
KLOW
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
Klow Blend: Four Peptides, One Smarter Research Stack
Klow Blend combines four research peptides — BPC-157, TB-500, KPV, and GHK-Cu — into one formulation designed to cover more than just "repair" on paper. In the research context, BPC-157 has been studied for angiogenesis and nitric oxide signaling, TB-500 for actin-driven cell migration, GHK-Cu for collagen-related activity and extracellular matrix support, while KPV stands out as the added anti-inflammatory piece with a distinct NF-κB and PepT1-linked mechanism.
That matters because KPV gives the blend a more explicit gut-and-skin inflammation angle, rather than simply stacking more of the same. In preclinical models, those pathways look complementary, which is exactly why the formula attracts attention in regenerative research circles.
But the honest part stays the same: the four-peptide combination itself has never been tested in a human clinical trial, and the evidence depth is very uneven across the individual components. So Klow Blend is best understood as a research-driven, mechanistically coherent concept — interesting, layered, and still far from clinically proven.
KLOW (GHK-Cu + BPC-157 + TB-500 + KPV Peptide Stack): A Scientific Review
Based on peer-reviewed literature — see References. Last updated: April 2026.
The Short Version: KLOW = GLOW + KPV
KLOW is a direct evolution of the GLOW stack (GHK-Cu + BPC-157 + TB-500), covered in the preceding article in this series. The only structural difference between the two products is the addition of a fourth peptide: KPV (Lys-Pro-Val), the C-terminal tripeptide of alpha-melanocyte-stimulating hormone (α-MSH).
The rationale for the addition is coherent: the GLOW stack addresses tissue repair and collagen synthesis (GHK-Cu), angiogenesis and healing (BPC-157), and cell migration and connective tissue remodelling (TB-500). What it does not directly address is systemic and mucosal inflammation, particularly the NF-κB-mediated inflammatory signalling that underlies gut pathology, autoimmune flares, and chronic inflammatory states. KPV — which operates primarily as an NF-κB suppressor acting through the gut epithelial peptide transporter PepT1 — fills this gap. The marketing framing from community sources is blunter: GLOW is for skin rejuvenation and injury recovery; KLOW is for the same plus gut dysfunction, chronic inflammation, or autoimmune involvement.
| At a glance | |
|---|---|
| KLOW components | GHK-Cu + BPC-157 + TB-500 + KPV |
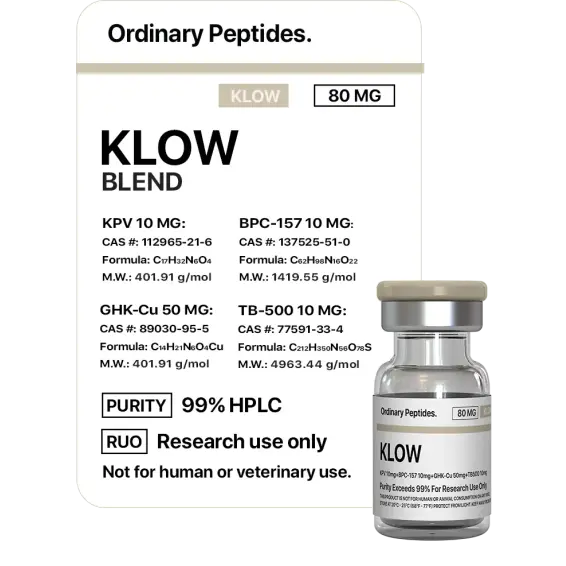
| Standard vial | 80 mg total: GHK-Cu 50 mg / BPC-157 10 mg / TB-500 10 mg / KPV 10 mg |
| Ratio | 5:1:1:1 (GHK-Cu dominant) |
| GLOW comparison | GLOW = GHK-Cu + BPC-157 + TB-500 (70 mg, no KPV) |
| KPV’s role | Anti-inflammatory; NF-κB inhibition; gut mucosal targeting |
| FDA status | ⚠️ BPC-157 and TB-500: Category 2, prohibited for compounding |
| WADA | ❌ TB-500: Prohibited S2 at all times (4-year standard ban) |
| Human clinical trials for combination | ❌ None |
Component Overview: What Each Peptide Contributes
All four KLOW components are covered in full in separate articles in this series. This section provides the essential mechanism summary for each, with emphasis on their distinct roles within the stack.
