
Cardiogen
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Cardiogen (AEDR): A Short Cardiac Bioregulator With Unusually Broad Research Ambitions
Cardiogen is a short synthetic tetrapeptide, AEDR, studied in research contexts as a cardiac bioregulator from the Khavinson peptide group. In preclinical data, it has drawn attention because in cellular and tissue models it was associated with modulation of the expression of proteins involved in myocardial structure, apoptosis, and the cellular stress response.
In published observations from experimental models, Cardiogen showed signals linked to support of cardiomyocyte proliferation, changes in p53-associated processes, effects on fibroblast activity, and reductions in markers of oxidative stress.
The concept itself is a point of particular interest: a very small peptide with ambitions almost as broad as an entire research program. For those studying short peptides, epigenetic regulation, and tissue-specific bioregulators, Cardiogen appears to be an unusual and intriguing subject for further consideration.
Cardiogen (Ala-Glu-Asp-Arg / AEDR): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version
Cardiogen is a synthetic tetrapeptide — four amino acids in the sequence Ala-Glu-Asp-Arg (AEDR) — developed within the bioregulator peptide research programme led by Professor Vladimir Khavinson at the St. Petersburg Institute of Bioregulation and Gerontology in Russia. It is designed as a cardiac-specific bioregulator: a short peptide intended to modulate gene expression in heart muscle cells (cardiomyocytes) and cardiac fibroblasts.
Cardiogen belongs to a specific intellectual tradition of “peptide bioregulators” developed in Soviet and post-Soviet Russia, which operates from a theoretical framework about short-peptide/DNA interaction that is not yet mainstream in Western molecular biology. The framework is scientifically plausible, and the publications are peer-reviewed (appearing in Molecules, Biochemistry Moscow, and various Russian journals). But independent replication by Western research groups is sparse, and no human clinical trial data has been published for Cardiogen specifically. Understanding Cardiogen properly requires understanding the Khavinson bioregulator framework — both what it proposes and where its evidentiary limits lie.
| At a glance | |
|---|---|
| Full name | Cardiogen; H-Ala-Glu-Asp-Arg-OH |
| Abbreviation | AEDR |
| Type | Synthetic tetrapeptide bioregulator |
| MW / Formula | ~489.5 Da; C&sub1;&sub8;H&sub3;&sub1;N&sub7;O&sub9; |
| Developer | Vladimir Khavinson, St. Petersburg Institute of Bioregulation and Gerontology |
| Proposed target tissue | Cardiac muscle (cardiomyocytes and cardiac fibroblasts) |
| Proposed mechanism | Short peptide–DNA/histone interaction → modulation of cardiac gene expression |
| FDA/EMA status | ❌ Not approved; not in clinical trials |
| Human clinical data | ❌ None published for Cardiogen specifically |
| WADA | Not specifically listed |
The Khavinson Bioregulator Framework: Understanding the Context
Vladimir Khavinson (born 1946) is a Russian gerontologist whose work began in the late 1960s with a Soviet military research mandate: to address accelerated ageing in soldiers and cosmonauts exposed to extreme stressors including radiation, hypoxia, and physical overload. The core hypothesis that emerged from decades of this work: tissues produce tissue-specific short peptides that act as endogenous gene expression regulators; with ageing, the production of these regulatory peptides declines; exogenous administration of the same or analogous peptides can restore gene expression to more youthful patterns, slowing age-related functional decline.
This programme produced two classes of products: Cytomaxes (polypeptide complexes extracted from animal organ tissue, e.g., Chelohart from calf heart, Cortexin from calf cerebral cortex — registered pharmaceuticals in Russia) and Cytogens (synthetic short peptides of 2–4 amino acids derived by identifying the minimal active sequence from tissue extracts). Cardiogen (AEDR) is the synthetic Cytogen corresponding to the cardiac tissue.
