

MK-677
For in vitro testing and laboratory use only. Not for human or animal consumption. Bodily introduction is illegal. Handle only by licensed professionals. Not a drug, food, or cosmetic. Educational use only.
MK-677 (Ibutamoren): A Non-Peptide Ghrelin Receptor Agonist at the Crossroads of GH/IGF-1 Axis Research, Secretagogue Pharmacology, and Somatic Aging Biology
MK-677, also known as Ibutamoren, is a non-peptide small molecule best known in the field of endocrine research, where it has been studied as a selective, orally active agonist of the ghrelin receptor (GHS-R1a) and linked to the biology of growth hormone secretion. In the research context, the main interest in this compound grew out of studies reporting sustained elevations of endogenous GH and IGF-1, preserved pulsatility, and an unusually clean endocrine profile — without measurable effects on cortisol or testosterone — in clinical and preclinical models. That sounds dramatic — and that is precisely why it attracts so much attention.
Published reports have also discussed its relationship with slow-wave sleep, lean mass, and bone mineral density, while preclinical data have connected it to a broader somatotropic and regenerative framework, including effects on muscle strength and recovery in age-related decline models. Still, a sober filter is essential here: a compelling endocrine story is not yet a ready-made anti-aging therapy in a vial. If only biology were that cooperative.
What makes MK-677 genuinely interesting is that it sits at the crossroads of GH/IGF-1 axis pharmacology, ghrelin biology, and the broader tradition of non-peptide secretagogues — a class designed to overcome the injection-only limits of peptide GHRPs. For readers who care not just about bold promises but about the actual scientific grounds for interest, this is exactly the kind of compound worth examining carefully — and without illusions.
MK-677 (Ibutamoren): A Scientific Review of the Oral Growth Hormone Secretagogue
Based on peer-reviewed literature — see References. Last updated: May 2026.
The Short Version
MK-677 is one of the more unusual compounds in this review series, because for once the story isn't "interesting preclinical data with no human trials." It's almost the opposite: substantial human clinical trial data going back nearly three decades, including a well-designed 2-year placebo-controlled study in older adults published in Annals of Internal Medicine, FDA Orphan Drug Designation, and pharmaceutical industry development that reached late-stage clinical trials before getting set aside.
The compound is also one of the most heavily marketed "research peptides" in the bodybuilding and longevity space — which is itself a piece of misdirection, because MK-677 isn't a peptide. It's a small, orally active, non-peptide molecule developed by Merck in the early 1990s. The mainstream framing as a "peptide" alongside BPC-157 and similar compounds is a marketing convenience, not a chemical fact.
The pharmacology is real and well-characterized. MK-677 is a selective agonist of the ghrelin receptor (GHSR-1a) — the same receptor that endogenous ghrelin activates, and the same target hit by injectable peptide secretagogues like ipamorelin. Activating that receptor stimulates the pituitary to release growth hormone (GH), which then stimulates the liver to produce IGF-1. The result is a sustained elevation of both GH and IGF-1 levels — the two hormones that drive most of the anabolic, body composition, and recovery effects people associate with growth hormone therapy. But unlike injectable HGH, MK-677 preserves the natural pulsatility of GH secretion, which is generally considered a feature.
In healthy older adults over 12 months, MK-677 at 25 mg/day increased fat-free mass by approximately 1.1 kg, raised GH and IGF-1 to young-adult levels, and was generally well-tolerated.[2] That sounds like a clear win. The catch is that the same trial showed:
- No improvement in muscle strength or physical function despite the increased fat-free mass
- Worsening of insulin sensitivity (Quicki index decreased, fasting glucose rose, HbA1c rose)
- Cortisol elevation of approximately 47 nmol/L
- Mild lower extremity edema in some participants
- Appetite increase and weight gain beyond just lean tissue
That's the central tension of MK-677: it does what it's supposed to do hormonally, but the downstream functional benefits are smaller than the hormone numbers would suggest, and the metabolic costs are real.
A second important data point is rarely discussed in the wellness press: a separate trial in older adults with hip fracture, sponsored by Merck, showed increased adverse events (including congestive heart failure) at MK-677-equivalent doses. This trial was a major factor in Merck's eventual decision not to pursue further development.[5]
| At a glance | |
|---|---|
| Generic name | Ibutamoren |
| Development codes | MK-677, MK-0677, L-163,191, LUM-201 |
| Former brand name | Oratrope (tentative) |
| Chemical class | Small molecule (non-peptide), spiropiperidine |
| Mechanism | Selective agonist of ghrelin receptor (GHSR-1a) |
| Effect | Stimulates endogenous GH and IGF-1 secretion |
| Originator | Merck Research Laboratories (early 1990s) |
| Current development holder | LUMOS Pharma (as LUM-201, for pediatric GHD) |
| First publication | Patchett et al., PNAS, 1995 |
| Major Phase 2 trial | Nass et al., Ann Intern Med, 2008 |
| FDA status | ❌ Not approved; Orphan Drug Designation 2017 for pediatric GHD |
| EMA status | ❌ Not approved; Orphan Drug Designation 2017 for pediatric GHD |
| WADA status | ⚠️ Prohibited — Class S2 (peptide hormones, growth factors, and related substances) |
| Half-life | ~6 hours; sustained GH/IGF-1 elevation with once-daily dosing |
| Oral bioavailability | Active orally; specific bioavailability ~7% |
Origin: Merck's Search for an Oral GH Therapy
The MK-677 story starts in a place that's easy to forget: the early 1990s pharmaceutical race to find an oral alternative to injectable growth hormone.
