

FST 344
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
FST 344: When Muscle Biology Becomes Truly Interesting
FST 344 is the 344-amino acid form of follistatin, a natural protein studied in a research context as a potent regulator of myostatin and activin A — the very signals that normally restrain the growth of muscle tissue.
In preclinical data, AAV-mediated delivery of the FS-344 gene produced pronounced increases in muscle mass and strength in mice and primates, and in early clinical studies in Becker muscular dystrophy and sIBM, researchers observed improvement in functional measures in some patients without serious adverse events within the framework of controlled gene therapy.
This is precisely why FST 344 generates such interest: it is not a story about "yet another peptide," but about intervention in the very system that brakes muscle growth. Accuracy matters here, however — the published data relate to gene delivery of FS-344, not to unregulated peptide injections, which the article explicitly describes as a separate and far riskier story.
For the reader, this makes FST 344 particularly intriguing not as a ready-made solution, but as a compelling research platform at the intersection of muscle biology, gene therapy, and the medicine of the future. In short: the molecule commands attention not because of hype, but because within the context of study it genuinely has the ability to shift muscle biology.
Follistatin-344 (FS344 / FST-344): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Follistatin-344 sits at the intersection of reproductive endocrinology, muscle biology, and gene therapy — a compound whose discovery history traverses three entirely different scientific contexts. It was first isolated in 1987 from porcine ovarian follicular fluid as an FSH-suppressing protein. It was later identified as an activin-binding protein. And following the 1997 discovery of myostatin, it was found to be one of the most potent natural inhibitors of the myostatin signalling pathway. Mice overexpressing follistatin develop muscles 2–3 times normal size — more even than myostatin-knockout mice, because follistatin also inhibits activin A and other TGF-β family members that independently constrain muscle growth.[6]
The “344” in the name refers to the amino acid length of the preprotein precursor encoded by the FS344 mRNA transcript — a product of alternative splicing. After cleavage of the 29-amino acid signal peptide, the actual secreted protein is follistatin-315 (FS315), the principal circulating form. Community vendors selling “follistatin-344” as an injectable product are typically selling recombinant FS315 protein — not the 344-residue preprotein, which requires intracellular processing before secretion.
The clinical evidence for follistatin-344 gene therapy is the most meaningful for a myostatin-targeting strategy: the Phase 1/2 sporadic inclusion body myositis trial (2017) produced +56 metres/year improvement vs. −25.8 metres/year in matched untreated controls — a statistically significant functional benefit in a disease with no effective treatment.[8]
| At a glance | |
|---|---|
| Common names | Follistatin-344; FST-344; FS344; follistatin (general) |
| Type | Monomeric secreted glycoprotein; endogenous TGF-β antagonist |
| Gene designation | FST gene; FS344 = 344-amino acid preprotein transcript |
| Mature secreted protein | FS315 (after 29-AA signal peptide cleavage) |
| Isoform basis | Alternative splicing: FS344 includes exon 6; FS317 excludes it |
| MW (mature FS315) | ~35 kDa (protein core ~32 kDa + glycosylation) |
| Discovery | Ueno et al., 1987; isolated from porcine follicular fluid |
| Primary biological role | Extracellular antagonist of activin, myostatin, GDF-11, select BMPs |
| FDA status | ❌ Not approved; gene therapy (AAV1-FS344) in clinical development |
| WADA | ❌ Prohibited at all times — S2 |
Nomenclature: Resolving the FS344 / FS315 Confusion
Alternative splicing occurs at the 3′ end of the FST gene between exon 5 and exon 6. Splicing out of intron 5 generates a stop codon following the last amino acid of exon 5, terminating the coding sequence for FS317. An alternative splice site results in the inclusion of exon 6 and generates FS344. After translation and prior to activation, follistatin undergoes cleavage of the 29-amino acid signal peptide, resulting in polypeptides FS315 (long-isoform from FS344) and FS288 (short-isoform from FS317).[3]
| mRNA/Gene designation | Preprotein length | Signal peptide | Mature protein |
|---|---|---|---|
| FS344 | 344 AA | 29 AA | FS315 (circulating long isoform) |
| FS317 | 317 AA | 29 AA | FS288 (cell-surface short isoform) |
The number refers to the preprotein — the full unprocessed translation product before signal peptide cleavage. The biologically active secreted forms are FS315 and FS288. An intermediate form, FS303, arises from C-terminal proteolytic trimming of FS315 and is found primarily in follicular fluid. The gene therapy literature uses “FS344” to refer to the transgene construct; the protein biology literature uses “FS315” to describe the circulating protein. Community vendors selling “follistatin-344” as an injectable are selling recombinant FS315 protein, not the 344-residue preprotein.