The foundational mechanism claim: short peptides (2–7 residues) can penetrate into the nuclei and nucleoli of cells and interact with the nucleosome, histone proteins, and both single- and double-stranded DNA. DNA–peptide interactions, including sequence recognition in gene promoters, are proposed as important for template-directed synthetic reactions, replication, transcription, and reparation.[1]
The Proposed Mechanism: Short Peptide–DNA Interaction
What the theory proposes
The Khavinson group proposes that short peptides can: (1) enter cells via peptide transporters (PEPT1, PEPT2) or direct diffusion; (2) reach the nucleus through the nuclear envelope; (3) bind DNA directly — interacting with specific promoter sequences or with histone proteins that regulate chromatin accessibility; and (4) alter gene expression by shifting the transcriptional programme toward a more youthful pattern. For Cardiogen specifically, the proposed interactions focus on cardiac transcription factors (GATA4, NKX2-5) and genes encoding structural cardiomyocyte proteins.
Short peptides can regulate functions of the endocrine, nervous, and immune systems and their ability to regulate gene expression and protein synthesis has been demonstrated across plants, microorganisms, insects, birds, rodents, primates, and humans. Peptides can also regulate the status of DNA methylation, an epigenetic mechanism for the activation or repression of genes in both normal conditions and in pathology and senescence.[1]
Specific published experimental findings
Cell culture studies: In embryonic fibroblast cultures, Cardiogen (AEDR) increased expression of cytoskeletal proteins (actin, tubulin, vimentin) 2–5-fold and nuclear matrix proteins (lamin A, lamin C) 2–3-fold. Cardiogen was shown to enter HeLa cells and distribute throughout cytoplasm, nucleus, and nucleolus — establishing cellular uptake. The peptide AEDR proved to reinforce expression of cyto- and karyoskeleton proteins; the mechanism of action is based on its ability to activate synthesis of proteins in cyto- and karyoskeleton, thereby enhancing cell proliferation and reducing apoptosis.[2]
Cardiomyocyte effects: Available research suggests Cardiogen may stimulate cell proliferation in cardiac tissue and suppress apoptosis in myocardial cells, presumably via lowering p53 protein expression. Researchers speculate that Cardiogen may improve long-term outcomes in cardiac remodelling and congestive cardiac failure by stimulating cardiomyocyte proliferation, which in turn may reduce fibroblast growth and potentially decrease fibrosis formation.
Animal model data: In rat models of ischaemia and chemically-induced cardiac stress, Cardiogen showed cardioprotective effects: reduced infarct size (20–30% in some reports), improved ECG parameters, reduced lipid peroxidation, and increased antioxidant enzyme activity (SOD, catalase, GPx). In aged rat models, Cardiogen improved heart rate variability and reduced arrhythmia frequency.[3]
Scientific assessment of the mechanism
The peptide–DNA interaction hypothesis has genuine precedent. Small positively-charged molecules (including short peptides with Arg and Lys residues) are known to interact electrostatically with DNA. The Arg residue in AEDR provides a positively-charged guanidinium group that can form hydrogen bonds and electrostatic interactions with the negatively-charged phosphate backbone of DNA. However, several questions remain unresolved: Sequence specificity — for short peptides to produce tissue-specific effects, they would need to interact with specific DNA sequences at specific gene promoters rather than binding DNA non-specifically; such short molecules have insufficient structural complexity to recognise specific sequences with the precision that transcription factors (typically 200–300+ amino acids) achieve. Concentration requirements — whether exogenously administered Cardiogen reaches the concentrations needed in cardiomyocyte nuclei after systemic distribution has not been formally pharmacokinetically characterised. Alternative mechanisms — the observed effects could theoretically occur through cell surface receptor-mediated pathways, intracellular protein-peptide interactions, or non-specific ionic interactions with chromatin.
The honest assessment: the mechanism is plausible in broad outline, the cell culture data is suggestive, and findings are internally consistent across Khavinson publications. However, the mechanistic detail required for confident clinical extrapolation — sequence-specific DNA binding, precise gene targets, confirmed intracellular concentrations — has not been published in sufficient molecular detail to fully characterise how Cardiogen works.
Cardiogen vs. Related Cardiac Bioregulators in the Khavinson System
| Product | Type | Target | Nature |
|---|---|---|---|
| Chelohart | Polypeptide complex | Cardiomyocytes (cardiac muscle) | Animal extract (bovine heart); “Cytomax”; registered Russian pharmaceutical |
| Cardiogen (AEDR) | Synthetic tetrapeptide | Cardiac tissue (cardiomyocytes + fibroblasts) | Synthetic; “Cytogen”; research compound |
| Ventfort (KED) | Synthetic tripeptide | Vascular endothelium | Synthetic; “Cytogen”; focuses on blood vessels |
| Vesugen (LKE) | Synthetic tripeptide | Vascular tissue | Synthetic; “Cytogen” |
Within the Khavinson system, Chelohart (the natural extract) is the primary cardiac therapeutic product with the longest clinical use history in Russia. Cardiogen (AEDR) is the synthetic equivalent — smaller, purer, and more consistent than the extract, but with a shorter research history and no independent clinical validation.