GHK-Cu (Copper Tripeptide-1) — 50 mg / 62.5% of vial
Sequence: Gly-His-Lys (complexed with Cu²♠) — MW ~340 Da (peptide); copper complex ~403 Da. Naturally occurring human plasma peptide; levels decline with age (200 ng/mL at age 20 → ~80 ng/mL at age 60). The dominant component by mass and the primary driver of the stack’s collagen synthesis, skin regeneration, and ECM remodelling activity. Mechanisms: fibroblast collagen (types I, III), fibronectin, and glycosaminoglycan production; Nrf2/ARE pathway activation → antioxidant enzyme upregulation; TGF-β1-driven fibrosis reduction; copper delivery supporting lysyl oxidase, SOD, and other copper-dependent enzymes. Evidence quality: the strongest individual evidence base in the KLOW stack for skin applications; multiple controlled human studies of topical GHK-Cu cream; injectable GHK-Cu has no human trial data.
BPC-157 (Body Protection Compound-157) — 10 mg / 12.5% of vial
Sequence: Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val (15 AA); MW ~1,419 Da. Synthetic peptide derived from a region of the human gastric juice protein BPC. Role in KLOW: angiogenesis promotion (VEGFR2/Akt-eNOS signalling), tendon and ligament repair, gut mucosal healing, and anti-inflammatory effects. Contributes vascular supply to healing tissue, structural connective tissue repair, and gut barrier integrity (complementary to KPV, though via a different mechanism). Evidence quality: extensive preclinical rodent model data (>100 published studies); no published human clinical trials. FDA Category 2 — prohibited for routine compounding.[5]
TB-500 (Thymosin Beta-4 Fragment Ac-LKKTETQ) — 10 mg / 12.5% of vial
Sequence: Ac-Lys-Lys-Thr-Glu-Thr-Gln (residues 17–23 of Tβ4); MW ~799 Da. Fragment of the naturally occurring protein thymosin beta-4. Role in KLOW: cell migration facilitation (G-actin sequestration → actin polymerisation regulation), connective tissue remodelling, and wound healing at sites distal to injection via systemic distribution. Contributes fibroblast and keratinocyte migration, collagen matrix organisation, and flexibility/mobility improvement (reduced muscle fascia fibrosis). Evidence quality: preclinical data in animal wound, cardiac, and corneal repair models; a 2024 finding (Rahaman et al.) suggests bioactivity may reside in the Ac-LKKTE metabolite rather than parent TB-500; no published human RCTs. WADA S2 prohibited at all times; FDA Category 2 prohibited; DoD prohibited.[6][7]
KPV (Lys-Pro-Val) — 10 mg / 12.5% of vial
Sequence: Lys-Pro-Val (tripeptide; residues 11–13 of α-MSH C-terminus); MW ~342 Da. Endogenous cleavage product of α-melanocyte-stimulating hormone; naturally occurring in human tissues. The new addition versus GLOW — the stack’s dedicated anti-inflammatory agent:
NF-κB pathway inhibition: reduces transcription of pro-inflammatory cytokines (TNF-α, IL-1β, IL-6, IL-8). PepT1-mediated uptake in gut epithelium: KPV is transported by the intestinal peptide transporter PepT1, making it uniquely effective at delivering anti-inflammatory signals to gut mucosal cells — the mechanism underlying its activity in IBD models. Mast cell stabilisation: reduces histamine release and IgE-mediated responses. Melanocortin receptor independence: critically, KPV does NOT bind MC1R, MC3R, or MC5R, meaning it has none of the hormonal or pigmentation effects associated with α-MSH or Melanotan II.
Key preclinical evidence: Dalmasso et al. 2008 (Gastroenterology) established PepT1-mediated KPV uptake reducing intestinal inflammation in vitro (Km for hPepT1 ~700 μM);[1] Kannengiesser et al. 2008 (IBD) demonstrated anti-inflammatory activity in DSS and CD45RBhi transfer colitis mouse models;[2] Xiao et al. 2017 (Molecular Therapy) showed HA-KPV nanoparticles efficiently alleviate UC in mice.[3] Human clinical trials for KPV: none published. Regulatory status: not specifically prohibited for compounding; not WADA-prohibited.
