

LGD-4033
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
LGD-4033 (Ligandrol): A Selective Androgen Receptor Modulator at the Crossroads of Anabolic Research, Tissue-Selective Pharmacology, and Musculoskeletal Biology
LGD-4033, also known as Ligandrol or VK-5211, is a synthetic nonsteroidal small molecule best known in the field of anabolic research, where it has been studied as a selective androgen receptor modulator (SARM) with high affinity and selectivity for the androgen receptor (AR), and linked to the biology of muscle protein synthesis. In the research context, the main interest in this compound grew out of studies reporting increased lean body mass, enhanced nitrogen retention, and improved bone parameters without the broad off-target activity characteristic of classical anabolic steroids. That sounds dramatic — and that is precisely why it attracts so much attention.
Published reports have also discussed its relationship with GH/IGF-1 axis stimulation, muscle recovery, and lean mass preservation during caloric deficit, while preclinical and early clinical data have connected it to a broader tissue-selective anabolic framework, including investigations in muscle wasting and osteoporosis models. Still, a sober filter is essential here: a compelling selectivity story is not yet a free-of-consequences anabolic in a vial — LGD-4033 still suppresses endogenous testosterone in a dose-dependent way and appears on the WADA prohibited list. If only biology were that cooperative.
What makes LGD-4033 genuinely interesting is that it sits at the crossroads of muscle growth hypotheses, androgen receptor pharmacology, and the newer tradition of nonsteroidal SARMs — a class designed to dissociate anabolic activity in muscle and bone from androgenic effects in other tissues. For readers who care not just about bold promises but about the actual scientific grounds for interest, this is exactly the kind of compound worth examining carefully — and without illusions.
LGD-4033 (Ligandrol): A Scientific Review of the Selective Androgen Receptor Modulator
Based on peer-reviewed literature — see References. Last updated: May 2026.
The Short Version
LGD-4033 (also known as ligandrol, anabolicum, VK5211) is one of the most popular compounds in the consumer "SARM" market. It has been the subject of a properly conducted Phase 1 trial published in the Journal of Gerontology in 2013, advanced into a Phase 2 program for hip fracture recovery by Viking Therapeutics (under the code name VK5211), and continues to appear in pharmacology literature including a notable 2025 critical appraisal in Frontiers in Endocrinology and multiple published case reports of drug-induced liver injury.
The pharmacological premise is genuinely interesting. SARMs (Selective Androgen Receptor Modulators) were designed to solve a specific problem: testosterone and anabolic steroids produce real anabolic effects on muscle and bone, but at the cost of widespread off-target effects on prostate, cardiovascular system, lipid profile, fertility, and other androgen-sensitive tissues. SARMs aim to retain the anabolic benefits while eliminating or reducing the side effects through tissue-selective receptor activation. The theory is elegant. The clinical translation has been substantially more complicated.
The Basaria et al. 2013 study — the only published placebo-controlled human trial of LGD-4033 — established that at doses up to 1 mg/day over 21 days, the compound was reasonably well-tolerated, produced dose-dependent increases in lean body mass, and suppressed testosterone, SHBG, and HDL cholesterol.[1] These results validated the basic premise: at low doses, over short periods, in healthy young men under careful monitoring, LGD-4033 produces measurable anabolic effects without catastrophic side effects.
That isn't the situation in which LGD-4033 is typically used.
The compound went through legitimate pharmaceutical development. It just doesn't behave the same way in the consumer market as it did in the trials.
| At a glance | |
|---|---|
| Generic name | LGD-4033 |
| Common names | Ligandrol, anabolicum |
| Development code | VK5211 (Viking Therapeutics) |
| Chemical class | Non-steroidal selective androgen receptor modulator (SARM) |
| Molecular formula | C₁₄H₁₂F₆N₂O |
| Molecular weight | 338.2 Da |
| Mechanism | Selective agonist of androgen receptor (AR); tissue-selective |
| Originator | Ligand Pharmaceuticals (early 2000s) |
| Subsequent developer | Viking Therapeutics (2014–present; as VK5211) |
| Foundational human trial | Basaria et al., J Gerontol A, 2013 |
| Phase 2 indication | Rehabilitation after hip fracture |
| Half-life (humans) | ~24-36 hours |
| Oral bioavailability | High (active orally) |
| FDA status | ❌ Not approved. Public warnings against use in bodybuilding products (2017, 2024) |
| EMA status | ❌ Not approved |
| WADA status | ⚠️ Prohibited — Class S1.2 (anabolic agents, "other anabolic agents") — at all times |
| Documented serious AE | Drug-induced liver injury (multiple case reports); hormonal suppression; lipid changes |
What SARMs Are and Aren't
Before discussing LGD-4033 specifically, it helps to understand the SARM concept clearly, because the marketing framing often differs substantially from the pharmacological reality.
The SARM concept
The androgen receptor (AR) is expressed in many tissues: skeletal muscle, bone, prostate, sebaceous glands, hair follicles, liver, brain, and others. Testosterone and dihydrotestosterone activate AR in all of these tissues simultaneously, which is why steroid use produces both desired effects (muscle gain, strength) and undesired effects (prostate enlargement, acne, hair changes, cardiovascular impact, sometimes infertility, mood changes). For the broader hormonal axis context, see the Endocrine Research category.
SARMs are designed to activate AR selectively — turning on the anabolic effects in muscle and bone while minimizing activation in prostate and other tissues. The mechanism varies by compound: some SARMs are designed to recruit different sets of coactivators in different tissues, some have different tissue distribution, some have agonist activity in some tissues and antagonist activity in others.
