available preclinical data suggest a relatively favorable safety profile, but comprehensive long-term human safety data are limited, and it remains an experimental compound.
It is a short peptide analogue of relaxin designed to activate RXFP1 more selectively than relaxin itself.
Yes. The Guide to Pharmacology explicitly classifies it among peptide ligands.
Primarily for antifibrotic, vascular, and cardioprotective indications — including cardiac and pulmonary fibrosis, remodeling after myocardial infarction, and vascular dysfunction.
In the reviewed reliable sources, a mature published clinical program specifically for B7-33 is not apparent; the molecule looks like a preclinical candidate.
B7-33 is structurally simpler, easier to synthesize, and has a biased RXFP1 profile with greater emphasis on ERK1/2 and less on cAMP.
Very short serum stability and lack of mature clinical development.
The key point is not to treat B7-33 as if it were already a proven antifibrotic agent. At present, it is a promising preclinical peptide, not a finished therapy.
B7-33 is a synthetic single-chain peptide derived from the B-chain of human relaxin-2 — a naturally occurring hormone best known for its roles in pregnancy, tissue remodeling, and cardiovascular regulation. It was developed by a research group at Monash University in Australia through over a decade of structure-activity relationship studies on the relaxin receptor system. B7-33 represents a significant engineering achievement — it is the first known example of successfully minimizing a complex two-chain, disulfide-rich insulin-like peptide into a single-chain linear peptide that retains potent biological activity. This simplification dramatically reduces the cost and complexity of production compared to full-length relaxin-2 or its pharmaceutical form serelaxin.
Full-length relaxin-2 and its recombinant pharmaceutical form serelaxin activate the RXFP1 receptor through two parallel intracellular pathways — the cAMP pathway and the ERK1/2 pathway. While this produces broad therapeutic effects, the cAMP signaling component has been linked to tumor-promoting activity in preclinical models, raising concerns about long-term use. B7-33 is a functionally selective or "biased" agonist — it binds RXFP1 and preferentially activates the ERK1/2 pathway while minimizing cAMP activation. This selective signaling retains the antifibrotic and cardioprotective benefits of relaxin while avoiding the tumor-promoting effects associated with cAMP overstimulation. Crucially, in animal studies B7-33 did not promote prostate tumor growth, unlike full-length relaxin.
B7-33 binds RXFP1 receptors — expressed widely in the heart, kidneys, blood vessels, and lungs — and activates RXFP1-angiotensin II type 2 receptor heterodimers, triggering downstream ERK1/2 phosphorylation and upregulation of matrix metalloproteinase-2 (MMP-2), a key collagen-degrading enzyme. This mechanism directly breaks down pathological collagen accumulation and reduces fibrotic scar tissue. Simultaneously it promotes vasodilation through nitric oxide synthesis, reduces NLRP3 inflammasome activation, suppresses pro-inflammatory cytokines, and protects cardiomyocytes from ischemia-reperfusion injury. Its selectivity for the ERK1/2 pathway makes it a precision tool for targeting fibrosis and tissue repair without broadly disrupting endocrine signaling.
The most extensively studied application is cardiac protection and anti-fibrosis. In mouse models of myocardial infarction, B7-33 treatment post-ischemia-reperfusion significantly reduced infarct size, preserved cardiac function, and attenuated adverse cardiac remodeling. In three separate rodent models of heart and lung fibrosis, B7-33 prevented and reversed fibrosis with potency comparable to serelaxin. Research has also explored renal fibrosis, pulmonary fibrosis, wound healing, anti-fibrotic coatings for implantable medical devices — where B7-33 released from biodegradable polymer coatings reduced fibrotic capsule thickness by 49% in mouse models — and potential applications in preeclampsia and obstetric conditions. A significant pharmacokinetic challenge identified is B7-33's very short serum half-life of approximately 6 minutes, prompting research into lipidated analogs that extend half-life to 60 minutes.
In preclinical research settings B7-33 is administered by subcutaneous or intravenous injection. Doses in animal studies vary widely by model and condition. It has no approved human dosing protocol as it has not entered human clinical trials. Researchers are actively developing lipidated analogs and controlled-release formulations to address its short half-life and improve clinical translatability.
B7-33 has a promising early safety profile in preclinical studies. The most commonly noted effects are mild injection site reactions. Due to its vasodilatory mechanism through nitric oxide enhancement, mild hypotension and headache are potential effects at higher doses. Importantly, unlike serelaxin and full-length relaxin-2, it does not appear to promote tumor growth in animal models — a key safety advantage. No serious adverse events have been documented in preclinical studies, though comprehensive human safety data does not yet exist.
As B7-33 has not entered human clinical trials, it should not be used outside of formally approved research settings. People with low blood pressure or conditions sensitive to vasodilation should exercise particular caution. Those with hormone-sensitive conditions should discuss its use with a physician given its action on RXFP1 — a receptor involved in reproductive physiology. Pregnant women should avoid it despite relaxin's natural role in pregnancy, as the pharmacological doses and biased signaling profile are not equivalent to physiological relaxin. As with all research peptides, qualified medical supervision is essential.