By that point, recombinant human growth hormone (rhGH) was an established but inconvenient therapy. It worked for growth hormone deficiency, certain pediatric conditions, and (controversially) HIV-associated wasting. But it required daily subcutaneous injection, was expensive, produced supra-physiologic single-pulse exposure rather than the natural pulsatile pattern, and had its own side effect profile. The market pressure for an oral GH alternative was substantial.
Merck's approach was to find a small molecule that would stimulate endogenous GH secretion rather than supplement GH directly. The biology suggested this should be feasible: there was a known peptide called GHRP-6 (growth hormone releasing peptide-6) that powerfully stimulated GH release through a then-unidentified receptor. Merck's medicinal chemistry program aimed to find a non-peptide small molecule that activated the same receptor with similar potency.
The Patchett et al. paper in PNAS in 1995 reported the result: L-163,191, later renamed MK-677, a spiropiperidine compound that selectively activated what would later be identified as the ghrelin receptor (GHSR-1a).[1] The compound was orally active, long-acting, and produced robust GH stimulation.
What happened next is the long, slow, mixed-results clinical development program. Phase 1 and 2 trials proliferated through the late 1990s and 2000s. The compound was tested in healthy young adults, healthy elderly adults, GH-deficient children, GH-deficient adults, obese subjects, hip fracture patients, and several other populations. The results were consistent on hormonal effects (GH and IGF-1 rise to young-adult levels). The results on clinical benefits and safety were inconsistent enough that Merck eventually halted development.
In 2017, LUMOS Pharma acquired rights to develop MK-677 as LUM-201 specifically for pediatric growth hormone deficiency. Both FDA and EMA granted Orphan Drug Designation. As of mid-2026, LUM-201 remains in clinical development for that specific indication. The broader development for adult muscle wasting, frailty, sarcopenia, and obesity has not been pursued by a major pharmaceutical company since Merck's withdrawal.
How It Works
The ghrelin receptor and growth hormone biology
Growth hormone secretion from the pituitary is regulated by a competing-signal system. GHRH (growth hormone-releasing hormone) from the hypothalamus stimulates GH release. Somatostatin inhibits it. The balance between these two signals — together with ghrelin from the stomach — produces the characteristic pulsatile pattern of GH secretion, with the largest pulses occurring during slow-wave sleep. For broader context on this hormonal axis and related compounds, see the Endocrine Research category.
Ghrelin acts on the growth hormone secretagogue receptor type 1a (GHSR-1a) — a G-protein-coupled receptor expressed in the hypothalamus, pituitary, and various peripheral tissues. Activation of GHSR-1a has multiple effects:
- Stimulates GHRH release
- Suppresses somatostatin release
- Directly activates pituitary somatotrophs
- Promotes appetite (ghrelin is the "hunger hormone")
- Affects sleep architecture (favors slow-wave sleep)
- Modulates insulin sensitivity (negatively)
- Affects mood and reward circuits
MK-677 is a selective non-peptide agonist of this receptor — pharmacologically a "ghrelin mimetic." A 2021 cryo-EM structure published in Nature Communications (Liu et al.) showed exactly how MK-677 binds GHSR-1a, illuminating the structural basis of its activity.[7]
What activation does
After MK-677 binds GHSR-1a, the downstream effects mirror what happens with elevated endogenous ghrelin:
- GH pulse amplitude increases. The natural pulsatile pattern is preserved (this is one of the compound's distinguishing features), but the peaks are higher.
- IGF-1 rises. The liver responds to the elevated GH exposure by increasing IGF-1 production. IGF-1 mediates many of GH's downstream effects on tissues.
- Appetite increases. This is direct GHSR-1a activation, separate from the GH/IGF-1 axis.
- Slow-wave sleep increases. This is documented in multiple trials, particularly relevant since GH peaks naturally during slow-wave sleep.
- Cortisol rises modestly. GHSR-1a activation increases ACTH release.
| Effect | Magnitude in human trials | Time course |
|---|---|---|
| GH peak amplitude increase | 1.5-1.8× baseline (Nass 2008) | Begins within days; sustained chronically |
| IGF-1 elevation | ~1.5× baseline; reaches young-adult range | Plateaus over weeks |
| Fat-free mass increase | ~1.1 kg over 12 months (older adults) | Plateau by 6-12 months |
| Insulin sensitivity | Decreased (Quicki index falls) | Manifests within months |
| Cortisol | +47 nmol/L (Nass 2008) | Sustained |
| Appetite | Increased (subjective and objective) | Within days |
| Body weight | +2.7 kg over 12 months (older adults) | Progressive |
The pulsatility argument
One pharmacological point worth understanding clearly, because it gets repeated as a marketing line: MK-677 does preserve the natural pulsatile pattern of GH secretion, unlike injectable rhGH which produces a single high-amplitude pulse after each injection.