The most successful SARM developed so far is enobosarm (GTx-024, ostarine), which has completed multiple Phase 3 trials and is being pursued for breast cancer and other indications. LGD-4033 sits in the next tier — successful Phase 1, partial Phase 2 development, no approved indication anywhere.
What SARMs aren't
A few persistent misconceptions worth flagging upfront:
- SARMs are not "natural" alternatives to steroids. They're synthetic drugs that activate androgen receptors. The activation mechanism differs, but the receptor is the same.
- SARMs are not approved supplements. The FDA has explicitly stated that SARMs are unapproved drugs and that their inclusion in dietary supplements is illegal.
- SARMs are not free of androgenic effects. They're more selective than steroids, not selective in an absolute sense. Some tissues still respond to AR activation in ways that look like classical androgen exposure.
- SARMs do not protect against the hormonal suppression of natural testosterone. Activating AR with an exogenous ligand suppresses LH and FSH (and therefore endogenous testosterone production) just as steroids do.
Origin and Development
The Ligand Pharmaceuticals years
LGD-4033 emerged from Ligand Pharmaceuticals' SARM discovery program in the early 2000s. The compound was a structure-activity-relationship optimization target arising from screening of non-steroidal AR modulators. The "LGD" prefix refers to Ligand; the "4033" is the program identifier. Ligand had a history of working on nuclear receptor pharmacology and selected LGD-4033 as their lead SARM candidate based on its in vitro receptor selectivity profile and in vivo anabolic efficacy in animal models.
The Phase 1 single ascending dose and multiple ascending dose studies established safety at doses up to 22 mg single-dose and up to 1.0 mg/day for 21 days. The Basaria et al. 2013 paper in Journal of Gerontology reported the multiple ascending dose study — this remains the only published placebo-controlled human trial of LGD-4033.[1]
The Viking Therapeutics handoff
In 2014, Ligand transferred LGD-4033 (along with several other compounds) to Viking Therapeutics, a newly formed biotech specifically built around the Ligand-licensed pipeline. Viking renamed LGD-4033 to VK5211 and prioritized development for rehabilitation after hip fracture — a meaningful unmet medical need where lean mass preservation and bone density during recovery are clinically important. For the broader landscape of compounds investigated in musculoskeletal contexts, see the Musculoskeletal Research category.
Viking's Phase 2 hip fracture trial (NCT02578095) was reported in 2018 with positive results: VK5211 produced dose-dependent increases in lean body mass over 12 weeks compared to placebo in patients recovering from hip fracture surgery. Different doses (0.5 mg, 1 mg, 2 mg daily) were tested, and the higher doses produced greater lean mass gains.
As of 2026, Viking's broader pipeline has shifted heavily toward their GLP-1/GIP and other metabolic programs (VK2735, etc.), and VK5211 has not progressed to a registration-enabling Phase 3 program for the hip fracture indication. The compound remains in development limbo — clinically validated for early indications, not advanced toward approval.
The consumer market
In parallel with the legitimate pharmaceutical development, LGD-4033 was discovered by the bodybuilding community in the mid-2010s and rapidly became one of the most popular "research chemical" SARMs. It's sold by hundreds of online vendors, frequently mislabeled in supplements, and appears in adulterated products that the FDA has repeatedly warned consumers about.
The doses used in this consumer context (typically 5-20 mg daily, sometimes much higher) are 5-20× higher than the highest dose in the published Phase 1 trial. The published clinical literature provides essentially no direct safety data for this exposure range.
How It Works
Binding and activation
LGD-4033 is a non-steroidal small molecule that binds the androgen receptor with high affinity (Ki ~1 nM). Unlike testosterone, which is a steroid that diffuses through cell membranes to reach intracellular AR, LGD-4033 has a different binding pose in the receptor and produces different coactivator recruitment profiles.
After AR activation, the receptor translocates to the nucleus, dimerizes, and binds androgen response elements (AREs) in DNA, modulating transcription of androgen-target genes. The downstream effects in muscle tissue include increased protein synthesis, decreased protein degradation, and net anabolic phenotype.
Tissue selectivity (in theory)
The pharmacology argument for LGD-4033's selectivity is based on differential coactivator recruitment between tissues. In muscle and bone, the receptor-LGD-4033 complex efficiently recruits the coactivators needed for anabolic gene transcription. In prostate, the same complex recruits fewer of the coactivators needed for prostate cell proliferation. The net result is anabolic activity in muscle/bone with reduced effect on prostate.
This selectivity has been demonstrated in animal models (the foundational paper showed muscle-to-prostate selectivity ratios many times higher than testosterone) and is supported by the Phase 1 trial's observation that PSA didn't change at the doses tested.[1]
How well this selectivity holds at higher doses is less clear. Receptor selectivity is generally a continuum, not a binary feature, and at high enough exposure most selective compounds become less selective.
What activation produces in humans (from Phase 1)
The Basaria 2013 trial reported, at 1 mg daily over 21 days:
| Parameter | Effect |
|---|---|
| Lean body mass | Dose-dependent increase |
| Muscle strength (1RM) | Trend toward increase (underpowered) |
| Stair-climbing power | Trend toward increase (underpowered) |
| Total testosterone | Decreased |
| Free testosterone | Decreased |
| Sex hormone binding globulin (SHBG) | Decreased |
| LH and FSH | Decreased (HPG axis suppression) |
| HDL cholesterol | Decreased |
| Total cholesterol | Decreased slightly |
| Liver function tests (ALT, AST) | No significant change |
| PSA | No significant change |
| Hematocrit | No clinically significant change |
| ECG | No clinically significant change |
The hormonal suppression normalized over the 5-week observation period after drug discontinuation. The lipid changes also reverted after stopping.[1]
This is what 1 mg/day for 21 days does in healthy young men under monitoring. The marketing extrapolation to "10 mg/day for 8-12 weeks in untrained or trained adults" requires considerable assumption.