Discovery: From FSH Suppressor to Muscle Builder
Follistatin was independently isolated from porcine ovarian follicular fluid in 1987 by Ueno et al. (Salk Institute) and Robertson et al. (Monash University). It was named for its initial characterisation as an FSH-suppressing protein (FSP). It was earlier called FSH-suppressing protein (FSP); at the time of its initial isolation from follicular fluid, it was found to inhibit the anterior pituitary’s secretion of follicle-stimulating hormone.[1]
In the early 1990s, the mechanism of FSH suppression was clarified: follistatin binds activin — the ovarian hormone that promotes FSH secretion — with extraordinarily high affinity (Kd ~45 pM), sequestering activin before it could signal. This repositioned follistatin as a broadly important TGF-β superfamily regulator. Following McPherron and Lee’s 1997 discovery of myostatin, follistatin’s known ability to bind multiple TGF-β superfamily members prompted investigation of its effects on myostatin. The results were striking: transgenic mice expressing high levels of follistatin show a 194–327% increase in muscle mass relative to controls, significantly greater than in myostatin-null animals, suggesting follistatin enhances muscle growth not solely through inhibiting myostatin but also by inhibiting activin A, activin B, and GDF-11 — all of which independently constrain muscle mass via ActRIIB.
Protein Structure: The Follistatin Domain Architecture
Follistatin is a monomeric glycoprotein with a distinctive multidomain structure designed for high-affinity ligand capture: an N-terminal unique domain (ND/Fs0, ~63 AA) critical for initial TGF-β family ligand contact; three follistatin domains (FSD1, FSD2, FSD3) with ~65–70 AA each containing 10 conserved cysteines that form the core binding scaffold; and a 26-residue acidic C-terminal tail present in FS315 only. The full-length FS315 has an acidic 26-residue C-terminal tail not present in the shortest form FS288; accordingly, the biochemistry of each isoform is distinct, including their ability to bind to cell surface proteoglycans, an activity that ranks in the order FS288 > FS303 > FS315.[2]
Crystal structure studies reveal how follistatin neutralises its targets: follistatin molecules wrap around the back of the ‘wings’ of activin, blocking the type II receptor-binding site. This two-point blocking makes follistatin one of the most potent inhibitors of TGF-β superfamily signalling known — more effective than antibodies targeting only one binding surface.
Isoform Biology: Why FS344/FS315 Was Chosen for Therapy
FS288 (from FS317 transcript): High affinity for cell surface heparan sulphate proteoglycans (HSPG); membrane-associated and locally active; found in ovary and reproductive tissues; potent activin neutraliser; clinical concern: strong FSH suppression with high reproductive tissue affinity.
FS315 (from FS344 transcript): Circulates freely in blood as the principal circulating form of follistatin in human serum; acquires HSPG binding only after complexing with activin (activin-induced conformational change); ~10-fold lower affinity for activin than FS288 in reproductive tissues.[3]
The therapeutic rationale for selecting the FS344 transgene (encoding FS315): lower activin affinity reduces FSH suppression and reproductive disruption; circulating distribution reaches muscles at sites remote to the injection; less aggressive reproductive axis suppression while still achieving potent myostatin inhibition at muscle cells.
The FS344 Gene Therapy Strategy: Why Inject a Gene, Not a Protein?
This is the pivotal question distinguishing the legitimate AAV gene therapy approach from community injectable protein use. Problems with injecting follistatin protein directly: short plasma half-life (measured in hours) requiring repeated injections; immediate systemic distribution including to ovarian and pituitary tissues where FSH suppression is not desired; and systemic GDF-11 suppression risking bone loss (documented in follistatin-overexpressing mice).
The gene therapy approach delivers the FS344 transgene by intramuscular injection of AAV1; transduced muscle cells continuously secrete FS315 locally; local concentrations at target muscle are pharmacologically relevant while systemic concentrations are modest; and single injection provides durable expression (AAV1 persists as episomal DNA in post-mitotic muscle nuclei). Community injectable use bypasses all of this safety engineering.