Pulsatility matters for several reasons. It's how the body's tissue responses are calibrated to GH — receptors desensitize after sustained exposure but reset between pulses. It's also how IGF-1 production gets regulated, and how the GH/IGF-1 axis interacts with insulin sensitivity, glucose homeostasis, and other systems.
Is preserved pulsatility actually clinically advantageous over rhGH? The honest answer is "probably, but not in a way that's been definitively demonstrated." The studies that would directly compare clinical outcomes (long-term, head-to-head) haven't been done. The argument is mechanistic plausibility rather than measured advantage.
Human Evidence: The Nass 2008 Trial
This is the cornerstone study, and it's worth examining closely because it's the strongest human dataset and most representative of what MK-677 actually does in people.
Design
Two-year, double-blind, randomized, placebo-controlled, modified-crossover trial in 65 healthy older adults (ages 60-81). 43 randomized to MK-677 25 mg daily; 22 to placebo. Conducted at the University of Virginia and three other US sites. Funded by NIH and Merck (Merck provided the drug).[2]
Primary findings (12 months)
Hormonal effects:
- GH levels increased 1.8× from baseline
- IGF-1 levels increased 1.5×, reaching young-adult range
- Pulsatile pattern of GH secretion preserved
Body composition:
- Fat-free mass: +1.1 kg in MK-677 vs -0.5 kg in placebo (P<0.001)
- Body cell mass: +0.8 kg in MK-677 vs -1.0 kg in placebo
- Total body water and intracellular water increased (consistent with anabolic effects)
- Limb fat increased more in MK-677 group (+1.1 kg vs +0.24 kg)
- Body weight increased 2.7 kg in MK-677 group vs 0.8 kg in placebo
- Abdominal visceral fat: no significant difference between groups
- Total fat mass: no significant difference between groups
Functional outcomes:
- Increased fat-free mass did not result in changes in strength or function.
This last point is critical and often glossed over. The compound added muscle tissue but didn't make participants meaningfully stronger or better-functioning. For an indication targeting frailty in older adults, this is a meaningful limitation.
Metabolic effects:
- Fasting blood glucose increased
- HbA1c increased
- Quicki index of insulin sensitivity decreased
- LDL cholesterol decreased slightly
- Cortisol rose (+47 nmol/L)
At 24 months (subset analysis):
- Hormonal and body composition effects persisted
- Fasting glucose changes had normalized
Adverse effects:
- Increased appetite (most common)
- Transient, mild lower-extremity edema
- Muscle pain
- No significant increase in serious adverse events
- No newly detected malignancies in the trial period
What this trial actually shows
A nuanced reading: MK-677 reliably does what its mechanism predicts. GH and IGF-1 go up. Body composition shifts toward more lean tissue. Most participants tolerate it adequately.
But the functional payoff is smaller than the body composition numbers suggest, the metabolic costs (insulin sensitivity in particular) are real, and the trial wasn't designed to capture longer-term outcomes that matter most for an aging population.
Other Human Trials
The Nass 2008 trial is the most-cited, but several other human studies exist:
- Svensson et al. 1998 (obesity, 2-month): GH secretion, fat-free mass, and energy expenditure all increased in obese adults.
- GH-deficient adults: MK-677 raised GH and IGF-1, though effects were generally less robust than in GH-replete subjects.
- GH-deficient children (the LUM-201 indication): A subset of pediatric GHD patients respond to MK-677, leading to the orphan drug designation and ongoing LUMOS Pharma development program. The trick is identifying which children are "secretagogue-responsive" — work on predictive biomarkers continues.
- Hip fracture recovery: This is the trial that contributed to Merck halting broader development. MK-677 in older hip fracture patients was associated with increased adverse events including congestive heart failure. The compound's fluid retention effect, while typically mild in healthier populations, became more consequential in patients with reduced cardiovascular reserve.
- Catabolic states / cancer cachexia: Some small studies; results mixed.
The cumulative human safety database for MK-677 is substantial by the standards of compounds in this review series — likely several thousand patient-exposures across two decades of clinical development.
Regulatory Status
| Jurisdiction | Status |
|---|---|
| FDA (USA) | ❌ Not approved. Orphan Drug Designation (June 2017) for pediatric growth hormone deficiency (as LUM-201). |
| EMA (Europe) | ❌ Not approved. Orphan Drug Designation (June 2017) for pediatric GHD. |
| WADA | ⚠️ Prohibited — Class S2 (peptide hormones, growth factors, and related substances, despite being a non-peptide). Detection methods including hair testing are now available.[8] |
| Compounding pharmacies (US) | Not approved for compounding; not a designated bulk drug substance |
| Consumer access | Predominantly grey-market "research chemical" channels |
The Orphan Drug Designation is worth understanding clearly. ODD is granted to compounds being developed for rare conditions (in the US, fewer than 200,000 affected patients). It provides regulatory and commercial incentives for development but is not an approval. LUM-201 is in ongoing clinical development; whether it will receive full FDA approval for pediatric GHD is still pending.
The WADA prohibition predates the structural identification of MK-677 as a non-peptide — anti-doping classification follows mechanism, not chemistry. The compound elevates GH and IGF-1, which is what S2 covers. Recent hair-testing methods can detect MK-677 use months after discontinuation, with quantitative LC-MS/MS able to identify both single-dose exposure (1.3 pg/mg at 4 weeks post-exposure) and chronic use (224 pg/mg in a user taking 60×10mg over 90 days).[8]
Safety: What's Documented
This is where MK-677 differs from most compounds in this review series — there's actually a substantial documented safety profile to discuss, not just theoretical concerns.