Human Evidence
The corpus of human evidence on LGD-4033 has a distinctive shape: one well-conducted small Phase 1 trial, a moderately reported Phase 2 trial in a specific clinical population, multiple case reports of severe adverse events from real-world use, and a 2025 critical appraisal published in Frontiers in Endocrinology.
Basaria et al. 2013 (the cornerstone study)
The most-cited human trial. Phase 1 randomized, double-blind, placebo-controlled ascending dose study. 76 healthy young men randomized to placebo or LGD-4033 at 0.1, 0.3, or 1.0 mg daily for 21 days, followed by a 5-week observation period.[1]
Findings, summarized above. Three things worth noting that get less attention:
- The functional measures (strength, stair-climbing) showed only trends, not significant differences. The study was, by the authors' own statement, not powered to detect functional improvements.
- The hormonal suppression was substantial. Total testosterone fell, free testosterone fell, SHBG fell, LH and FSH fell — even at 1 mg daily, well below typical "user" doses.
- HDL cholesterol dropped meaningfully. This is consistent with AR activation effects on hepatic lipid metabolism and is a documented feature of essentially all AR ligands (steroids and SARMs alike).
The trial showed what LGD-4033 does at low doses, short term. It did not address what happens at the doses and durations of typical consumer use.
Viking Therapeutics Phase 2 (VK5211 in hip fracture)
A Phase 2 randomized, double-blind, placebo-controlled trial in patients recovering from hip fracture. 108 patients across multiple sites. Three VK5211 doses (0.5, 1.0, 2.0 mg daily) versus placebo for 12 weeks.
Results: VK5211 produced dose-dependent increases in lean body mass at all tested doses. The compound was generally well-tolerated in the patient population. Detailed peer-reviewed publication of the Phase 2 results in major Western journals has been less extensive than the Phase 1 trial's coverage; most of the public information comes from Viking's corporate disclosures and conference presentations.
Drug-induced liver injury case reports
This is the part of the literature that has expanded most since 2020 — and it's the part that the consumer-facing marketing carefully ignores.
Barbara et al. 2020 (ACG Case Reports Journal) — A 32-year-old man developed severe cholestatic drug-induced liver injury after taking 10 mg of LGD-4033 daily for 2 weeks. Total bilirubin reached very elevated levels, alkaline phosphatase increased dramatically, and liver biopsy showed cholestatic hepatitis with mild portal, periportal, and perisinusoidal fibrosis. Other causes of liver injury were ruled out. The patient improved after discontinuation.[2]
A 2024 case report (PMC11485217) — A 52-year-old man developed DILI with pruritic jaundice and significant weight loss after three months of high-dose LGD-4033 use. Liver enzymes were severely elevated. Clinical course consistent with SARM-induced hepatotoxicity.[6]
Other case reports have appeared in Cureus, Journal of Clinical and Translational Hepatology, and other journals describing similar patterns: previously healthy individuals developing severe cholestatic or mixed-pattern liver injury after weeks to months of LGD-4033 use at consumer-typical doses (5-20 mg/day).
The pattern in these cases is striking and clinically important:
- Doses are 10-100× higher than the Phase 1 trial dose
- Duration is weeks to months rather than 21 days
- The liver injury is severe enough to cause clinical symptoms (jaundice, pruritus, weight loss)
- Improvement on discontinuation supports causation
- Some cases have shown bridging fibrosis on biopsy, indicating real liver damage rather than transient enzyme elevations
The Basaria 2013 trial's reassuring "no significant changes in liver function tests" was at 1 mg/day for 21 days. It does not apply to the consumer dosing range.
Bond et al. 2025 (Frontiers in Endocrinology)
A 2025 critical appraisal of SARMs as a class, covering LGD-4033 and other compounds in detail. The general conclusion: SARMs have meaningful effects on muscle mass and strength, but the safety profile in real-world use is concerning, with documented hepatotoxicity, cardiovascular effects, and HPG axis suppression that may not always recover spontaneously. The authors emphasize that "SARMs should not be considered as alternatives to androgenic anabolic steroids" given the side effect profile.[7]
This is a meaningful framing shift from the early-2010s optimism about SARMs as a "safer alternative." The current academic position is more cautious.
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) | ❌ Not approved. Public warning issued 2017 against SARMs in bodybuilding products; reiterated 2024. Multiple seizure actions against vendors. |
| EMA (Europe) | ❌ Not approved |
| WADA | ⚠️ Prohibited at all times — Class S1.2 (anabolic agents, "other anabolic agents") |
| Compounding pharmacies | Not approved for compounding |
| Dietary supplement legal status | ❌ Illegal — FDA position is that SARMs are unapproved drugs, not dietary ingredients |
| Sport testing | Routine LC-MS/MS detection; hair testing also available |
The FDA's position deserves particular attention. The 2017 warning specifically called out the inclusion of SARMs (including LGD-4033) in products marketed as bodybuilding supplements, citing both the unapproved drug status and the risk of serious adverse events. The FDA has since taken multiple enforcement actions against vendors, including warning letters and product seizures.
This doesn't stop the grey market, but it does mean that any vendor selling LGD-4033 for human consumption is operating in violation of FDA regulations, with no quality control requirements and no liability framework.