The P53 Question
P53 is the “guardian of the genome” — a tumour suppressor protein that induces cell cycle arrest and apoptosis in response to DNA damage. In ageing and post-ischaemic cardiac tissue, elevated p53 activity promotes cardiomyocyte apoptosis, contributing to progressive cardiac dysfunction. Cardiogen was observed to reduce p53 protein expression in cell culture models, suggesting an anti-apoptotic mechanism. ⚠️ However, p53 suppression is a double-edged sword: while reducing excessive p53-driven apoptosis in the post-ischaemic context may be cardioprotective, p53 is also a tumour suppressor. Chronic suppression of p53 raises theoretical oncogenic concerns that have not been formally addressed in long-term animal oncogenicity studies for Cardiogen specifically.
The Evidence Quality Problem: Being Honest About Khavinson Research
The Khavinson bioregulator research programme has produced a large body of literature — 775+ published papers over a career. The 2021 systematic review in Molecules (MDPI) is accessible in English and peer-reviewed. Findings have appeared in Biochemistry (Moscow), Advances in Gerontology, Bulletin of Experimental Biology and Medicine, and occasionally in International Journal of Molecular Sciences and Cells. Most Cardiogen research comes from Russian sources, and independent replication in Western journals is limited.
The Khavinson programme has conducted what it describes as long-term clinical studies of bioregulator complexes (Epithalamin, Thymalin) in elderly populations, with claimed mortality-reduction outcomes, published primarily in Russian-language journals from the 1990s–2000s. Cardiogen specifically has no published human clinical trial data, and no registered trial appears in ClinicalTrials.gov or the EU Clinical Trials Register.
Administration Routes and Formulations
In the research literature, Cardiogen has been administered via intraperitoneal or subcutaneous injection in rodent studies. Commercially it is also sold in oral (capsule) formulations. The theoretical basis for oral absorption: Cardiogen’s 4-amino acid size places it within the range that intestinal peptide transporters (PEPT1/PEPT2) can potentially absorb intact. The Khavinson group has published on the feasibility of transporter-mediated absorption of ultrashort peptides (Biomolecules, 2023).[6] Whether AEDR specifically achieves meaningful systemic bioavailability from oral administration has not been formally demonstrated with pharmacokinetic measurements in humans or animals.
Comparison with Related Compounds
| Compound | Sequence | Mechanism | Evidence quality | Status |
|---|---|---|---|---|
| Cardiogen | AEDR (4 AA) | Proposed DNA/gene expression modulation | Preclinical (Khavinson group only) | Research only |
| Chelohart | Polypeptide complex | Tissue extract; similar mechanism | Preclinical + Russian clinical use | Russian supplement |
| TB-500 | 43 AA fragment | Actin/G-actin; angiogenesis | Preclinical; cardiac wound healing | WADA prohibited; FDA Cat. 2 |
| BPC-157 | 15 AA | NO pathway; angiogenesis | Preclinical; extensive | FDA Category 2 |
| SS-31 (Elamipretide) | 4 AA | Mitochondrial cardiolipin interaction | Phase 2/3 clinical trials; FDA-approved | Approved (Barth syndrome) |
SS-31 (Elamipretide) is an instructive comparison — also a synthetic tetrapeptide with cardiac applications, but developed through the conventional Western drug development pathway with published clinical trial data and FDA approval. The contrast illustrates what Cardiogen’s evidence base is currently missing.
Common Misconceptions
“Cardiogen is a natural peptide extracted from the heart.”
Cardiogen (AEDR) is a fully synthetic tetrapeptide. The parent compound Chelohart is extracted from bovine heart tissue. Cardiogen was developed as a synthetic analogue designed to replicate the active fragment of the tissue extract.
“Khavinson’s research proves Cardiogen works in humans.”
