
GDF-8
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
GDF-8 (Myostatin): The Natural Muscle Brake That Turned Into a Major Research Target
GDF-8, better known as myostatin, is the body's own "stop signal" for muscle growth — a natural protein that, in research models, limits muscle fiber expansion, slows myoblast proliferation, and pushes muscle biology away from overgrowth. Interest in it exploded after knockout mice, cattle, dogs, and even rare human cases with loss-of-function mutations showed dramatically increased muscle mass, turning myostatin from a quiet regulator into a headline molecule in muscle science.
In the research context, GDF-8 works through the ActRIIB/Smad2/3 pathway and also affects protein synthesis and breakdown, which is why it is studied not only in muscle wasting disorders but also in metabolism, bone biology, and recovery after injury. What makes it especially compelling is that blocking GDF-8 is not just about "more muscle" — in published studies it has been linked to meaningful functional changes in conditions such as spinal muscular atrophy.
At the same time, the field has learned the hard way that this pathway is biologically powerful and not as simple as flipping one switch and getting superhero results. That is exactly why GDF-8 remains one of the most fascinating frontiers in modern muscle research: not hype, but a real molecular control point with unusually big consequences.
GDF-8 / Myostatin: A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Few biological targets have generated as much scientific excitement — and as many clinical development failures — as myostatin/GDF-8. The biology is among the most compelling in all of musculoskeletal medicine: a single gene whose knockout doubles muscle mass in mice; a mutation that creates “double-muscled” cattle; a human infant born with myostatin loss-of-function who exhibited extraordinary muscle development. The concept is simple and beautiful: a molecular brake on muscle growth that, if released, allows muscles to grow beyond their normal ceiling.
The translation to clinical medicine has proven far harder. First-generation myostatin inhibitors increased muscle mass in animal models but failed repeatedly in Phase 3 trials to produce meaningful improvements in muscle function. The distinction between muscle mass (what you measure on a scan) and muscle function (what matters to the patient) turned out to be unbridgeable in diseased muscle lacking the neural and structural architecture to use additional mass productively. The field has since evolved substantially.
| At a glance | |
|---|---|
| Full name | Growth differentiation factor 8 (GDF-8); also myostatin (MSTN) |
| Protein type | TGF-β superfamily member; secreted homodimeric growth factor |
| Gene | MSTN; chromosome 2q32.2 in humans |
| Primary role | Negative regulator of skeletal muscle mass |
| Discovery | McPherron, Lawler, Lee (Johns Hopkins, 1997) |
| Receptor | Activin receptor type IIB (ActRIIB); also ActRIIA |
| Downstream signalling | Smad2/3 → Smad4 complex → nuclear translocation; Akt inhibition |
| FDA-approved therapeutic | ❌ None as of April 2026; apitegromab BLA resubmission expected 2026 |
| WADA status | Myostatin inhibitors prohibited under S2 |
The Biology: Why Myostatin Matters
Discovery: the “mighty mouse”
In 1997, Se-Jin Lee and Alexandra McPherron at Johns Hopkins reported the discovery of a new TGF-β superfamily member expressed specifically in skeletal muscle. They named it myostatin — “muscle halt” — and demonstrated in knockout mice its function: a strain of mice lacking the gene has approximately twice as much muscle as normal mice, subsequently named “mighty mice.” In the same year, two independent papers confirmed myostatin’s role in cattle: Belgian Blue cattle carry an 11-nucleotide deletion in the third exon causing a frameshift that eliminates virtually all of the mature active region; Piedmontese cattle carry a missense mutation substituting an invariant cysteine. These famous double-muscled breeds had been selectively bred for decades without understanding why — the 1997 papers provided the molecular answer.[1][2][3]
Natural history across species
MSTN-knockout mice exhibit a 2–3-fold increase in muscle mass, with both larger muscle fibres (hypertrophy) and greater fibre number (hyperplasia), a higher proportion of type II fibres, and decreased adipose tissue. Belgian Blue cattle show approximately 40% more total muscle mass, arising primarily from hyperplasia. A 2004 report described a German infant boy born with exceptional musculature and extraordinary strength — genetic analysis revealed a loss-of-function mutation in the myostatin gene; his mother, a professional athlete and heterozygous carrier, had above-average muscle mass. This human case provides the strongest possible evidence that myostatin inhibition in humans produces the expected muscle phenotype without catastrophic consequences in the congenital/developmental setting.