The WADA classification under S1.2 means LGD-4033 use is a doping violation for any athlete subject to anti-doping testing — Olympic, professional, college, even some recreational competitions. Detection methods are well-established and sensitive; trace exposure (including from contaminated supplements) has produced positive tests in athletes who claim no knowledge of intentional use.
Safety: What's Documented at Different Exposure Levels
This is where LGD-4033 requires especially careful framing, because the safety profile differs dramatically between the studied dose range and the real-world use range.
At the studied range (≤1 mg/day, 21 days, monitored)
From Basaria 2013 and supporting trials:
- Hormonal suppression: documented, reversible after discontinuation
- Lipid changes: HDL decrease, reversible
- Liver enzymes: no significant change
- PSA: no significant change
- Cardiovascular markers: no significant short-term change
- Overall tolerability: acceptable
At the consumer range (5-20+ mg/day, weeks to months, unmonitored)
This is the range where most LGD-4033 use actually occurs, and where the published case reports come from.
Hepatotoxicity (documented)
Multiple published case reports of severe DILI:
- Cholestatic pattern most common, but mixed pattern also reported
- Onset typically 2 weeks to 3 months after starting
- Severity ranges from transaminase elevations to clinical jaundice
- Some cases show bridging fibrosis on biopsy
- Improvement on discontinuation
- The mechanism may involve idiosyncratic drug reactions and/or dose-dependent toxicity
This is the single most important safety signal that's emerged from real-world use. It was not predicted by the Phase 1 trial.
Hormonal suppression (documented)
Even at low doses, LGD-4033 suppresses LH, FSH, and endogenous testosterone production. At higher doses and longer durations, this suppression is more severe. Recovery is variable:
- Most users see hormonal normalization within weeks to months after stopping
- Some users develop persistent hypogonadism requiring medical intervention
- Co-administration of "post-cycle therapy" (SERMs like clomiphene or tamoxifen) is common in user communities but has its own safety considerations and isn't formally validated. HPG-axis recovery is also studied in the context of peptide compounds like gonadorelin acetate and kisspeptin-10, which target upstream regulation of the same axis.
Lipid profile changes (documented)
HDL cholesterol decreases consistently. At higher doses, total cholesterol and LDL may also shift. The cardiovascular implications of prolonged HDL suppression are well-established from the broader androgen-steroid literature.
Cardiovascular concerns (suggested)
Multiple sources, including Bond et al. 2025, raise cardiovascular safety as a concern with SARMs as a class. The mechanisms include lipid effects, possible direct effects on cardiac tissue, and effects on hematocrit at higher doses. Long-term cardiovascular outcomes data don't exist.
Psychiatric effects (reported)
Mood changes, irritability, and other psychiatric symptoms have been reported. Mechanism is plausibly related to androgen receptor activation in CNS but not well-characterized.
Other reported adverse effects
- Sleep disturbance
- Mild hypertension in some users
- Hair changes (less than with steroids, but present)
- Possible effects on fertility (related to HPG axis suppression)
Vendor product quality
A separate but critical safety consideration. Independent testing of "LGD-4033" products from research-chemical and supplement vendors has repeatedly shown:
- Variable LGD-4033 content (often much higher or lower than labeled)
- Substitution with other SARMs (especially RAD-140, which is more potent and more hepatotoxic)
- Contamination with other compounds (other SARMs, prohormones)
- In some cases, complete absence of any active SARM
This means that even setting aside the question of LGD-4033's own safety, the actual product consumers receive may contain something different and worse. For tested athletes especially, contamination has produced positive doping tests with serious consequences.
| Safety area | Studied range (≤1 mg/day, 21 days) | Consumer range (5-20+ mg/day, months) |
|---|---|---|
| Hepatotoxicity | ✓ No signal | ⚠️ Multiple severe DILI cases reported |
| Hormonal suppression | ⚠️ Documented, reversible | ⚠️ More severe, recovery variable |
| Lipid changes | ⚠️ HDL drop, reversible | ⚠️ More substantial |
| Cardiovascular effects | ✓ No short-term signal | ⚠️ Concerning class-level signals |
| Psychiatric effects | ✓ Not reported | ⚠️ Mood changes reported |
| Fertility effects | ⚠️ Theoretical | ⚠️ Real concern via HPG suppression |
| Vendor quality | N/A (pharmaceutical grade) | ⚠️ Highly variable |
Common Misconceptions
"SARMs are safer alternatives to steroids."
This is the most persistent and most consequential misconception. SARMs are more selective than steroids — meaning they activate AR more in muscle/bone than in prostate or other tissues. They are not categorically safer. The 2024 case report explicitly notes that "the misconception that SARMs are safer alternatives to anabolic steroids" is what drives much of the consumer use, despite documented hepatotoxicity, cardiovascular complications, endocrine disturbances, and psychiatric symptoms.[6]
"SARMs don't suppress your natural testosterone."
They do. Activating AR with any exogenous ligand suppresses LH and FSH via negative feedback, which suppresses endogenous testosterone production. The Basaria 2013 trial clearly documented this even at the lowest dose tested. The user-community myth that "SARMs don't shut you down" doesn't survive contact with the actual clinical data.
"LGD-4033 doesn't affect the liver."
The Phase 1 trial at 1 mg/day for 21 days showed no significant liver enzyme changes. Multiple published case reports at consumer doses (10-15 mg/day for weeks to months) show severe drug-induced liver injury including cholestatic hepatitis and fibrosis. Both can be true: low-dose short-term LGD-4033 doesn't significantly affect liver enzymes, while high-dose long-term LGD-4033 can cause severe DILI.