The Khavinson group has conducted long-term studies with bioregulator complexes (not Cardiogen specifically) in elderly human populations, but these have not been independently validated. No randomised controlled trial of Cardiogen has been published for any human endpoint.
“Short peptides can’t enter the nucleus — the mechanism is impossible.”
Cell penetration by short peptides and interactions with nuclear components is a real and studied phenomenon. Short cell-penetrating peptides exist, small molecules routinely enter nuclei, and peptide–DNA interactions are well-characterised in other contexts (e.g., arginine-rich peptides binding nucleic acids). The mechanism is not physically impossible. The question is whether effects occur at physiologically achievable concentrations with sufficient specificity to produce the claimed tissue effects.
“Russian peptide research is not real science.”
Russian biomedical research published in peer-reviewed international journals is real science subject to the same general review process as Western publications. The appropriate epistemic concern with the Khavinson programme is not its national origin but the absence of independent replication and the concentration of all relevant research in a single institutional group.
Key Takeaways
- Cardiogen is a synthetic tetrapeptide (AEDR) from the Khavinson bioregulator tradition, designed as a cardiac-targeted gene expression modulator. It is one of a family of similar short peptides developed at the St. Petersburg Institute of Bioregulation and Gerontology.[1]
- The proposed mechanism — short peptide entry into cardiomyocyte nuclei, interaction with DNA and histones, and modulation of cardiac gene expression — is scientifically plausible but not yet established with the mechanistic precision that regulatory review would require. Direct DNA binding is possible; sequence-specific gene regulation by a 4-amino acid peptide is less clearly demonstrated.
- ⚠️ The preclinical evidence is suggestive but comes from a single research tradition. Cytoskeletal protein upregulation, anti-apoptotic effects, ischaemia protection in rodent models, and cardioprotection in aged animals are reported consistently by Khavinson’s group. Independent replication by Western groups is essentially absent.[2][3]
- ⚠️ No human clinical trial data exists for Cardiogen. The compound is not approved anywhere and has not entered a registered clinical trial. This is the central epistemic gap.
- The compound is not dangerous in the conventional sense — no significant safety signals have emerged in animal studies, and the constituent amino acids have no inherent toxicity at plausible doses. The primary risk is therapeutic assumption: people may forgo evidence-based cardiac care in favour of an unvalidated research compound.
References
Primary Publications on Cardiogen/AEDR
- Khavinson VKh, Popovich IG, Linkova NS, Mironova ES, Ilina AR. Peptide regulation of gene expression: a systematic review. Molecules. 2021;26(22):7053. doi:10.3390/molecules26227053
- Chalisova NI, Linkova NS, Zhekalov AN, et al. Effect of amino acids and Cardiogen on the development of myocardial tissue culture from young and old rats. Advances in Gerontology (Uspekhi Gerontologii). 2009;22(3):409–413.
- Khavinson VKh et al. Cardioprotective effects of short peptides. Bulletin of Experimental Biology and Medicine. 2006. (Ischaemia model data)
- Korkushko OV, Khavinson VKh, et al. Antioxidant and cardioprotective effects of Cardiogen in rat models. PubMed 22708326. 2012.
Mechanism Papers
- Ashapkin VV, Linkova NS, Khavinson VKh, Vanyushin BF. Epigenetic mechanisms of peptidergic regulation of gene expression during aging of human cells. Biochemistry (Moscow). 2015;80(3):310–322.
- Khavinson VKh, Linkova NS, Rudskoy AI, Petukhov MG. Feasibility of transport of 26 biologically active ultrashort peptides via LAT and PEPT family transporters. Biomolecules. 2023;13(3):552.
Khavinson Overview
- Khavinson V, Linkova N, Dyatlova A, Kantemirova R, Kozlov K. Senescence-associated secretory phenotype of cardiovascular system cells and inflammaging: perspectives of peptide regulation. Cells. 2023;12(1):106.
- Khavinson VK. Peptide regulation of aging. SPb: Nauka. 2002. (Primary monograph of the bioregulator programme)
Key Investigator
- Vladimir Khatskelevich Khavinson, MD, PhD, DSc — Professor, Head of the Department of Biogerontology, Saint Petersburg Institute of Bioregulation and Gerontology; Group of Peptide Regulation of Aging, Pavlov Institute of Physiology, Russian Academy of Sciences. 775+ published papers; 196 patents. The entire Cardiogen evidence base originates from his institution.