Clinical Evidence
Nonhuman primate safety and efficacy (2009)
Before human trials, Rodino-Klapac, Mendell and colleagues at Nationwide Children’s Hospital studied AAV1-FS344 in cynomolgus macaque monkeys: single intramuscular injection to quadriceps produced 15–27% increase in quadriceps muscle size with corresponding strength gains; long-term transgene expression without organ pathology; reproductive organs showed no abnormalities post-mortem; pituitary-gonadal axis function preserved.[5]
Phase 1/2 — Becker Muscular Dystrophy (2015)
AAV1.CMV.FS344 was delivered by direct bilateral intramuscular quadriceps injections to six BMD patients. In cohort 1 (three subjects; 3 × 10¹¹ vg/kg/leg), patients 01 and 02 improved 58 metres and 125 metres respectively on the 6-minute walk test — the first gene therapy clinical trial to show functional improvement in any form of muscular dystrophy. Caveats: six subjects; no placebo control; gains inconsistent across patients. The trial established safety and proof-of-biological activity.[7]
Phase 1/2 — Sporadic Inclusion Body Myositis (2017)
rAAV1.CMV.huFS344 (6 × 10¹¹ vg/kg) was delivered to the quadriceps muscles of both legs of six sporadic inclusion body myositis subjects. Performance, annualised to a median 1-year change, improved +56.0 m/year for treated subjects compared to a decline of −25.8 m/year in untreated subjects matched for age, gender, and functional capacity (p = 0.01).[8] For patients with sIBM who experience progressive functional decline and no therapeutic options, this >80 m/year functional difference is clinically meaningful. Important caveats: six treated subjects; matched historical comparison (not randomised placebo control); potential for performance bias; N is too small for definitive regulatory conclusions.
Broader Biology: Follistatin Beyond Muscle
Follistatin is expressed in virtually every tissue and participates in multiple biological systems. Embryonic development: Global follistatin knockout mice die within hours of birth with profound developmental abnormalities; the ectoderm-neuroectoderm transition during neural development requires follistatin-mediated BMP inhibition. Metabolic regulation: Elevated circulating follistatin levels are associated with increased risk of type 2 diabetes, early death, heart failure, stroke, and chronic kidney disease. The “more follistatin = healthier” model is too simple; chronically elevated systemic follistatin carries metabolic risk. Bone: Follistatin inhibits GDF-11 (a promoter of osteogenesis); mice overexpressing follistatin show decreased bone mineral density and spontaneous fractures. Cancer: Activin plays a significant role in cellular proliferation, while follistatin acts as safeguard against uncontrolled cellular proliferation; paradoxically, follistatin overexpression is found in several cancers where loss of activin’s growth-suppressive signal promotes tumour progression.
Community Injectable Use: Documented Serious Adverse Effects
⚠️ Central serous chorioretinopathy (CSCR): A 2020 case series documented 11 male bodybuilders who developed CSCR after subcutaneous follistatin-344 injections. All patients injected complete 1 mg vials (approximately 10 times typical recommended doses). 10 patients developed unilateral CSCR; one had bilateral involvement. Single-injection cases saw complete resolution after an average of 2.3 months, but high-dose cases carried risk of permanent vision impairment. CSCR involves fluid accumulation under the retina causing blurred and distorted vision.[9]
⚠️ FSH suppression: Myostatin inhibition itself affects the reproductive axis; systemic follistatin administration adds activin suppression on top of this, amplifying FSH disruption. This has implications for fertility and HPG axis function in both males and females.
⚠️ Product quality: More than half of black-market follistatin products either contain no follistatin or are contaminated with bacterial expression tags and other growth peptides. Follistatin is a glycosylated protein requiring mammalian cell expression systems; bacterial expression produces non-glycosylated forms with altered biological activity and immunogenicity potential.
Regulatory and Anti-Doping Status
AAV1-FS344 has completed Phase 1/2 trials for BMD and sIBM with orphan drug designation for sIBM (Milo Biotechnology). Injectable follistatin protein is not approved for any indication. All myostatin inhibitors including follistatin are prohibited under WADA S2 at all times; both the gene therapy vector and injectable protein administration would constitute violations. Detection approaches for AAV-based gene therapies are under active development by WADA-affiliated laboratories.
Common Misconceptions
“Follistatin-344 is a peptide.”