"It's basically approved — it's just in Phase 2 trials."
Phase 2 trials are early clinical development, not regulatory approval. The Phase 2 hip fracture program by Viking Therapeutics has not been advanced to Phase 3. The compound's clinical development has effectively stalled, and there is no announced path to FDA approval for any indication as of 2026.
"SARMs are legal because they're in supplements."
The FDA position is the opposite: SARMs are unapproved drugs, and their inclusion in products marketed as dietary supplements is illegal. The continued availability of SARM products reflects regulatory enforcement limitations, not legal status. Multiple FDA warning letters and seizure actions have targeted SARM vendors.
"PCT (post-cycle therapy) fully recovers your hormones after SARMs."
PCT protocols using SERMs (clomiphene, tamoxifen) and other agents are common in user communities. They can help, but recovery is variable. Some users develop persistent hypogonadism that doesn't fully resolve with PCT. PCT itself isn't a clinical protocol — it's a community practice based on bodybuilding tradition, not validated clinical research.
"Liver injury from SARMs only happens at extreme doses."
The published case reports include users taking 10 mg/day — which is a common consumer dose, often advertised as "moderate" by vendors. The dose at which DILI becomes likely isn't well-characterized, and individual susceptibility appears to vary substantially.
Frequently Asked Questions
How does LGD-4033 compare to anabolic steroids in terms of muscle gain?
Less effective on muscle mass per unit time at typical doses, but the comparison varies substantially with dose, individual response, training status, and exposure duration. The Basaria 2013 trial showed lean body mass gains of approximately 1-1.5 kg over 21 days at 1 mg/day — modest but real. Higher consumer doses produce larger gains, but the safety profile deteriorates rapidly with increasing exposure.
Why is the Phase 2 hip fracture trial program stalled?
Viking Therapeutics has shifted its strategic focus toward its metabolic programs (GLP-1/GIP, others) where commercial opportunities are larger. The hip fracture indication, while medically meaningful, represents a relatively niche commercial market that may not justify the Phase 3 development cost. As of 2026, there's no announced timeline for further LGD-4033 development.
Will SARMs ever be approved?
Enobosarm (ostarine) has come closest, with multiple Phase 3 trials. Whether any SARM reaches FDA approval depends on demonstrating clinical benefit that justifies the safety profile in well-defined patient populations. For LGD-4033 specifically, the clinical development program has not advanced toward approval and the regulatory pathway is unclear.
Is the liver injury risk universal?
It appears to be idiosyncratic with a dose-dependent component. Most users don't develop clinical DILI. The published case reports represent a minority of users but represent serious events when they occur. Individual genetic factors (hepatic transporter polymorphisms among others) may predispose certain users.
Can the hormonal suppression be permanent?
In most cases, suppression resolves within weeks to months of discontinuation. Some users develop persistent hypogonadism. The risk of persistent suppression appears to increase with higher doses, longer use, and possibly with younger age at first use. Recovery is variable enough that individual outcomes can't be predicted.
How does LGD-4033 compare to GH-axis compounds like MK-677 or peptide secretagogues?
These are pharmacologically unrelated. LGD-4033 works through the androgen receptor; MK-677 and peptide GH secretagogues like ipamorelin and HGH work through the growth hormone / IGF-1 axis. The compounds are frequently stacked in bodybuilding contexts, but the mechanisms, side effect profiles, and clinical evidence bases differ substantially. Stacking unrelated mechanisms also stacks unrelated risks.
Why is it so popular if these risks are documented?
A combination of factors: the marketing framing as "safer than steroids" continues despite contradicting evidence; the case reports of severe adverse events are buried in clinical journals rather than appearing in social media or fitness content; many users don't experience overt symptoms even if they're experiencing subclinical hormonal or hepatic changes; and the visible short-term effects (muscle gain) are real, while the longer-term consequences are often invisible.
Key Takeaways
- LGD-4033 (ligandrol) is a non-steroidal selective androgen receptor modulator developed by Ligand Pharmaceuticals, with a properly conducted Phase 1 trial published in 2013 (Basaria et al., J Gerontol A) showing dose-dependent lean body mass gain at doses ≤1 mg/day over 21 days in healthy young men.[1]
- Viking Therapeutics advanced LGD-4033 as VK5211 into a Phase 2 trial for hip fracture rehabilitation, with positive top-line results. The program has not progressed to Phase 3, and no clear path to FDA approval exists as of 2026.
- ⚠️ Multiple published case reports document severe drug-induced liver injury (DILI) from LGD-4033 use at consumer doses (5-15 mg/day for weeks to months). This is the most consequential real-world safety signal and was not predicted by the Phase 1 trial at lower doses.[2][6]
- ⚠️ Even at the lowest tested dose (0.1 mg/day), LGD-4033 produces hormonal suppression (decreased total and free testosterone, LH, FSH, SHBG) and HDL cholesterol decrease. These effects normalize after discontinuation in most cases but recovery is variable at higher doses.
- The "SARMs are safer alternatives to steroids" framing that drives much consumer use is increasingly contradicted by the published case literature. The 2025 Frontiers in Endocrinology critical appraisal explicitly states SARMs should not be considered as alternatives to anabolic steroids.[7]
- Regulatorily, LGD-4033 is not approved anywhere. The FDA has issued public warnings (2017, 2024) against SARMs in bodybuilding products and taken enforcement actions against vendors. Inclusion in dietary supplements is illegal under FDA position.