Insulin sensitivity decline
This is the most consistently documented metabolic effect. Across multiple trials:
- Fasting glucose rises
- HbA1c rises
- Insulin sensitivity indices (Quicki, HOMA-IR) decline
- Effects are dose-dependent
The mechanism is clear: GH directly antagonizes insulin action at the cellular level, and chronic GH elevation produces measurable insulin resistance. This is a known property of all growth hormone-elevating therapies, including injectable rhGH.
For an otherwise metabolically healthy young adult, the effect may be modest and reversible. For someone with prediabetes, type 2 diabetes, metabolic syndrome, or strong family history thereof, the effect is more consequential.
Fluid retention
GH elevation produces sodium and water retention. In trials, this manifested as mild lower-extremity edema in some participants. For most users this is cosmetic. For users with congestive heart failure, kidney disease, or compromised cardiovascular reserve, it can be clinically significant — which is exactly what surfaced in the Merck hip fracture trial.
Cortisol elevation
GHSR-1a activation increases ACTH and therefore cortisol. The +47 nmol/L rise documented in Nass 2008 is modest but real and sustained. Chronic mild cortisol elevation has implications for glucose tolerance (worsens insulin sensitivity further), bone health (decreases bone mineral density over time), immune function, and mood.
Increased appetite and weight gain
The body composition effect of MK-677 is partly anabolic (real muscle tissue gain) and partly accretive (increased food intake leading to general weight gain, including fat). For users targeting body recomposition rather than absolute mass gain, this is a counterproductive effect.
Potential cardiovascular concerns
Two threads converge:
- Fluid retention contributes to volume load on the heart
- The Merck hip fracture trial showed increased CHF events at active doses
For young, healthy adults the cardiovascular risk profile is probably modest. For older adults, anyone with existing cardiovascular disease, or those with reduced ejection fraction, the risk is substantive.
Cancer biology
GH and IGF-1 are growth-promoting hormones. There's a substantial epidemiological literature linking elevated IGF-1 to increased risk of certain cancers (particularly prostate, breast, colorectal). Whether the magnitude of IGF-1 elevation from MK-677 (~1.5×, into young-adult range) translates to clinically meaningful cancer risk is uncertain. The trials are too short and underpowered for cancer endpoints. The Nass 2008 trial reported no newly detected malignancies during the study period, but a 2-year trial in 65 participants cannot detect modest cancer risk changes.
For anyone with personal or family history of hormone-sensitive cancers, this is a meaningful unresolved question.
Other documented effects
- Numbness and tingling (peripheral nerve effects, occasionally reported)
- Mild aches and joint pains (similar to rhGH)
- Vivid dreams (related to slow-wave sleep changes)
- Lethargy in some users
- Mild blood pressure changes
| Safety area | Status |
|---|---|
| Insulin resistance | ⚠️ Documented; dose-dependent; reversible on discontinuation |
| Fluid retention | ⚠️ Documented; mild in healthy users |
| Cortisol elevation | ⚠️ Documented; sustained at +47 nmol/L magnitude |
| Cardiovascular safety | ⚠️ Concern in cardiac-compromised populations (Merck hip fracture trial) |
| Cancer risk | ⚠️ Theoretical concern via IGF-1 elevation; not directly characterized |
| Sleep architecture | ✓ Generally favorable (more slow-wave sleep) |
| Bone biomarkers | ⚠️ Mixed; increased turnover but unclear net effect |
| Appetite/weight gain | ⚠️ Documented; can be substantial |
| Vendor material quality | ⚠️ Variable; grey-market standards |
Common Misconceptions
"It's a peptide."
It isn't. MK-677 is a small spiropiperidine molecule developed by Merck's medicinal chemistry program. The frequent grouping with BPC-157, TB-500, and other actual peptides on vendor websites is incorrect labeling. Pharmacokinetically, structurally, and metabolically, MK-677 is an orally active small molecule.
"It's safer than injectable HGH because it works through your own pituitary."
This is partially true and substantially misleading. MK-677 does preserve natural GH pulsatility, which has theoretical advantages over single-pulse exogenous HGH. But the downstream effects on insulin sensitivity, fluid retention, IGF-1 elevation, and cortisol are largely the same as with exogenous GH, because the elevated hormones produce the same tissue effects regardless of source. "Endogenous" doesn't equal "safer."
"It builds muscle."
It produces measurable increases in fat-free mass. Whether that translates to functional muscle (in the sense of increased strength and athletic performance) is less clear. The Nass 2008 trial specifically documented increased fat-free mass without corresponding increases in strength or physical function. Some of the "muscle" gain may be intracellular water and other non-contractile tissue.
"There's lots of research, so it must be safe."
There is substantial research, and that research documents real safety concerns: insulin resistance, fluid retention, cortisol elevation, and the Merck hip fracture trial signal. "Well-studied" doesn't mean "shown to be safe" — in MK-677's case, the studies have shown specific, predictable adverse effects that were significant enough to halt mainstream pharmaceutical development.
"It's an SARM."