The GLOW → KLOW Evolution: What the Addition of KPV Addresses
The GLOW stack targets wound healing and regeneration pathways: matrix synthesis (GHK-Cu), vascular supply (BPC-157), and cell migration (TB-500). What GLOW does not meaningfully address is the upstream inflammatory environment that often impairs healing in the first place. In conditions characterised by chronic low-grade inflammation — IBD, autoimmune disease, metabolic syndrome, ageing-associated inflammaging, or acute inflammatory flares — the healing pathways targeted by GLOW may be partially suppressed by the pro-inflammatory cytokine environment. NF-κB activation antagonises the healing response: it promotes catabolism, inhibits collagen synthesis, and suppresses the regulatory T-cell responses needed for orderly tissue resolution. KPV’s addition targets this gap.
| Target | GLOW coverage | KLOW coverage (KPV adds) |
|---|---|---|
| Collagen and ECM synthesis | GHK-Cu | GHK-Cu (unchanged) |
| Angiogenesis | BPC-157 | BPC-157 (unchanged) |
| Cell migration | TB-500 | TB-500 (unchanged) |
| NF-κB inflammatory signalling | Partial (BPC-157 has some anti-inflammatory activity) | ✅ KPV — direct NF-κB inhibitor |
| Gut mucosal inflammation | Partial (BPC-157 supports gut barrier) | ✅ KPV — PepT1 transporter mechanism at gut epithelium |
| Mast cell activity | Minimal | ✅ KPV — mast cell stabilisation |
| Systemic cytokine burden | Indirect | ✅ KPV — direct cytokine suppression |
The clinical decision framework community sources use: KLOW rather than GLOW when the primary concern involves gut dysfunction (IBD, leaky gut, IBS, dysbiosis), autoimmune activity, chronic systemic inflammation, or conditions where NF-κB-driven inflammatory signalling is a primary driver of pathology rather than a secondary consequence of injury.
The Synergy Question: Does Combining Four Peptides Produce Better Results?
This is the central claim underlying KLOW’s marketing. The four mechanisms are genuinely complementary: NF-κB inhibition (KPV) removes a brake on the healing response that GHK-Cu, BPC-157, and TB-500 are trying to accelerate; reducing pro-inflammatory cytokine burden (KPV) improves the local environment for angiogenesis (BPC-157) and cell migration (TB-500). These relationships are pharmacologically coherent.
⚠️ What the evidence cannot support: no published study has compared KLOW as a combination against individual components in any model; measured whether the four peptides interact pharmacokinetically; established whether the 5:1:1:1 ratio is optimal for any indication; or determined whether any component inhibits or reduces the activity of another when mixed in the same vial. The possibility of antagonistic interactions cannot be excluded without data. BPC-157 has some pro-inflammatory signalling early in the wound healing cascade (the initial inflammatory phase is necessary for proper healing); KPV suppresses inflammation. Whether KPV’s NF-κB inhibition at KLOW doses suppresses the early inflammatory signals that BPC-157 relies on is unknown. As community source peptide-db.com correctly notes: no one has studied whether these four peptides interact synergistically, antagonistically, or not at all when combined.[9]
Vial Composition and the Ratio Question
The de facto standard KLOW vial is 80 mg total: GHK-Cu 50 mg / BPC-157 10 mg / TB-500 10 mg / KPV 10 mg (5:1:1:1 ratio). GHK-Cu’s dominant mass (62.5% of the vial) reflects its typical standalone dosing: GHK-Cu is used at 50–100 μg per dose in most protocols, while BPC-157, TB-500, and KPV are typically used at 250–500 μg per dose. For the ratios to produce roughly equivalent doses of each component, GHK-Cu needs to be present in significantly higher absolute mass. However, this ratio reflects a pragmatic compounding reality rather than evidence-based optimisation — the 5:1:1:1 ratio has not been justified by dose-response studies or PK/PD modelling for any indication.