Follistatin is a large glycosylated protein (~35 kDa when glycosylated) — an order of magnitude larger than most peptides in this series, with a complex three-dimensional structure and multiple disulfide bonds. It cannot be synthesised by standard solid-phase peptide synthesis (SPPS) and must be produced by recombinant expression in mammalian cell systems. Products claiming to be SPPS-synthesised “follistatin peptide” either contain only a fragment of unknown activity or are mislabelled.
“The clinical trials proved it works for muscle building.”
The clinical trials studied it in patients with muscular disease using AAV gene therapy — not injectable protein to healthy individuals. Extrapolating the +56 metres/year walk improvement in sIBM to healthy muscle hypertrophy in people without muscle disease is not scientifically supported.[8]
“Follistatin has no side effects because it’s natural.”
Endogenous follistatin levels are tightly regulated and compartmentalised. Pharmacologically elevating circulating FS315 beyond normal levels via injection disrupts the activin/FSH axis, risks bone loss, is associated with metabolic disease at elevated levels, and at community doses has caused CSCR with vision loss. “Natural” does not mean “safe at pharmacological doses.”
Key Takeaways
- “FS344” is a gene/mRNA designation, not the protein. The secreted mature protein from the FS344 transcript is FS315. This distinction matters for product quality assessment and pharmacological prediction.
- The isoform choice (FS344/FS315 over FS317/FS288) was deliberate and scientifically motivated. FS315’s lower activin affinity, circulating distribution, and reduced reproductive tissue binding were specific reasons for its selection as the therapeutic transgene — properties absent in HSPG-bound FS288.
- The gene therapy route was specifically designed to avoid the systemic risks of injected follistatin protein. Intramuscular AAV delivery provides local muscle expression without HPG axis disruption and systemic GDF-11/BMP suppression. Community injectable use bypasses all of this safety engineering.
- ✅ The sIBM clinical data is the most positive functional gene therapy result for a myostatin-targeting strategy. Small uncontrolled trial, but +56 m/year vs. −25.8 m/year in a disease with no effective treatment represents a clinically meaningful signal.[8]
- ⚠️ Documented CSCR at high doses in bodybuilders is a real safety signal. Vision damage from injectable follistatin is not theoretical; the 2020 case series of 11 bodybuilders who developed retinal pathology is a direct and sobering real-world adverse event record.[9]
- Chronic elevation of follistatin is not simply beneficial. Epidemiological data associate higher circulating follistatin with increased cardiovascular and metabolic disease risk. The assumption that “more follistatin = more muscle = healthier” is a significant oversimplification of a complex regulatory protein.
References
Discovery
- Ueno N, Ling N, Ying SY, Esch F, Shimasaki S, Guillemin R. Isolation and partial characterisation of follistatin: a single-chain Mr 35,000 monomeric protein that inhibits the release of follicle-stimulating hormone. PNAS. 1987;84(23):8282–8286.
Structure
- Structural basis for the inhibition of activin signalling by follistatin. PMC1409725. EMBO Journal. 2006.
Isoforms and Tissue Distribution
- Differential distribution of follistatin isoforms: application of a new FS315-specific immunoassay. Journal of Clinical Endocrinology and Metabolism. 2004;89(10):5067.
- The follistatin-288 isoform alone is sufficient for survival but not for normal fertility in mice. PMC2840692. 2010.
Preclinical and NHP Gene Therapy
- Follistatin gene delivery enhances muscle growth and strength in nonhuman primates. PMC2852878. Science Translational Medicine. 2009.
- Inhibition of myostatin with emphasis on follistatin as a therapy for muscle disease. PMC2717722. 2009.
Clinical Trials
- A Phase 1/2a follistatin gene therapy trial for Becker muscular dystrophy. PMC4426808. Molecular Therapy. 2015.
- Mendell JR et al. Follistatin gene therapy for sporadic inclusion body myositis improves functional outcomes. Molecular Therapy. 2017;25(4):870–879. PMC5383643
Adverse Effects
- Case series: Central serous chorioretinopathy in bodybuilders after follistatin-344 injections. 11 cases. 2020.
Key Investigators
- Jerry R. Mendell, MD — Nationwide Children’s Hospital, Columbus; Director, Center for Gene Therapy; principal investigator of the BMD and sIBM Phase 1/2 AAV-FS344 clinical trials; first researcher to demonstrate functional improvement in muscular dystrophy via gene therapy.
- Louise R. Rodino-Klapac, PhD — former Nationwide Children’s Hospital; co-investigator on AAV-FS344 trials; now at Sarepta Therapeutics.