GDF-8 and GDF-11: the important distinction
Myostatin (GDF-8) has a close structural paralogue — GDF-11 — sharing ~90% sequence identity in the mature domain. GDF-8 and GDF-11 have opposing functions in bone: GDF-8 inhibits bone formation while GDF-11 promotes osteogenesis. Follistatin overexpression increases skeletal muscle mass by suppressing myostatin but also diminishes bone mineral density and induces bone fractures through binding and repressing GDF-11 activity — the opposing roles of myostatin and GDF-11 must be carefully considered when generating myostatin inhibitors for therapeutic intervention. This finding dramatically complicated the follistatin and pan-ActRIIB inhibitor strategies: gaining muscle while losing bone is not an acceptable clinical trade-off for most indications.
Molecular Structure and Processing
GDF-8/myostatin is produced as a 375-amino acid precursor (prepromyostatin), processed through several steps: signal peptide cleavage; homodimerisation of two promyostatin chains; furin convertase cleavage (Golgi) separating the N-terminal prodomain from the C-terminal mature domain (the two fragments remain non-covalently associated as the latent complex); and finally tolloid metalloproteinase cleavage (extracellular), which dissociates the prodomain from the 12.5 kDa C-terminal mature GDF-8 homodimer — the form that binds receptors and is biologically active.
This proteolytic activation cascade provides multiple intervention points: inhibit tolloid metalloproteinase cleavage (keep myostatin in latent complex — apitegromab’s mechanism); neutralise mature GDF-8 with antibodies (first-generation approach); block ActRIIB receptor with soluble decoy receptor; administer endogenous antagonists (follistatin) via gene therapy; or administer GDF-8 propeptide fragments as competitive inhibitors.
Mechanism of Action: The Smad Signalling Pathway
Active mature GDF-8 binds and activates the activin type II receptor (ActRIIB) at the cell surface. Subsequent autophosphorylation of ActRIIB recruits and activates the type I receptor ALK-4 or ALK-5. Activated type I receptor kinase phosphorylates Smad2 and Smad3, allowing them to interact with Smad4 (co-Smad) and translocate to the nucleus to activate target gene transcription. Importantly, myostatin receptor activation also inhibits Akt (protein kinase B) — a major determinant of muscle protein synthesis and cell proliferation.[4]
The dual anti-anabolic mechanism — Smad2/3 transcriptional activation promoting muscle atrophy genes, AND Akt inhibition reducing protein synthesis — means myostatin acts through the same pathways (in reverse) as IGF-1 and insulin. Blocking myostatin operates as a mirror image of activating the IGF-1/PI3K/Akt/mTOR axis. Additionally, myostatin maintains satellite cells in quiescence; when myostatin is absent, satellite cells activate, proliferate, and contribute to myofibre growth — the mechanism underlying hyperplasia in addition to hypertrophy.
GDF-8 and the New GLP-1 Combination Context
The most clinically significant new development in 2025 involves an intersection with GLP-1 pharmacology. GLP-1 agonists (semaglutide, tirzepatide) produce profound weight loss, but approximately 15–20% of weight lost is lean mass — a consequence of caloric restriction triggering evolutionary muscle-minimisation mechanisms including elevated myostatin. GDF-8 and activin A are the two major ActRIIA/B ligands mediating the muscle-minimisation actions of ActRIIA/B receptors, and dual blockade can prevent muscle loss associated with GLP-1 receptor agonists — and even increase muscle mass — in both obese mice and non-human primates; moreover, this muscle preservation enhances fat loss and is metabolically beneficial.[6]
The Therapeutic Inhibitor Landscape
GDF-8 propeptide (the natural inhibitor)
The propeptide of GDF-8 is its endogenous inhibitor, remaining non-covalently associated with mature GDF-8 in the latent complex. Recombinant GDF-8 propeptide, including engineered “super-propeptide” variants with enhanced affinity, has been studied in preclinical models with muscle mass increases in mice and rats. No human clinical trial data has been published for GDF-8 propeptide as a standalone therapeutic. This is the compound typically discussed in the community as “injectable GDF-8 propeptide” — a research reagent without clinical evidence.
Follistatin and FS344 (gene therapy approach)
Follistatin (FST) is an endogenous secreted protein that binds and neutralises multiple TGF-β family members including myostatin, GDF-11, and activins. Transgenic mice expressing high levels of follistatin show a 194–327% increase in muscle mass relative to controls — substantially greater than myostatin-null animals alone, suggesting follistatin enhances muscle growth through mechanisms beyond just myostatin inhibition. The problem with systemic follistatin: it suppresses FSH (hence its name from ovarian biology) and inhibits activins and BMPs beyond myostatin, disrupting the HPG axis and potentially compromising bone density through GDF-11 inhibition.