- ⚠️ WADA-prohibited at all times in sport under class S1.2. Detection methods are well-established. Contamination of supplements with SARMs has produced positive doping tests in athletes who deny intentional use.
- ⚠️ Consumer supply chain quality is highly variable. Independent testing of vendor products shows inconsistent LGD-4033 content, substitution with more potent SARMs (RAD-140), and contamination. The compound consumers receive may not match the label.
- The dose disparity matters substantially. The Phase 1 trial used ≤1 mg/day for 21 days. Consumer doses are 5-20 mg/day for 8-16 weeks. The published safety data does not extrapolate cleanly across this range, as the DILI case reports demonstrate.
- Honest framing: LGD-4033 has more substantial human clinical data than most compounds in this review series. The data show real anabolic effects, real hormonal suppression, real lipid changes, and — in real-world consumer use — real risk of severe liver injury. Decisions about use should weigh these documented effects, not the marketing narrative that contradicts them.
Related Compounds
For peptide-based approaches studied in muscle and bone contexts, see the Musculoskeletal Research category. The growth hormone / IGF-1 axis is frequently stacked with SARMs in bodybuilding contexts — relevant compounds in that space include ipamorelin (selective GH secretagogue) and HGH itself. For HPG-axis recovery research after exogenous hormone suppression, peptides like gonadorelin acetate and kisspeptin-10 are relevant. For the broader endocrine landscape, see Endocrine Research.
References
Pivotal clinical trial
- Basaria S, Collins L, Dillon EL, Orwoll K, Storer TW, Miciek R, Ulloor J, Zhang A, Eder R, Zientek H, Gordon G, Kazmi S, Sheffield-Moore M, Bhasin S. The Safety, Pharmacokinetics, and Effects of LGD-4033, a Novel Nonsteroidal Oral, Selective Androgen Receptor Modulator, in Healthy Young Men. J Gerontol A Biol Sci Med Sci. 2013;68(1):87-95. doi: 10.1093/gerona/gls078. PMID: 22459616
Documented adverse events
- Barbara M, Dhingra S, Mindikoglu AL. Ligandrol (LGD-4033)-Induced Liver Injury. ACG Case Rep J. 2020;7(6):e00370. doi: 10.14309/crj.0000000000000370. PMC7304490
- LGD-4033 and a Case of Drug-Induced Liver Injury: Exploring the Clinical Implications of Off-Label Selective Androgen Receptor Modulator Use in Healthy Adults. Cureus. 2024. PMC11485217
Reviews and critical appraisals
- Bond P, Smit DL, Verdegaal T, de Ronde W. Selective androgen receptor modulators: a critical appraisal. Front Endocrinol. 2025;16:1634799.
- Wen J, Syed B, Leapart J, et al. Selective androgen receptor modulators (SARMs) effects on physical performance: a systematic review. Clin Endocrinol. 2025;102(1):3-27.
- Narayanan R, Coss CC, Dalton JT. Development of selective androgen receptor modulators (SARMs). Mol Cell Endocrinol. 2018;465:134-142.
Animal pharmacology and additional human data
- Vasilev V, et al. Ligandrol lowers endurance and negatively affects lipid and hormonal profile of male rats. PMC. 2025.
- Cardaci TD, Machek SB, Wilburn DT, et al. LGD-4033 and MK-677 use impacts body composition, circulating biomarkers, and skeletal muscle androgenic hormone and receptor content: a case report.
Comparative SARM context
- Dalton JT, Barnette KG, Bohl CE, Hancock ML, Rodriguez D, Dodson ST, Morton RA, Steiner MS. The selective androgen receptor modulator GTx-024 (enobosarm) improves lean body mass and physical function in healthy elderly men and postmenopausal women. J Cachexia Sarcopenia Muscle. 2011.
Regulatory
- FDA Statement on SARMs in bodybuilding products (2017; reiterated 2024). Warning letters and enforcement actions.
- WADA Prohibited List 2026 — Class S1.2 anabolic agents.
Key investigators and developers
- Shehzad Basaria, MD — Brigham and Women's Hospital / Harvard Medical School (formerly Boston University). Co-principal investigator of the LGD-4033 Phase 1 study; long-time researcher in androgen and SARM pharmacology.
- Shalender Bhasin, MD — Brigham and Women's Hospital / Harvard. Senior author on the Basaria 2013 paper; foundational figure in androgen clinical research.
- Ligand Pharmaceuticals — Original developer of LGD-4033.
- Viking Therapeutics — Current rights holder; developed VK5211 (LGD-4033) through Phase 2 for hip fracture indication.