It isn't. SARMs (Selective Androgen Receptor Modulators) work through androgen receptors and affect testosterone-related pathways. MK-677 works through the ghrelin receptor and affects GH/IGF-1. The compounds are frequently sold by the same vendors and stacked by users, but mechanistically they're unrelated.
"It restores you to young adult hormone levels, which must be optimal."
The Nass 2008 study showed MK-677 raises older adults' GH/IGF-1 to young-adult ranges. Whether achieving young-adult hormone levels in older bodies is optimal is a separate question. The decline of GH with age may be physiologic adaptation rather than pure deficiency, and "more hormone is better" doesn't necessarily hold.
Frequently Asked Questions
What's the current status of LUM-201?
LUMOS Pharma continues developing MK-677 (as LUM-201) specifically for pediatric growth hormone deficiency. Phase 2 trials and ongoing work on predictive biomarkers to identify responsive patients are central to the program. Full FDA approval for pediatric GHD remains the goal but timing is uncertain.
Why did Merck stop developing it?
The mainstream pharmaceutical narrative isn't fully transparent, but several factors clearly contributed: the lack of functional improvement despite lean mass gains, the insulin sensitivity signal, the hip fracture trial adverse events including CHF, and the difficult regulatory positioning for an aging-related indication (FDA generally resistant to approving drugs for "aging" without disease-specific endpoints). The economic case for a broader indication was insufficient given these complications.
Is the IGF-1 elevation cancer risk meaningful?
For short-term use in healthy individuals without cancer history, the risk is probably modest but uncharacterized. For users with personal or family history of hormone-sensitive cancers (prostate, breast, colorectal), the risk-benefit calculation is meaningfully different. Long-term users should weigh this carefully against their personal medical context.
How does MK-677 compare to peptide GH secretagogues?
The most common comparison is to injectable peptide secretagogues like ipamorelin, GHRP-2, or combinations like CJC-1295 + Ipamorelin. These peptides work through the same GHSR-1a receptor as MK-677 (in the case of ipamorelin and the GHRPs) or through GHRH receptor (in the case of CJC-1295 and sermorelin). The pharmacological differences: MK-677 is oral with a longer half-life producing sustained activation; the peptides are injectable, shorter-acting, and typically dosed multiple times per day. The hormonal endpoints and side-effect profiles overlap considerably, but the practical use profiles differ.
How does it compare to direct GH therapy?
Direct HGH therapy produces large, single-pulse hormone exposure; MK-677 preserves pulsatility but with elevated baseline. Each approach has different pharmacokinetic profiles and somewhat different side-effect distributions, but the core risks (insulin resistance, fluid retention, cancer concerns) are common to all three.
Why is the lethargy/sleep effect so prominent in user reports?
The slow-wave sleep increase is real and documented. For some users this manifests as deeper, more restorative sleep; for others as next-day grogginess. Individual responses to GH and to changes in sleep architecture vary substantially. Morning dosing reduces some of these effects but doesn't eliminate them, given the compound's half-life.
Can the insulin resistance be managed?
In healthy individuals without underlying glucose dysregulation, the effect is typically modest and reversible on discontinuation. Some clinicians use co-administration with metformin or attentive carbohydrate management to mitigate the effect during use. None of this is formally validated for MK-677 specifically, and individual responses vary.
Key Takeaways
- MK-677 (ibutamoren) is a non-peptide, orally active selective agonist of the ghrelin receptor (GHSR-1a), developed by Merck in the early 1990s as an oral alternative to injectable growth hormone therapy.
- The compound reliably raises GH and IGF-1 levels in humans to young-adult ranges, while preserving the natural pulsatile pattern of GH secretion. This hormonal effect is the most consistently documented finding across all clinical trials.
- ⚠️ The Nass 2008 trial in Annals of Internal Medicine — the strongest human evidence — showed clear hormonal effects and increased fat-free mass (1.1 kg over 12 months) but no improvement in strength or physical function despite the body composition change.[2]
- ⚠️ Documented adverse effects include decreased insulin sensitivity (rising fasting glucose and HbA1c), fluid retention (mild edema), cortisol elevation (+47 nmol/L), increased appetite and weight gain, and joint discomfort. These are not theoretical — they're measured in well-controlled trials.
- ⚠️ A Merck-sponsored hip fracture trial showed increased adverse events including congestive heart failure in older patients on MK-677-equivalent doses. This trial was a significant factor in Merck's decision to halt broader development.
- The IGF-1 elevation associated with MK-677 raises theoretical cancer concerns (epidemiologically, elevated IGF-1 correlates with increased risk of several hormone-sensitive cancers). Direct cancer endpoints have not been adequately characterized in the trials.
- Regulatorily, MK-677 is not approved anywhere despite having received Orphan Drug Designation from both FDA and EMA in 2017 for pediatric growth hormone deficiency. Development continues as LUM-201 (LUMOS Pharma) for that specific indication only.
- WADA-prohibited under Class S2. Hair-testing detection methods are now established. For tested athletes, use is a guaranteed violation.
- Despite frequent labeling as a "peptide" in research-chemical channels, MK-677 is a small molecule. The mislabeling reflects marketing conventions rather than chemical reality.