The solution: AAV-FS344 gene therapy. The FS344 isoform, delivered by AAV directly into muscle, produces local follistatin-315 expression that remains largely locally active, has 10-fold lower activin affinity than the FS288 isoform, and drives local muscle mass increases without systemic hormonal disruption. Phase 1/2 gene therapy trials in Becker muscular dystrophy and inclusion body myositis have been conducted; the 2017 Mendell et al. Molecular Therapy paper demonstrated improved functional outcomes in sporadic inclusion body myositis — one of the few positive functional outcomes in the entire myostatin clinical space.[9]
First-generation anti-myostatin antibodies: the cautionary tale
MYO-029 (Wyeth/Pfizer) and similar compounds neutralising mature myostatin increased muscle mass in Phase 2 muscular dystrophy trials but produced no functional improvement. The key lesson: in dystrophic muscle, the underlying structural pathology — loss of dystrophin, repeated membrane fragility, fibrosis, fatty replacement — means that adding muscle mass does not restore function. Despite extensive research and promising preclinical results, clinical trials targeting myostatin inhibition in muscle dystrophies have failed to yield substantial improvements in muscle function, with challenges including drug specificity issues, serum myostatin concentration differences between animal models and humans, and the necessity of neural input for functional improvements.
Apitegromab (Scholar Rock): Phase 3 success
Apitegromab (SRK-015) is a fully human antibody that binds pro-GDF-8 and latent GDF-8 (the inactive precursor forms) without binding mature GDF-8, GDF-11, or activin A. By binding pro-myostatin and latent myostatin, apitegromab prevents tolloid metalloproteinase cleavage — keeping myostatin in its inactive form before release as active mature protein. This selectivity prevents the GDF-11 bone concern and reduces off-target effects.
Why does apitegromab work in SMA where earlier compounds failed in muscular dystrophies? In SMA, the primary lesion is motor neuron loss — the muscles themselves are structurally intact but denervated. Restoring muscle mass and strength in structurally intact muscles with functional neural connections allows functional benefit. In DMD/BMD, the muscle architecture is compromised at the sarcolemmal level. Scholar Rock filed a BLA in early 2025; manufacturing issues delayed approval; resubmission is expected in 2026.
Clinical Evidence Summary
| Inhibitor | Target | Indication | Outcome |
|---|---|---|---|
| MYO-029 (Wyeth) | Mature GDF-8 | Muscular dystrophy (Phase 2) | ❌ Increased mass; no functional benefit |
| Bimagrumab (Novartis) | ActRIIB (pan) | Inclusion body myositis (Phase 3) | ❌ Failed primary endpoint |
| Bimagrumab | ActRIIB (pan) | Obesity (Phase 2) | Fat loss + lean mass preservation — promising |
| Apitegromab (Scholar Rock) [8] | Pro/latent GDF-8 | Spinal muscular atrophy (Phase 3 SAPPHIRE) | ✅ Met primary endpoint (Oct 2024) |
| Apitegromab + tirzepatide | GDF-8 + GLP-1 | Obesity (Phase 2) | 54.9% more lean mass preserved vs. tirzepatide alone |
| Dual GDF-8 + ActA antibodies (Regeneron) [6] | GDF-8 + Activin A | Obesity + GLP-1 combination (NHP + Phase 1) | Lean mass gain + enhanced fat loss (Nat Commun May 2025) |
| AAV-FS344 gene therapy [9] | Multiple TGF-β | Inclusion body myositis (Phase 1/2) | Functional improvement (2017) |
“GDF-8 Peptide” in Community Use
Recombinant GDF-8 propeptide: Some vendors sell this as an injectable research peptide. It has preclinical evidence for muscle mass increases in rodents. No human pharmacokinetic, dose-finding, or safety data exists. The propeptide is a large protein (~28 kDa) with an entirely unknown human safety profile.
Follistatin-315 (FS344 product) administered as a protein: Systemic follistatin protein administration suppresses FSH and disrupts reproductive hormones — a real clinical concern confirmed in the biological literature. The gene therapy route was specifically developed to avoid this consequence. Injectable follistatin bypasses the tissue-local delivery that makes AAV-FS344 safe; systemic effects on FSH and GDF-11/bone are not modelled by the gene therapy data.
Peptide fragments derived from myostatin inhibitory sequences: Minimum inhibitory peptide sequences from the myostatin prodomain that block GDF-8 receptor binding have been identified in research. The step from “identified minimum inhibitory sequence” to “safe and effective therapeutic peptide in humans” involves enormous translational work that has not been done.
None of these uses have human clinical evidence.