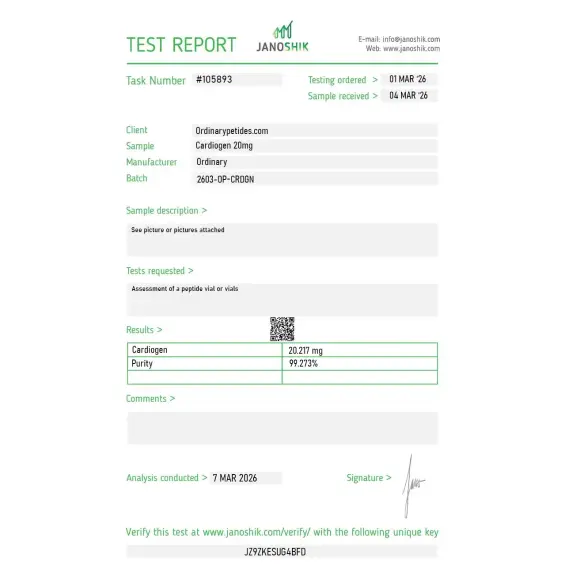
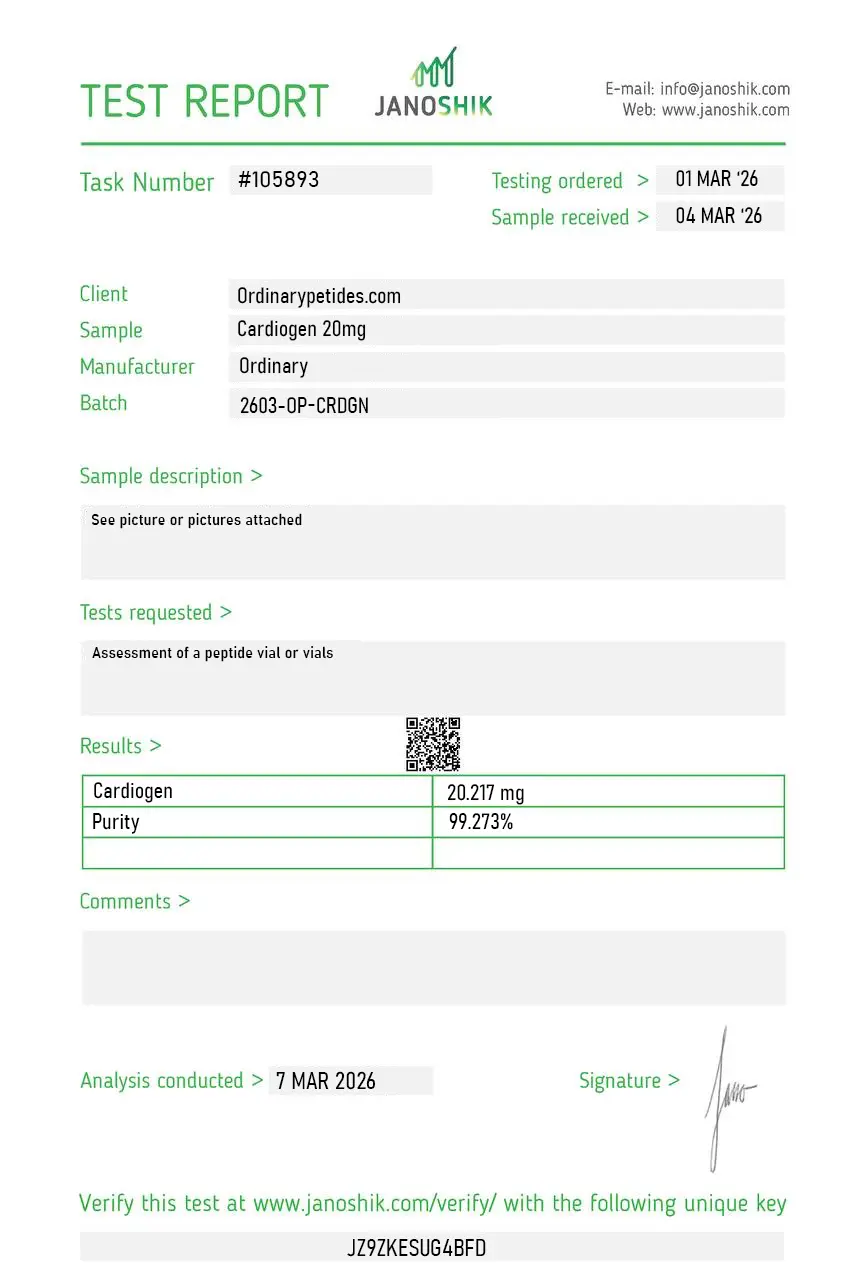
Certificate of Analysis
An independent test report is available for Cardiogen 20mg. This report provides batch-level documentation and analytical verification information for research reference.