- ⚠️ Honest framing: MK-677 has the most substantial human evidence base of nearly any compound in this review series, and that evidence is mixed. The hormonal effects are real. The body composition effects are real but modest. The functional benefits are smaller than expected. The metabolic and cardiovascular safety signals are documented and substantive. This is one of the relatively rare cases where the limiting factor isn't absence of human data — it's the data itself, which suggests a more complicated risk-benefit picture than the marketing implies.
Related Compounds
For peptide-based growth hormone secretagogues that work through the same or complementary pathways, the most direct comparisons are Ipamorelin (selective GHSR-1a agonist, peptide form) and the combination CJC-1295 + Ipamorelin stack. For the broader landscape of growth hormone, GHRH analogs, and endocrine-axis compounds, see the Endocrine Research category.
References
Foundational chemistry and discovery
- Patchett AA, Nargund RP, Tata JR, et al. Design and biological activities of L-163,191 (MK-0677): a potent, orally active growth hormone secretagogue. Proc Natl Acad Sci USA. 1995;92(15):7001-7005.
Pivotal clinical trial
- Nass R, Pezzoli SS, Oliveri MC, Patrie JT, Harrell FE Jr, Clasey JL, et al. Effects of an oral ghrelin mimetic on body composition and clinical outcomes in healthy older adults: a randomized trial. Ann Intern Med. 2008;149(9):601-611. PMID: 18981485
- Blackman MR. Use of growth hormone secretagogues to prevent or treat the effects of aging: not yet ready for prime time (editorial). Ann Intern Med. 2008;149(9):663-664.
Other clinical trials
- Svensson J, Lönn L, Jansson JO, et al. Two-month treatment of obese subjects with the oral growth hormone (GH) secretagogue MK-677 increases GH secretion, fat-free mass, and energy expenditure. J Clin Endocrinol Metab. 1998;83(2):362-369.
- Murphy MG, Plunkett LM, Gertz BJ, et al. MK-677, an orally active growth hormone secretagogue, reverses diet-induced catabolism. J Clin Endocrinol Metab. 1998;83(2):320-325.
Mechanism and structure
- Müller TD, Nogueiras R, Andermann ML, et al. Ghrelin. Mol Metab. 2015;4(6):437-460.
- Liu H, Sun D, Myasnikov A, et al. Structural basis of human ghrelin receptor signaling by ghrelin and the synthetic agonist ibutamoren. Nat Commun. 2021;12(1):6410. doi: 10.1038/s41467-021-26735-5
Safety reviews
- Sigalos JT, Pastuszak AW. The safety and efficacy of growth hormone secretagogues. Sex Med Rev. 2018;6(1):45-53.
Anti-doping
- Knowing the minimal detectable dose can facilitate the interpretation of a hair test result: II. Case example with ibutamoren (MK-677), a growth hormone secretagogue. Clin Chim Acta. 2025.
Pediatric development
- Bright GM, Do MT, McKew JC, Blum WF, Thorner MO. Development of a predictive enrichment marker for the oral GH secretagogue LUM-201 in pediatric growth hormone deficiency. J Endocr Soc. 2021;5(5):bvab030.
Regulatory
- FDA Orphan Drug Designation database — Ibutamoren (LUM-201) for pediatric growth hormone deficiency (June 2017).
- EMA Orphan Drug Designation — Ibutamoren for pediatric growth hormone deficiency (June 2017).
Key investigators
- Arthur A. Patchett, PhD — Merck Research Laboratories. Lead chemist on MK-677 discovery and characterization.
- Roy G. Smith, PhD — Merck (formerly). Senior author on much of the ghrelin receptor/GHSR pharmacology, including ghrelin receptor identification.
- Michael O. Thorner, MD — University of Virginia. Principal investigator on the Nass 2008 trial; long-time leader in GH/IGF-1 axis research.
- Ralf Nass, MD — University of Virginia. Lead author of the 2008 Annals of Internal Medicine trial.
- LUMOS Pharma — Current developer of MK-677 (as LUM-201) for pediatric growth hormone deficiency.