Regulatory Status
| Component | FDA compounding status | WADA | US DoD |
|---|---|---|---|
| GHK-Cu | Generally permissible | Not prohibited | Not listed |
| BPC-157 | ⚠️ Category 2 — prohibited | Not specifically listed | Prohibited |
| TB-500 | ⚠️ Category 2 — prohibited | ❌ S2 — prohibited at all times | Prohibited |
| KPV | Not specifically restricted | Not prohibited | Not listed |
The addition of KPV does not resolve the regulatory problem inherent in KLOW: the stack still contains two Category 2 FDA-prohibited compounds. Any clinic claiming to provide KLOW from an “FDA-approved compounding pharmacy” is making a claim that requires scrutiny. The WADA concern is specifically relevant for athletes: TB-500’s presence makes KLOW a prohibited stack for any athlete subject to anti-doping rules; the S2 category (non-specified substance) means the standard four-year ban applies to first offences.[8]
Safety Profile
Individual component safety profiles: GHK-Cu is generally well tolerated; theoretical copper accumulation concern with prolonged high-dose use; injectable route unvalidated in human studies. BPC-157: no human safety data; theoretical oncogenic concern from chronic angiogenesis promotion (FDA concern underlying Category 2 designation). TB-500: same oncogenic concern; WADA-prohibited; DoD-prohibited. KPV: no human clinical trials; immunosuppressive mechanism raises theoretical concern in infection contexts; generally considered low-risk based on natural endogenous origin.
⚠️ Combination-specific risks — no data exists: Product stability across the recommended storage period for a four-peptide mixture has not been formally characterised. Pharmacokinetic interactions (competition for elimination pathways; copper chelation by GHK affecting other components) are unknown. The combination of KPV-mediated immunosuppression and BPC-157-driven angiogenesis in immunocompromised individuals is a theoretical concern without clinical data to quantify it.
Most common reported adverse effects (community protocols, not clinical data): injection site reactions (mild; class effect of subcutaneous injection); nausea (class effect; transient); fatigue during early protocol stages; potential pigmentation changes attributed to GHK-Cu or KPV (reversible based on available individual component data).
KLOW vs. GLOW: The Practical Decision
GLOW is sufficient for skin rejuvenation and standard tissue repair. The practical decision point is whether active inflammation is part of the picture. Gut issues (IBD, leaky gut, chronic digestive inflammation), autoimmune flares, or any situation where the immune system is contributing to the problem makes the KPV component mechanistically relevant, and KLOW the more targeted choice. This framing should be accompanied by the honest caveat: neither GLOW nor KLOW has been tested clinically for any of these applications. The “more targeted choice” is more targeted at the level of mechanistic rationale; clinical outcomes remain undemonstrated for both.
Common Misconceptions
“KLOW is a more advanced version of GLOW that is better in every way.”
KLOW contains KPV, which adds an anti-inflammatory mechanism. Whether this addition is beneficial, neutral, or potentially interfering with the other components’ actions in any specific context has not been studied. More components is not inherently better; it is more complex and less understood.
“The four peptides have been proven to work synergistically.”
No study has examined the combination. Complementary mechanisms on paper are not proof of synergy in practice.
“KPV makes KLOW safer by reducing inflammation.”
KPV’s NF-κB inhibition is a systemic immunomodulatory effect, not simply a tissue-protective one. In the context of active infection or in immunocompromised individuals, suppressing inflammatory signalling can be counterproductive. “Anti-inflammatory” is not synonymous with “safer.”
“KLOW is from a different regulatory category than GLOW because it has natural ingredients.”
Both stacks contain TB-500 and BPC-157, both of which are FDA Category 2. The naturalness of any individual component does not alter the regulatory status of the stack.
Key Takeaways
- KLOW is GLOW with KPV added. The entire GLOW analysis (GHK-Cu, BPC-157, TB-500, evidence base, regulatory concerns) applies equally to KLOW. The GLOW article should be read alongside this one.