Safety Considerations
Confirmed in clinical trials of related compounds: Muscle spasms (common with bimagrumab and other ActRIIB blockers); mouth ulcerations (consistent signal with ActRIIB inhibitors); upper respiratory tract infections; telangiectasia (activin A inhibition); GDF-11 inhibition → bone loss risk with non-selective agents and follistatin.
⚠️ Theoretical concerns for myostatin inhibition: Cardiac effects (myostatin is expressed in cardiac muscle; cardiac hypertrophy is theoretically possible with sustained inhibition); reproductive effects (systemic follistatin suppresses FSH; potential fertility impacts); cancer risk (myostatin has some anti-proliferative effects in certain tumour types; its inhibition could theoretically accelerate tumour growth in susceptible individuals — unquantified). Selective GDF-8 inhibitors (apitegromab) avoid GDF-11 inhibition and should not carry bone risk; pan-inhibitors and follistatin carry this concern.
Key Takeaways
- GDF-8 is the target, not the therapy. In the community, “GDF-8” means “something that inhibits myostatin.” This framing matters for understanding what evidence exists and what products are being discussed.
- The biology of myostatin is among the most compelling in muscle science. The “mighty mouse,” Belgian Blue cattle, and the human infant with loss-of-function mutation collectively make one of the clearest single-gene cases for muscle mass regulation in all of mammalian biology.[1][2]
- The clinical translation history is a cautionary tale about the gap between mass and function. First-generation anti-myostatin antibodies increased muscle mass without improving function in dystrophic patients. The muscle architecture of disease matters as much as the signal strength.
- ✅ Apitegromab’s Phase 3 SAPPHIRE success (October 2024) marks a genuine inflection point. By targeting pro/latent myostatin selectively, in patients with structurally intact muscles (SMA), meaningful functional improvement was demonstrated — the first Phase 3 success for a myostatin inhibitor.[8]
- The GLP-1 + myostatin inhibitor combination is the most exciting emerging application. Preserving lean mass during GLP-1-mediated weight loss is a real unmet need; the 2025 Regeneron data in non-human primates and the Scholar Rock obesity trial data suggest superior body composition outcomes are achievable.[6]
- ⚠️ Directly administered GDF-8 propeptide or follistatin proteins for human use are without clinical evidence. The preclinical data is real; the translational evidence to support human safety or dosing does not exist. Systemic follistatin carries specific reproductive and bone-related concerns that the AAV gene therapy approach was designed to circumvent.
References
Discovery
- McPherron AC, Lawler AM, Lee SJ. Regulation of skeletal muscle mass in mice by a new TGF-β superfamily member. Nature. 1997;387:83–90.
- McPherron AC, Lee SJ. Double muscling in cattle due to mutations in the myostatin gene. PNAS. 1997;94(23):12457–12461.
- Kambadur R, et al. Mutations in myostatin (GDF8) in double-muscled Belgian Blue and Piedmontese cattle. Genome Research. 1997;7(9):910–916.
Mechanism
- Lee SJ. Targeting the myostatin signalling pathway to treat muscle loss and metabolic dysfunction. PMID 33938454. 2021.
Clinical Evidence — GLP-1 Combination
- Gonzalez Trotter D, et al. GDF8 and activin A are the key negative regulators of muscle mass in postmenopausal females: a randomised Phase I trial. Nature Communications. 2025;16:4376.
- Gonzalez Trotter D, et al. GDF8 and activin A blockade protects against GLP-1-induced muscle loss while enhancing fat loss in obese male mice and non-human primates. Nature Communications. 2025;16:4377.
Clinical Evidence — Apitegromab SMA
- Myostatin inhibitors: panacea or predicament for musculoskeletal disorders? PMC7571243. 2020.
- Scholar Rock SAPPHIRE Phase 3 trial (apitegromab in spinal muscular atrophy). Primary endpoint met October 7, 2024.
Follistatin and Therapeutic Inhibitors
- Mendell JR et al. Follistatin gene therapy for sporadic inclusion body myositis improves functional outcomes. Molecular Therapy. 2017;25(4):870–879.
- Therapeutic applications and challenges in myostatin inhibition for enhanced skeletal muscle mass and functions. PMC11842502. 2025.
- Emerging role of myostatin inhibitors in the management of GLP-1-associated sarcopenia and metabolic disorders. PMC12719006. 2025.
Key Investigators
- Se-Jin Lee, MD, PhD — Johns Hopkins University (now Jackson Laboratories); co-discoverer of myostatin (1997); led the foundational knockout mouse work; principal investigator on the 2025 NHP GLP-1 combination study; the central figure in myostatin biology for nearly 30 years.
- Alexandra McPherron, PhD — National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK); co-discoverer of myostatin.