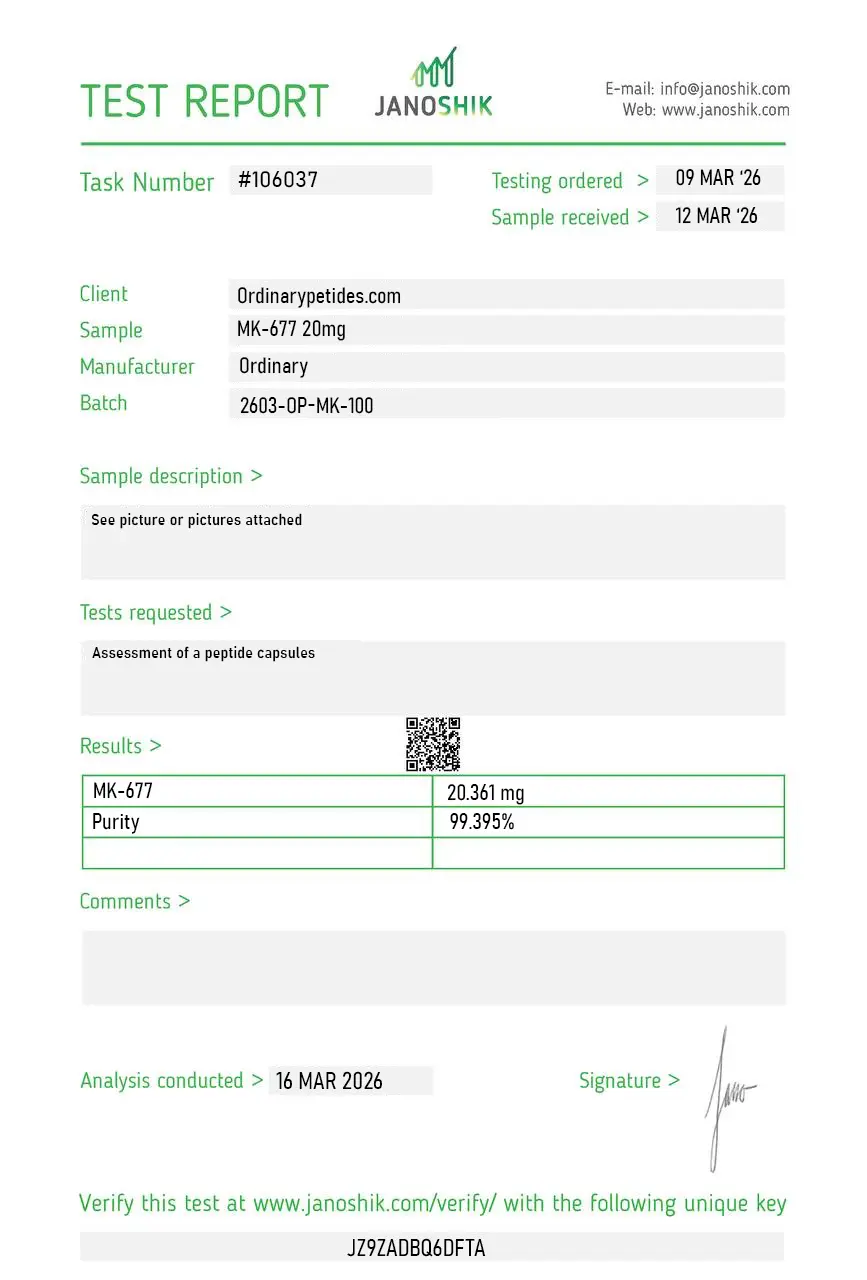
Certificate of Analysis
An independent test report is available for MK-677 20mg. This report provides batch-level documentation and analytical verification information for research reference.
MK-677 — also known as ibutamoren, ibutamoren mesylate, MK-0677, LUM-201, L-163,191, and by the former tentative brand name Oratrope — is a synthetic, orally active, non-peptide small-molecule agonist of the ghrelin receptor (GHS-R1a). It was developed by Merck & Co. and later licensed to other research organizations. It is classified as a growth hormone secretagogue (GHS) — a compound that stimulates the pituitary gland to secrete more endogenous growth hormone rather than supplying exogenous GH directly. Its molecular weight is 624.77 g/mol and it is notable for its 24-hour half-life, which is significantly longer than peptide-based growth hormone secretagogues and allows once-daily oral administration in research protocols.
MK-677 binds selectively to the growth hormone secretagogue receptor type 1a (GHS-R1a) — the same receptor activated by ghrelin, the endogenous orexigenic hormone produced primarily in the stomach. A 2021 structural biology study published in Nature Communications resolved the molecular basis of GHS-R1a signaling by both ghrelin and ibutamoren using cryo-electron microscopy, confirming that MK-677 activates the receptor through the Gq/11 and Gi/o G protein signaling pathways. The mechanism involves dual-site stimulation of GH release: direct activation of somatotroph cells in the anterior pituitary, and amplification of hypothalamic GHRH (growth hormone-releasing hormone) release. This dual action produces a synergistic GH response greater in magnitude than GHRH stimulation alone. Importantly, GH release remains pulsatile and subject to negative feedback from IGF-1 — a key mechanistic distinction from exogenous recombinant GH administration, which suppresses endogenous pituitary activity.
Multiple clinical studies have confirmed that MK-677 produces sustained, dose-dependent increases in both GH secretion and IGF-1. A 2019 trial published in the Journal of Clinical Endocrinology & Metabolism reported a 97% increase in GH secretion compared to baseline. In a 2-year double-blind, randomized, placebo-controlled trial in healthy older adults aged 60–81 (Nass et al., 2008, Annals of Internal Medicine), MK-677 at 25 mg/day sustained increases in both 24-hour mean GH pulse amplitude and IGF-1 levels to those typically seen in young adults. The pulsatile secretory pattern was preserved throughout, and IGF-1 feedback prevented supra-therapeutic GH accumulation. A separate study in 22 hemodialysis patients found IGF-1 was 1.76-fold higher in the MK-677 arm versus 1.07-fold in placebo, confirming the effect extends to populations with compromised renal function.
The most rigorous body composition data comes from the 2-year Nass et al. trial. MK-677 increased fat-free mass by 1.6 kg relative to placebo — with a concurrent increase in intracellular water reflecting body cell mass — without a significant change in total fat mass or visceral abdominal fat. A 12-month trial in healthy older adults (25 mg/day) found fat-free mass increased by 1.1 kg with no significant strength or functional improvement despite the mass gain. An earlier study found a 40% increase in serum IGF-1 alongside sustained increases in lean body mass and a transient elevation in basal metabolic rate. Across the clinical literature, MK-677 consistently increases fat-free mass in older adults and individuals with catabolic conditions, though the translation of mass gains into functional strength improvements has not been consistently demonstrated.