- Wylie Vale, PhD and Roger Guillemin, MD, PhD — Salk Institute; foundational work on TGF-β superfamily including activins; provided scientific context for follistatin discovery.
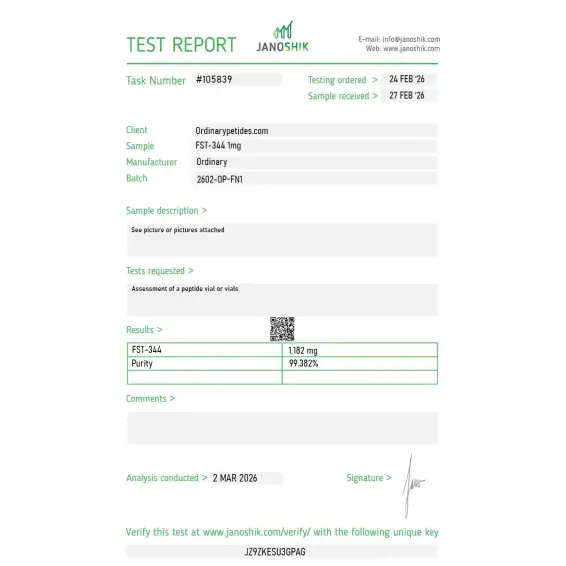
Certificate of Analysis
An independent test report is available for FST-344 1mg. This report provides batch-level documentation and analytical verification information for research reference.

Based on 1 reviews
5.0
Asked their team about endotoxin levels before ordering — they came back within a day with specific LPS data below 1 EU/mg, which for any recombinant going into primary cell culture is the verification that matters more than purity alone. Documentation transparency was the deciding factor for the order.
FST-344 is a naturally occurring isoform of follistatin, a secreted glycoprotein found throughout the body in tissues including the pituitary, liver, kidney, bone marrow, and blood vessels. It is a 344-amino acid precursor protein that undergoes post-translational processing to produce the circulating isoform FS-315. It is best known for its powerful ability to inhibit myostatin — the protein that limits muscle growth — making it one of the most researched compounds in the field of muscle development and regenerative medicine.
FST-344 works by competitively binding to myostatin and activin, preventing them from attaching to their receptors on muscle cells. Myostatin normally acts as a brake on muscle growth, so blocking it removes that limitation and allows for increased muscle fiber development. It also inhibits activin, which plays a role in inflammation. The combined suppression of both proteins supports muscle hypertrophy, tissue repair, and reduced systemic inflammation.
Research across animal models has shown pronounced increases in muscle size and strength, improved recovery from muscle injury, and reductions in body fat. Additional areas under investigation include improved insulin sensitivity and glucose regulation, increased bone density through effects on osteogenesis, potential hair follicle growth improvements, and neuroprotective effects. In aged animals with muscular dystrophy, FST-344 gene delivery reversed muscle deterioration even when administered late in disease progression.
No. FST-344 is not approved by the FDA or any major regulatory authority for therapeutic use in humans. It is primarily used as a research compound in preclinical and laboratory settings. A gene therapy version delivered via adeno-associated virus (AAV1) has entered early clinical trials for muscular dystrophy, and companies like Minicircle offer it as an investigational longevity gene therapy administered at international partner clinics outside the United States.
In research and investigational gene therapy settings it is delivered via intramuscular or subcutaneous injection, often using an AAV1 viral vector to carry the FST-344 gene directly into muscle tissue. Effects from gene therapy administration can last approximately one year. As a standalone peptide it is also sold on the grey market in injectable form, though purity and authenticity of such products are highly unreliable — one study found that out of 17 supplements marketed as follistatin, only nine actually contained the compound.
The most commonly reported side effect in gene therapy trials is a mild increase in LDL cholesterol in roughly one-third of patients. A major biological concern is FST-344's ability to suppress follicle-stimulating hormone (FSH) through its effects on the activin-inhibin axis, which can disrupt reproductive hormones. Uncontrolled systemic use may also theoretically stimulate growth in unintended tissues. Long-term safety data in humans remains very limited.
It is not suitable for pregnant women or those planning to become pregnant due to its effects on reproductive hormones. Anyone with hormone-sensitive conditions, active cancer, or those not under qualified medical supervision should avoid it. Because it is largely unregulated outside of clinical trials, self-administration carries significant unknown risks and should not be attempted.