- ✅ KPV’s addition addresses a specific gap: NF-κB-mediated inflammation, particularly at gut mucosal surfaces. The PepT1-transporter mechanism makes KPV uniquely active in intestinal epithelium — its most validated preclinical application. This makes KLOW mechanistically more relevant than GLOW for conditions with a gut inflammatory component.[1][2]
- ⚠️ The regulatory situation is the same as GLOW: two of four components are FDA-prohibited for compounding. TB-500 adds WADA and DoD prohibition. KPV’s relative permissibility does not resolve the BPC-157/TB-500 problem.[8]
- ⚠️ No combination data exists. The synergy claim is biologically plausible but entirely unvalidated. No study has examined pharmacokinetic interactions, optimal ratios, or combination efficacy for KLOW as a stack.
- The clinical decision between GLOW and KLOW is rational at the mechanistic level. Choose KLOW (over GLOW) when chronic systemic inflammation, gut pathology, or NF-κB-driven inflammatory conditions are primary concerns. Choose GLOW (or neither) for pure tissue repair and skin rejuvenation without significant inflammatory component. Both choices lack clinical trial support; the distinction is mechanistic, not evidential.
References
KPV-Specific Literature
- Dalmasso G, Charrier-Hisamuddin L, Thu Nguyen HT, Yan Y, Sitaraman S, Merlin D. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology. 2008;134(1):166–178.
- Kannengiesser K, Maaser C, Heidemann J, et al. Melanocortin-derived tripeptide KPV has anti-inflammatory potential in murine models of inflammatory bowel disease. Inflammatory Bowel Diseases. 2008;14(3):324–331.
- Xiao B, Laroui H, Ayyadurai S, et al. Mannosylated biopolymeric nanoparticles for effective delivery of α-MSH C-terminal tripeptide KPV for ulcerative colitis. Molecular Therapy. 2017;25(4):870–882.
GHK-Cu Literature
- Pickart L, Margolina A. Regenerative and protective actions of the GHK-Cu peptide in the light of new gene data. International Journal of Molecular Sciences. 2018;19(7):1987.
BPC-157 Literature
- Sikiric P, et al. Multiple references (Zagreb group, 1993–present) — see BPC-157 article in this series.
TB-500 Literature
- Malinda KM, Goldstein AL, Kleinman HK. Thymosin beta4 stimulates directional migration of human umbilical vein endothelial cells. FASEB Journal. 1997.
- WADA Prohibited List 2024/2025: TB-500 listed under S2.
Regulatory
- FDA Category 2 Bulk Drug Substances list. BPC-157 and TB-500 designations. PCAC meeting records 2021–2023.
Stack Context
- KLOW vs. GLOW analysis and dosing reference. Peptide-db.com. April 2026. (Community-sourced; cited for ratio and framing analysis)
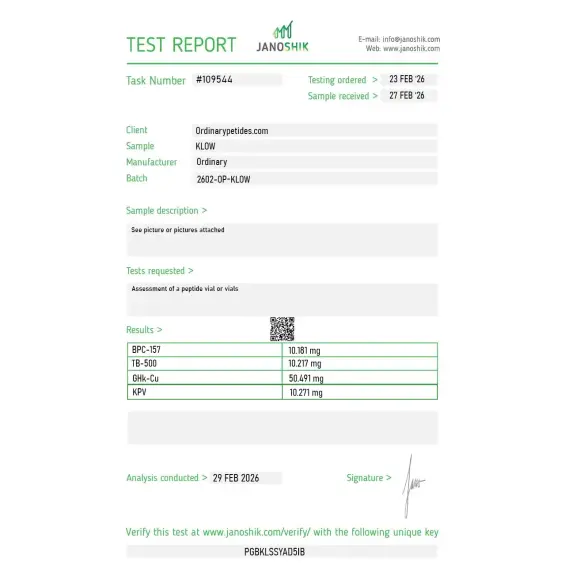
Certificate of Analysis
An independent test report is available for KLOW 80mg. This report provides batch-level documentation and analytical verification information for research reference.