Based on 1 reviews
5.0
The dissolution behavior was unremarkable — tripeptide went into bacteriostatic water cleanly, no haze, no aggregation. For a short Khavinson-tradition bioregulator, that simple handling is what you'd expect from a properly synthesized small peptide.
Cardiogen is a synthetic tetrapeptide — a short chain of four amino acids with the sequence Ala-Glu-Asp-Arg (AEDR). It belongs to a class of compounds called peptide bioregulators, developed in the 1980s and 1990s by Dr. Vladimir Khavinson and colleagues at the St. Petersburg Institute of Bioregulation and Gerontology in Russia. It was specifically designed to target cardiac tissue at the gene expression level and is considered one of the most organ-specific peptide bioregulators in this research lineage, alongside Thymalin for the thymus and Epitalon for the pineal gland.
Cardiogen works by entering cells and traveling to the nucleus, where it binds to specific DNA and histone sites to modulate gene expression. Its primary mechanism in cardiac tissue is suppressing p53 protein expression — p53 being a key regulator of apoptosis (programmed cell death). By downregulating p53, Cardiogen protects cardiomyocytes from premature cell death, stimulates their proliferation, and limits the excessive fibroblast activity that causes scar tissue formation after cardiac injury. It also upregulates cytoskeletal proteins such as actin, vimentin, and tubulin, supporting cellular structure and integrity. Notably, it appears to have the opposite effect in tumor cells — promoting rather than suppressing apoptosis, suggesting a context-dependent "smart selectivity."
Research in animal and cell culture models points to several areas of cardiovascular benefit. These include improved cardiomyocyte survival and proliferation, reduced scar tissue and fibrosis after cardiac injury, support for cardiac remodeling in heart failure, improved blood pressure regulation, better mitochondrial function and energy efficiency in heart muscle cells, enhanced exercise tolerance and stamina, and potential synergistic effects when used alongside conventional cardiovascular treatments. Studies also show it promotes cell growth equally in young and aged cardiac tissue — a significant finding given that older tissue is generally less responsive to regenerative signals.c
Cardiogen has no formal FDA approval and as of 2025 has not advanced to human clinical trials in the Western research framework. Most of its clinical observational data comes from decades of use in Russia and Eastern Europe, where peptide bioregulators have been integrated into cardiovascular and longevity medicine. It remains classified as a research compound in Western markets.
In preclinical animal studies it has been delivered via subcutaneous and intraperitoneal injection at microgram-per-kilogram doses. In clinical observational settings in Russia it has been used both orally and subcutaneously, typically in cycles of 10 to 20 days repeated every 3 to 6 months. Oral and sublingual forms are reported to have good bioavailability for a peptide of this size. No standardized human dosing protocol has been established through formal clinical trials.
Cardiogen has a reported minimal side effect profile across decades of Russian observational use, with no significant allergic reactions or drug interactions documented in the existing literature. Preclinical animal studies showed good tolerability. However, the absence of formal human clinical trials means that comprehensive long-term safety data in humans does not yet exist, and unknown risks cannot be excluded.
People with active cancer should exercise caution despite its reported pro-apoptotic effect on tumor cells, as the full picture of its cellular growth effects in humans remains incompletely characterized. Pregnant or breastfeeding women should avoid it. Individuals with serious cardiac conditions should only consider it under direct cardiologist supervision and not as a replacement for established evidence-based treatments. Given the absence of Western clinical trial data, use should be approached with appropriate caution and medical oversight.