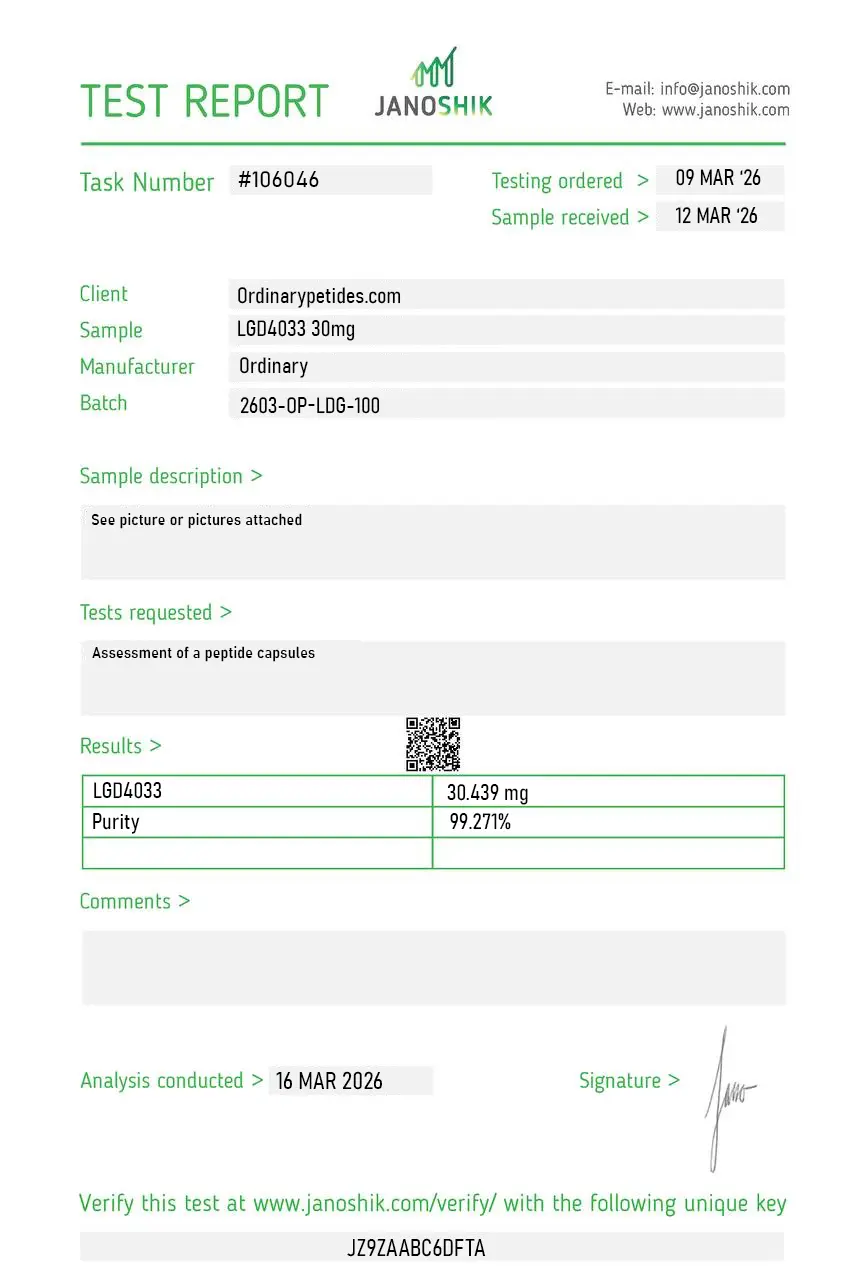
Certificate of Analysis
An independent test report is available for LGD-4033 30mg. This report provides batch-level documentation and analytical verification information for research reference.
LGD-4033 — also known as Ligandrol, VK5211, and L-163,191 — is a third-generation, non-steroidal, orally bioavailable selective androgen receptor modulator (SARM) first described in 2010. It was originally developed by Ligand Pharmaceuticals, Inc. as a potential treatment for muscle wasting, sarcopenia, and osteoporosis. In 2014, Viking Therapeutics licensed the developmental rights from Ligand Pharmaceuticals, renaming the compound VK5211 for its clinical programs. Its CAS number is 1165910-22-4. It is notable for possessing one of the highest binding affinities for the androgen receptor among all characterized SARMs, with a Ki of approximately 1 nM, and is widely described in the research literature as the most potent SARM to have progressed into clinical trials based on its anabolic-to-androgenic selectivity ratio.
LGD-4033 is a full agonist of the androgen receptor (AR) — the same receptor activated by testosterone and dihydrotestosterone (DHT). Its selectivity derives from tissue-specific differential gene expression downstream of AR activation rather than from partial agonism. In skeletal muscle and bone, LGD-4033 binding to AR produces strongly agonistic, anabolic transcriptional outputs — driving muscle protein synthesis gene programs and bone remodeling pathways. In the prostate gland and reproductive tissues, it produces partially agonistic or antagonistic effects, mechanistically reducing androgenic activity in these tissues relative to muscle. This dissociation of anabolic and androgenic effects in preclinical studies is the central pharmacological property that distinguishes SARMs from non-selective androgens such as testosterone and synthetic anabolic steroids. The compound does not undergo significant 5-alpha reduction to DHT and does not aromatize to estrogen — two conversion pathways responsible for significant side effects with classical androgens.
The key Phase 1 multi-dose clinical trial, published in the Journal of Gerontology by Basaria et al. (2013), enrolled 76 healthy young men in a 21-day, randomized, double-blind, placebo-controlled study. The trial found: dose-dependent increases in lean body mass in all active arms versus placebo; no significant change in fat mass; no significant change in prostate-specific antigen (PSA); no significant change in haematocrit; and no clinically relevant liver enzyme elevations at the doses studied. LGD-4033 was well tolerated across the 21-day period. The trial also confirmed dose-dependent suppression of total testosterone and sex hormone-binding globulin (SHBG) — a key safety finding establishing that LGD-4033 suppresses the hypothalamic-pituitary-gonadal (HPG) axis, with testosterone levels beginning to recover toward baseline within five weeks of stopping.
The most significant clinical data for LGD-4033 comes from Viking Therapeutics' 12-week, Phase 2 randomized controlled trial in patients recovering from non-elective hip fracture surgery — a population that typically loses up to 11% of lean muscle mass, 4.6% bone density, and gains up to 7% body fat in the year following fracture. The trial achieved its primary endpoint: statistically significant, dose-dependent increases in lean body mass, less head, ranging from 4.8% to 9.1% following VK5211 treatment compared to placebo. Secondary endpoints were also met, including statistically significant increases in appendicular lean body mass and total lean body mass across all doses. At the highest dose, patients showed greater than 20-metre improvement in 6-minute walk distance over placebo — a functionally meaningful outcome. Results were presented in a plenary oral session at the American Society for Bone and Mineral Research (ASBMR) Annual Meeting in 2018.