The four-arm comparison design we ran (blend versus each component individually) became substantially more demanding with four peptides than with the three-component blend — quadruple the standalone reference materials, quadruple the matched-source variance to control. The matched-vendor advantage is more valuable here than for simpler blends. Knocking a star because reconstitution timing across four peptides at slightly different working concentrations was harder to standardize, and a multi-vial timing protocol would help.
The four-component formulation adds meaningful QC complexity over the three-component blend — now you're verifying four purities, three pairwise ratios, no quadruple-component interactions, plus the GHK-Cu metal-coordination stability across an additional peptide context. The certificate broke out each peptide's purity separately, which is the baseline expectation for a quad-blend. Material assayed cleanly in our component-resolved chromatography.
KLOW is a compounded four-peptide stack combining BPC-157, TB-500, KPV, and GHK-Cu in a single injectable vial. It is the evolution of the GLOW stack — GLOW contains the first three peptides, while KLOW adds KPV, a potent anti-inflammatory tripeptide. The standard formulation is an 80 mg vial containing GHK-Cu at 50 mg, with BPC-157, TB-500, and KPV at 10 mg each. It is designed to target tissue repair, inflammation, immune modulation, and skin regeneration through four complementary but distinct molecular pathways simultaneously.
BPC-157 is a 15-amino acid fragment derived from a gastric protective protein. It promotes tissue healing through nitric oxide signaling, stimulates new blood vessel formation, and supports recovery of tendons, ligaments, muscles, and the gut lining. TB-500 is a synthetic fragment of Thymosin Beta-4 that regulates actin — a key protein in cell structure. It drives cell migration during repair, reduces fibrosis, enhances flexibility in connective tissue, and supports cardiovascular and muscle regeneration. KPV is a tripeptide derived from the C-terminal region of alpha-melanocyte-stimulating hormone. It is a powerful anti-inflammatory that inhibits NF-κB signaling at nanomolar concentrations, reducing pro-inflammatory cytokines like TNF-α, IL-6, and IL-1β — with particular effectiveness in gut and epithelial tissue. GHK-Cu is a naturally occurring copper-binding tripeptide that stimulates collagen and elastin production, activates wound-healing genes, reduces oxidative stress, promotes angiogenesis, and supports skin remodeling and hair follicle health
The key difference is KPV. GLOW targets repair and skin regeneration through three peptides. KLOW adds KPV's dedicated immune-modulating and anti-inflammatory action, making it more suited for individuals dealing with chronic inflammation, autoimmune involvement, gut issues, or conditions where inflammation is the primary obstacle to healing. If GLOW is described as the beauty and repair blend, KLOW is considered the rebuild and resilience blend.
The synergistic combination targets multiple healing pathways at once. Benefits include accelerated recovery from musculoskeletal injuries, reduced systemic and localized inflammation, improved skin firmness and collagen density, enhanced gut lining integrity, reduced scar formation and fibrosis, improved joint mobility and connective tissue health, and stronger immune balance. Users and clinics also report improvements in energy, skin clarity, and overall recovery resilience with consistent use.
KLOW is given as a daily subcutaneous injection, typically reconstituted with bacteriostatic water. A gradual titration schedule is recommended — starting at lower doses and increasing over several weeks to assess tolerance. It is stored as a lyophilized powder, reconstituted immediately before use, then refrigerated at 2 to 8°C and used within 28 days. It pairs well with aesthetic procedures such as microneedling or can be used alongside injury rehabilitation protocols.
Yes. Long-term continuous use is not recommended, primarily because BPC-157 and TB-500 both stimulate angiogenesis — new blood vessel growth. While beneficial during defined healing phases, prolonged angiogenic signaling may carry theoretical risks in individuals with a history of cancer or abnormal tissue growth, as tumor cells exploit similar pathways. Most protocols recommend defined on-cycles followed by rest periods, with frequency and duration guided by a qualified physician.
People with active cancer or a personal history of cancer should avoid it due to the angiogenic properties of BPC-157 and TB-500. Pregnant or breastfeeding women should not use it. Those with autoimmune conditions should consult a physician before use, as immune modulation can have unpredictable effects in these individuals. As none of the components are FDA-approved for human therapeutic use, KLOW should only be used under the supervision of a licensed and qualified healthcare provider.