- Jerry R. Mendell, MD — Nationwide Children’s Hospital, Columbus; pioneer of AAV gene therapy in neuromuscular disease including AAV-FS344 follistatin gene therapy trials.
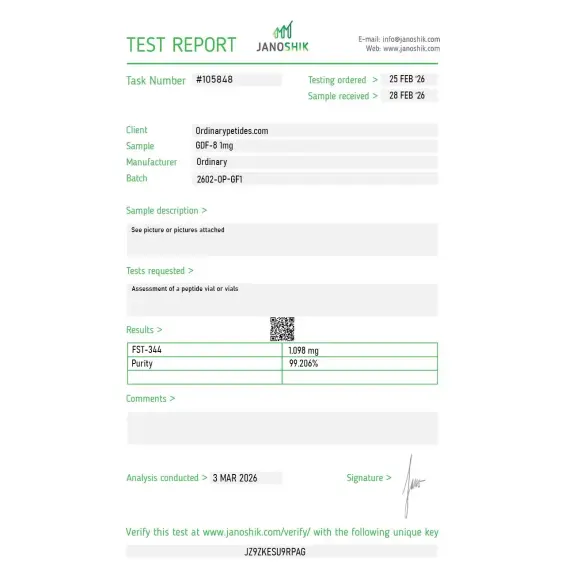
Certificate of Analysis
An independent test report is available for GDF-8 1mg. This report provides batch-level documentation and analytical verification information for research reference.

Based on 1 reviews
5.0
We use it as the positive-control ligand when screening compounds for activin/myostatin pathway interference — you need authentic functional GDF-8 to confirm that test inhibitors actually block what they're supposed to block, and any inactive control material would invalidate the whole screen. Material gave reproducible SMAD2/3 phosphorylation in our HEK293 reporter line, which is what makes it usable as the standard.
GDF-8, also known as myostatin, is a naturally occurring protein and member of the transforming growth factor-beta (TGF-β) superfamily. It is produced primarily in skeletal muscle and acts as the body's built-in brake on muscle growth — its sole biological purpose is to limit how much muscle the body can develop. It is 100% conserved across humans, mice, rats, pigs, and chickens, which underlines how fundamental it is to mammalian biology.
GDF-8 binds to activin type IIB receptors on muscle cells and activates SMAD2/3 signaling pathways, which suppress muscle fiber growth, inhibit satellite cell activity, promote muscle fibrosis, and block osteogenic differentiation. In simple terms it tells cells to stop growing, stop dividing, and in some cases break down existing tissue. Animals and humans with naturally non-functional GDF-8 develop dramatically increased muscle mass — a phenomenon observed in double-muscled cattle breeds and in rare human cases.
The therapeutic interest is not in administering GDF-8 itself, but in inhibiting it. Blocking GDF-8 activity is one of the most researched strategies for treating muscle-wasting diseases such as muscular dystrophy, sarcopenia, cancer cachexia, and age-related muscle loss. Compounds like follistatin (FST-344), myostatin propeptide-Fc, and monoclonal antibodies such as trevogrumab are all designed to neutralize GDF-8 and thereby allow muscle growth to proceed unchecked.
Research spans muscular dystrophy, sarcopenia in aging, cancer cachexia, ACL injury recovery, posttraumatic osteoarthritis, spaceflight-related muscle loss, and obesity-linked metabolic dysfunction. Studies in mice with GDF-8 deficiency also show decreased body fat and increased bone density across limbs, spine, and jaw, suggesting broader metabolic and skeletal implications beyond muscle alone.
No GDF-8 inhibitor is yet broadly FDA-approved for widespread clinical use, though several are in active clinical trials. Monoclonal antibodies targeting GDF-8 have reached Phase II and Phase III trials for muscular dystrophy and sarcopenia. GDF-8 as a standalone research reagent is not for human therapeutic use — it is used in laboratory settings to study signaling pathways and to validate inhibitor compounds.
The main concern with uncontrolled myostatin inhibition is that muscle growth can outpace the structural capacity of tendons, ligaments, and joints — leading to tendon rupture and joint damage. There is also evidence that myostatin inhibitors may deplete muscle stem cells over the long term, which could paradoxically worsen conditions like muscular dystrophy with extended use. Metabolic changes and reproductive hormone disruption are also possible depending on the inhibitor used.
Anyone without direct medical supervision, those with active joint or tendon injuries, individuals with hormonal disorders, pregnant women, and people with a history of cancer should avoid any GDF-8 modulating compounds. Because most available GDF-8 inhibitors outside of clinical trials are unregulated research compounds, their purity and safety cannot be guaranteed.