Preclinical work, including primate data, confirmed dose-dependent anabolic effects with reduced androgenic activity in reproductive tissues. In a 13-week primate study, male and female monkeys showed significant quantity-dependent increases in lean body mass at doses of 0.6, 3, 15, and 75 mg/kg, with 70% of increased body mass retained after a four-week recovery period. Notably, only the highest dose group (75 mg/kg) was discontinued early due to toxicity — at a dose significantly exceeding any tested in human trials. In postmenopausal rat models, LGD-4033 demonstrated anabolic effects on muscle and bone with markedly reduced virilizing effects compared to testosterone, supporting its research relevance for women with hormonal decline. A 2025 study published in Naunyn-Schmiedeberg's Archives of Pharmacology, however, found that ligandrol combined with endurance training in healthy male rats negatively affected lipid profiles, hormonal parameters, and endurance capacity — a finding that adds complexity to simplistic selectivity claims in the context of combined exercise exposure.
The clinical trial literature identifies several consistent safety signals. Testosterone suppression is the most consistently documented: LGD-4033 suppresses the HPG axis in a dose-dependent manner, reducing total testosterone and SHBG, though testosterone recovery toward baseline was observed within approximately five weeks of discontinuation in the Phase 1 trial. HDL cholesterol reduction is another consistent lipid finding across trials. Elevated liver enzymes have been reported in some studies, and a pattern of drug-induced liver injury (DILI) cases has been documented in the medical literature — including published case reports of significant hepatotoxicity in individuals using unregulated research-grade material. Headache and dry mouth have been noted as minor adverse effects. The prostate selectivity documented in preclinical studies has generally been maintained in clinical trials, with no significant PSA changes at therapeutic research concentrations. Long-term cardiovascular safety and endocrine effects beyond several weeks of treatment remain undercharacterized.
Within the SARM class, LGD-4033 is distinguished by its exceptionally high androgen receptor binding affinity (Ki ≈ 1 nM) — among the highest of any characterized SARM — and by its full agonist activity at AR in muscle tissue. Enobosarm (ostarine, MK-2866) is the most clinically studied SARM, with multiple Phase 2 and Phase 3 trials completed in cancer cachexia patients and a more developed regulatory history, including two completed but failed Phase 3 trials. RAD-140 (testolone) has less clinical data than LGD-4033 but higher selectivity claims in preclinical work. Andarine (S-4) is associated with vision disturbance adverse effects not seen with LGD-4033. In terms of potency per molar concentration and the lean mass gains demonstrated per unit time in Phase 1 data, LGD-4033 is broadly considered the most potent SARM with published human trial data. Its HPG axis suppression at research concentrations is also more pronounced than enobosarm at equivalent anabolic exposures.
Liver safety is an area of significant concern that has emerged in the post-Phase 1 literature. While the controlled Phase 1 trial did not identify clinically meaningful liver enzyme elevations at short-term research concentrations, published case reports and pharmacovigilance data have documented drug-induced liver injury (DILI) — including cholestatic hepatitis and markedly elevated transaminases — in individuals exposed to LGD-4033 from unregulated sources. A critical confound is that research chemical products sold as LGD-4033 frequently contain incorrect compounds, incorrect concentrations, or undisclosed adulterants — making it impossible to attribute DILI cases definitively to the pure compound versus contamination. The mechanism of potential hepatotoxicity is not fully characterized, but some researchers have proposed that as a non-17-alpha-alkylated compound, LGD-4033's liver effects may differ mechanistically from classical oral anabolic steroid hepatotoxicity. Liver safety monitoring is identified in the clinical trial literature as a key requirement for any future longer-term studies.
Yes. LGD-4033 is prohibited under the WADA Prohibited List in class S1 — Anabolic Agents, where all SARMs are explicitly listed as a class. This is an in-competition and out-of-competition prohibition — meaning detection at any point in an athlete's calendar triggers a doping violation, not only during events. LGD-4033 has been at the center of several high-profile anti-doping cases across professional sports, including suspension cases in rugby union, cricket, cycling, and combat sports. Detection methods have advanced significantly — urine and blood methods based on UHPLC-HRMS can now detect LGD-4033 and its metabolites for several weeks post-exposure at nanogram-per-millilitre sensitivity. The compound's long detection window relative to its washout period for endogenous hormone recovery makes doping control timing a particular challenge in adjudicating contamination versus deliberate use claims.
As of mid-2026, LGD-4033 has not received FDA approval or regulatory approval from any major authority for any clinical indication. It remains classified as an Investigational New Drug (IND) in the United States. As of March 2023, it continues to be in Phase 2 clinical development under Viking Therapeutics (as VK5211) for the treatment of muscle atrophy and hip fracture rehabilitation — no Phase 3 trial has been initiated or announced. The compound has not progressed to NDA submission. It is available from research chemical suppliers as a Research Use Only (RUO) material for qualified in vitro researchers. The gap between LGD-4033's strong Phase 2 clinical results — particularly the hip fracture data — and the absence of Phase 3 progression has been noted in the academic literature, with the commercial SARM market's suppression of pharmaceutical development incentives cited as a contributing factor alongside residual safety concerns requiring longer-duration human studies before regulatory submission could be supported.