Bone-related research represents one of MK-677's more consistent findings across clinical studies. The compound increases markers of both bone formation — including osteocalcin and bone-specific alkaline phosphatase — and bone resorption, indicating active stimulation of the full bone remodeling cycle rather than isolated formation. A systematic review in the context of sarcopenia research found that MK-677 addressed three key contributors to the condition simultaneously: reduced GH secretion, fat-free mass loss, and inadequate food intake via its ghrelin-mimetic appetite-stimulating properties. In hemodialysis patients — a population with significantly impaired bone metabolism — MK-677 produced the IGF-1 elevations described above, which are mechanistically relevant to bone density given IGF-1's role in osteoblast differentiation and function. Long-term bone density outcomes in randomized controlled trials remain limited in number.
A frequently cited early finding is a 1997 study by Copinschi et al. examining MK-677's effects on sleep architecture in eight young subjects. The study found that MK-677 administration improved both the quality and duration of sleep — specifically increasing slow-wave sleep (SWS, or deep sleep) duration. The proposed mechanism involves GHS-R1a activation in brain regions governing sleep-wake regulation, and the known relationship between GH pulsatility and slow-wave sleep — GH is normally secreted in large pulses during deep sleep, and GHS-R1a stimulation may reinforce this GH-sleep coupling. This finding has contributed to research interest in MK-677 for age-related sleep architecture deterioration, which is characterized by reduction in SWS. The finding derives from a small, short-duration study and has not been replicated in large randomized controlled trials.
Clinical trials have identified several consistent safety concerns. The most significant metabolic finding is reduced insulin sensitivity and elevated fasting blood glucose — in the Nass et al. trial, mean serum glucose increased by approximately 5 mg/dL in the MK-677 arm. This is mechanistically attributable to GH's counter-regulatory effects on insulin signaling, which are well-established endocrinologically. Fluid retention and peripheral edema are commonly reported, consistent with GH's sodium-retaining effects. Appetite stimulation — a direct consequence of GHS-R1a activation in the hypothalamus — is significant, comparable in magnitude to GHRP-6. Cortisol elevation was not significantly observed — a distinction from some other GH secretagogues. A 2024 FDA warning flagged adulterated products sold online claiming to contain ibutamoren, raising product quality and safety concerns in unregulated sourcing contexts. Long-term cardiovascular safety data beyond 2 years in healthy populations has not been established.
MK-677 and peptide secretagogues such as GHRP-6, GHRP-2, Ipamorelin, and CJC-1295 all stimulate endogenous GH release but differ significantly in administration route, pharmacokinetics, and receptor desensitization profiles. Peptide secretagogues require subcutaneous injection, have short half-lives (minutes to a few hours), and require multiple daily administrations to sustain GH elevation. MK-677 is orally bioavailable with a 24-hour half-life, allowing once-daily oral administration — a practically significant distinction for longitudinal research protocols. On receptor desensitization, MK-677 does not produce significant GHS-R1a desensitization at therapeutic research concentrations across 6–12 months of documented use — a property attributed to its non-peptide binding characteristics and the preservation of pulsatile GH secretion through IGF-1 negative feedback. GHRP-6 produces greater appetite stimulation than Ipamorelin or Hexarelin; MK-677's appetite stimulation falls in a comparable range to GHRP-6 given its ghrelin-mimetic mechanism.
Yes. MK-677 was investigated in a randomized clinical trial for Alzheimer's disease, published in Neurology (2008) — based on the hypothesis that IGF-1 elevation might modulate amyloid-beta dynamics or support neuronal survival. The trial found no clinical effect on Alzheimer's disease progression, representing a negative result for that specific neurological indication. Separately, the compound's activity at GHS-R1a in the CNS — the receptor plays established roles in modulation of stress and anxiety, regulation of dopamine signaling, and reward pathway function, as characterized in the 2021 Nature Communications structural study — has maintained broader neurological research interest. A GHS-R1a inverse agonist (PF-5190457) is under clinical investigation for alcohol use disorder, highlighting the receptor's relevance to addiction neuroscience. Cognitive effects of MK-677 specifically remain an underexplored research area with limited controlled data.
MK-677 is classified as an Investigational New Drug (IND) in the United States and has not received FDA approval for any clinical indication. It carries no approved brand name in any major market, though Oratrope was a former tentative designation. The FDA issued warnings in 2024 regarding adulterated products marketed online that contained undisclosed ibutamoren, flagging contamination and mislabeling risks in the research chemical supply chain. MK-677 is prohibited by WADA under the Prohibited List and also appears on the Department of Defense Prohibited Dietary Supplement Ingredients List. It is available from research chemical suppliers as a Research Use Only (RUO) reference material for qualified researchers. Despite more than two decades of clinical investigation — including multiple human randomized controlled trials — MK-677 has never advanced to regulatory submission for any indication, making it one of the most clinically studied compounds that remains entirely outside the approved pharmaceutical framework.





